
Abstract
Design: Prospective 2-year survey from 1 February 1997 to 31 January 1999.
Objectives: To compare the route from injury to rehabilitation, and the outcome of care in a large sample of traumatic (T) and nontraumatic (NT) spinal cord lesion (SCL) patients at their ‘first admission’.
Setting: T and NT SCI patients consecutively admitted to 37 SCL centres in Italy.
Method: Data were recorded on simple, computerised, closed-question forms, which were Centrally collected and analysed. Descriptive and inferential analysis was conducted to define the characteristics and compare the T and NT populations, and to identify correlations among the variables examined: time from the event to admission (TEA); pressure sores (PS) on admission; length of stay (LoS) and destination on discharge.
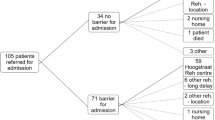
Results: A total of 1014 SCL patients, 67.5% with a lesion of T and 32.5% of NT aetiology were analysed. The subjects in the T group were younger (median 34 versus 58 years), with higher probability of cervical involvement (OR 2.47, CI 1.8–3.4) and completeness of the lesion (OR 3.0, CI 2.3–4.0), shorter median TEA(37 versus 64 days, P<0.0001) and less frequent admission from home (3.6 versus 17.4%) compared to the NT group. TEA and PS on admission were analysed as indicators of the efficacy of the courses from injury to rehabilitation. Longer TEA was reported for people with NT aetiology, admitted to rehabilitation centre (RC), not locally resident, transferred from certain wards and to a lesser degree female subjects and those with complications on admission. PS were associated to completeness of lesion, longer TEA, admission to RC, nonlocal residence and coming from general intensive care units, or general surgery wards. Median LoS was 99 days (mean 116 and range 0–672), and was statistically shorter in the NT group (122 versus 57 median, P<0.00001). Upon discharge, bladder and bowel autonomy were, respectively, obtained in 68.1 and 64.5% of the whole population without significant difference between the T and NT groups. A total of 80.2% of patients were discharged home and the following factors: not living alone, being discharged after longer LoS, having sphincterial autonomy and no PS, were all independent predictors of outcome.
Conclusion: There are important obstacles in the admission route to rehabilitation facilities, greater for NT, as longer TEA and more complications on admission testify. Moreover, the LoS is shorter for NT population. Our findings suggest that rehabilitation outcome could be improved through an early multidisciplinary approach and better continuity between acute and rehabilitation care, especially for the ‘neglected’ NT SCL patients.
Similar content being viewed by others


Log in or create a free account to read this content
Gain free access to this article, as well as selected content from this journal and more on nature.com
or
References
McMillan BS, Silver JR . Extension injuries of the cervical spine resulting in tetraplegia. Injury 1987; 18: 224–233.
DeVivo MJ, Kartus PL, Stover SL, Fine PR . Benefits of early admission to an organised spinal cord injury care system. Paraplegia 1990; 28: 545–555.
Celani MG et al. Spinal cord injury in Italy: a multicenter retrospective study. Arch Phys Med Rehabil 2001; 82: 589–596.
Caldana L, Lucca L . Epidemiological remarks on traumatic spinal cord injures and non traumatic spinal cord diseases in Veneto 1994–1995. Eur Med Phys 1998; 34: 121–124.
Taricco M et al. The social and vocational outcome of spinal cord injury patients. Paraplegia 1992; 30: 214–219.
Aito S . Indagine epidemiologica sulle lesioni midollari in Toscana. Firenze: Azienda Ospedaliera Careggi, 1999.
Nobunaga AI, Go BK, Karunas RB . Recent demographic and injury trends in people served by the model spinal cord injury care systems. Arch Phys Med Rehabil 1999; 80: 1372–1382.
Meinecke FW . What has spinal stabilization contributed for the paraplegic patient? Rehabilitation 1990; 29: 163–168.
