
Abstract
Study design: Case report.
Objective: To report a rare cause of spinal cord compression.
Setting: University Hospital, Wales, UK.
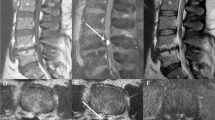
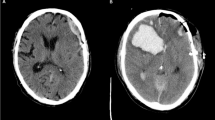
Case report: A 67-year-old gentleman on oral anticoagulation for atrial fibrillation presented with a 4-h history of progressive loss of sensation and weakness in both legs; there was no history of trauma. On examination, he had a flaccid paraplegia with altered sensation in the L1,2,3 dermatomes and complete anaesthesia in the L4,5 distribution. Knee and ankle jerk reflexes were absent, plantars were equivocal and anal sphincter tone was reduced. The patient's international normalized ratio (INR) was 4.1. An MR scan showed an extensive intradural haematoma compressing the cauda equina. The anticoagulation was reversed and an urgent T12-L2 laminectomy was performed; findings were a circumferential haematoma at L1 extending in the anterior canal between T10 and L3. The patient had an uneventful postoperative course generally, but at 1 week there was no neurological recovery.
Conclusion: This case highlights that anticoagulation even when well controlled is not without risk. This is particularly of concern as the number of patients receiving long-term anticoagulation therapy has doubled between 1993 and 1998.
Similar content being viewed by others

Log in or create a free account to read this content
Gain free access to this article, as well as selected content from this journal and more on nature.com
or
References
Calhoun JM, Boop F . Spontaneous spinal subdural haematoma: case report and review of the literature. Neurosurgery 1991; 29: 133–134.
Atrial Fibrillation Investigators. Risk factors for stroke and efficacy of antithrombotic therapy in atrial fibrillation. Analysis of pooled data from five randomized controlled trials. Arch Intern Med 1994; 154: 1449–1457.
Rose P . Audit of anticoagulant therapy. J Clin Pathol 1996; 49: 5–9.
Odén A, Fahlén M . Oral anticoagulation and risk of death: a medical report linkage study. Br Med J 2002; 325: 1073–1075.
British Committee for Standards in Haematology. BCSH Guidelines on oral anticoagulation, 3rd ed. Br J Haematol 1998; 101: 37–387.
Swann KW, Ropper AH, New PFJ, Poletti CE . Spontaneous spinal subarachnoid haemorrhage and subdural haematoma. J Neurosurg 1984; 61: 975–980.
Rader JP . Chronic subdural haematoma of the spinal canal: report of a case. N Eng J Med 1955; 253: 374–376.
Smith RA . Spinal subdural haematoma, neurilemmoma and acute transverse myelopathy. Surg Neurol 1985; 23: 367–370.
Groen RJM, van Alpen HAM . Operative treatment of spontaneous spinal epidural haematomas: a study of the factors determining postoperative outcome. Neurosurgery 1996; 39: 494–508.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Miller, D., Ray, A. & Hourihan, M. Spinal subdural haematoma: how relevant is the INR?. Spinal Cord 42, 477–480 (2004). https://doi.org/10.1038/sj.sc.3101591
Published:
Issue date:
DOI: https://doi.org/10.1038/sj.sc.3101591