Biering-Sørensen E, Pedersen V, Clausen S . Epidemiology of spinal cord lesions in Denmark. Paraplegia 1990; 28: 105–118.
Maharaj JC . Epidemiology of spinal cord paralysis in Fiji: 1985–1994. Spinal Cord 1996; 34: 549–559.
Schönherr MC, Groothoff JW, Mulder GA, Eisma WH . Rehabilitation of patients with spinal cord lesions in The Netherlands: an epidemiological study. Spinal Cord 1996; 34: 679–683.
McKinley WO, Jackson AB, Cardenas DD, DeVivo MJ . Long-term medical complications after traumatic spinal cord injury: a regional model systems analysis. Arch Phys Med Rehabil 1999; 80: 1402–1410.
Carroll CM . Spinal cord injuries in Arkansas due to violence: 1980–1989. Spinal Cord 1997; 35: 341–348.
Exner G, Meinecke FW . Trends in the treatment of patients with spinal cord lesions seen within a period of 20 years in German centers. Spinal Cord 1997; 35: 415–419.
McKinley WO, Seel RT, Hardman JT . Nontraumatic spinal cord injury: incidence, epidemiology, and functional outcome. Arch Phys Med Rehabil 1999; 80: 619–623.
Chen D, Apple Jr DF, Hudson LM, Bode R . Medical complications during acute rehabilitation following spinal cord injury–current experience of the model systems. Arch Phys Med Rehabil 1999; 80: 1397–1401.
Meinecke FW, Exner G . Treatment of patients with spinal cord lesions in Germany 1996–state of the art. Spinal Cord 1997; 35: 411–414.
Schonherr MC, Groothoff JW, Mulder GA, Eisma WH . Rehabilitation of patients with spinal cord lesions in The Netherlands: an epidemiological study. Spinal Cord 1996; 34: 679–683.
Stiens SA, Bergman SB, Goetz LL . Neurogenic bowel dysfunction after spinal cord injury: clinical evaluation and rehabilitative management. Arch Phys Med Rehabil 1997; 78: S86–S102.
Acknowledgements
We thank Dr MJ De Vivo for his useful advice. We are grateful to Hilary Ann Giles (MA) for reviewing the English language of the paper. We also thank the ‘Fondazione M. Taramelli per la ricerca sulla mielolesione’ and Umbria-Regional Health Administration Area for supporting the study with a grant for statistical elaboration.
Author information
Authors and Affiliations
Consortia
Additional information
GISEM group: Guiding Committee and coordinating office: M Franceschini, S Aito, MG Celani, A Citterio, G Finali, D Loria, MC Pagliacci, S Ricci, M Taricco, L Spizzichino and M Zampolini.
Clinica di Neuroriabilitazione, Ancona: L Provinciali, M Danni; SRRF Ospedale Maggiore, Parma: M Boselli, M Franceschini; SRRF Policlinico S Orsola Malpighi, Bologna: M Menarini, M Alianti, L Landi; SRRF Ospedale Bellaria, Bologna: MP Ferrari, G Domenicucci; DRRF Ospedale Maggiore, Bologna: R Piperno, N Battisti; Centro Paraplegici Ospedale di Ostia: DA Fletzer, M Magnini; Centro Medico Cassano Murge, IRCCS, Cassano Murge (BA): R Nardulli, S Calabrese, E Lo Savio; Unità Spinale, Ospedale Careggi, Firenze: S Aito; Casa di Cura ‘Luce sul Mare’, Igea Marina: A Battistini, L Betti; Centro di Riabilitazione ‘Villa Beretta’, Ospedale Valduce, Costamasnaga: N Cellotto, A Lissoni, M Cazzaniga, F Molteni, L Suardi; Ospedale di Riabilitazione di Longone al Segrino, Longone al Segrino: M Almici; Sezione Mielolesi, Magenta: Magnaghi, A Zanollo, MG Zucchi, Tagliabue, P Politi; U.O.R.R.F. Ospedale Civile, Legnano: G Alberti; Istituto di Terapia Fisica e Riabilitazione, Milano: T Redaelli, E Radaelli, C Gallo, F Santagostini; Divisione Paraplegici, CTO, Milano: A Bava, CM Borghi; SRRF Ospedale di Bergamo, Sezione Mozzo, Mozzo: I Ghislandi, M Ceravolo, G Molinero; Centro di Riabilitazione ‘S Stefano’, P Potenza Picena: M Menichetti, M Vallasciani, M Rabuini, G Leone, S Spurio; Servizio Riabilitazione Ortopedica, Padova: D Primon, M Ortolani, Arrigo Baldo, M Gulgelmetto; Ospedale Casati, Passirana di Rho, Passirana di Rho: M Taricco, Ranieri, R Adone, S Di Carlo, A Ferrari, MG Maringelli; Centro Medico Montescano, Pavia: C Pistarini, C Rampulla, A Contardi; Ospedale Villa Rosa, CRF, Pergine Valsugana: R Albertazzi, A Mosetti; Unità Spinale Unipolare, Ospedale Silvestrini, Perugia: MC Pagliacci, G Finali; Unità di Neuroriabilitazione Clinica neurologica Ospedale S Chiara, Pisa: G Stampacchia, B Rossi; SRRF Ospedale SM delle Croci, Ravenna: G Gatta, S Tibaldi, G Cortese; IRCCS Santa Lucia, Roma: G Scivoletto, V Castellano; Unità Spinale Unipolare CTO, Roma: V Santilli, Trigila, M Vinciguerra; Unità Spinale, Sondalo: E Occhi, F Gualzetti; Unità Spinale, Torino: D Loria, V Filipello, S Negri, L Olino; U.O. di Riabilitazione Intensiva Neuromotoria, Trevi: S Baratta, M Zampolini; Centro di Riabilitazione, Trieste: P Di Benedetto, R Piccinino; Istituto di Medicina Fisica e Riabilitazione, Udine: M Saccavini, L Lovati, A Zampa; Reparto di RRF Ospedale ‘Sacro Cuore–Don Calabria’, Negrar: Z Cordioli, G Salvi, R Avesani; UORRF Unita Spinale Ospedale San Bortolo, Vicenza: M Leucci, M Menarini; Centro di Recupero e Rieducazione Funzionale, Villanova d'Arda: S Lotta, D Nicolotti, R Bocchi; Clinica Villa delle Magnolie, Castel Morrone: N Avena, M Esposito, P Sabino, C Limardi; Istituto scienze neurologiche, Catania: A Reggio; Istituto Riabilitazione Neuromotoria, Mezzaselva di Roana: C Strazzabosco, C Guerriero.
Rights and permissions
About this article
Cite this article
Pagliacci, M., Celani, M., Spizzichino, L. et al. Spinal cord lesion management in Italy: a 2-year survey. Spinal Cord 41, 620–628 (2003). https://doi.org/10.1038/sj.sc.3101521
Published:
Issue date:
DOI: https://doi.org/10.1038/sj.sc.3101521
Keywords
This article is cited by
-
Incidence and mortality of spinal cord injury from 2008 to 2020: a retrospective population-based cohort study in the Piedmont Region, Italy
Spinal Cord (2023)
-
Effects of a rehabilitation program for individuals with chronic spinal cord injury in Shanghai, China
BMC Health Services Research (2020)
-
Traumatic spinal cord injury in Italy 20 years later: current epidemiological trend and early predictors of rehabilitation outcome
Spinal Cord (2020)
-
Reliability of the Italian version of the International Spinal Cord Injury Pain Basic Data Set
Spinal Cord (2019)
-
Cross-cultural adaptation and validation of the “Spinal Cord Injury-Falls Concern Scale” in the Italian population
Spinal Cord (2018)
