
Abstract
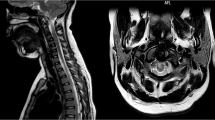
Study design: Case study on a 45-year-old female with progressive weakness and paresthesias in her lower extremities and a magnetic resonance image of an intramedullary mass at the level of C5–6 and a Klippel–Feil (KF) deformity ventral to the lesion.
Objective: Present an interesting case of an intramedullary mass coexisting with a ventral KF deformity with review of the medical literature on intramedullary masses and cervical spine biomechanics.
Setting: New York city, New York, USA.
Methods: Case study with discussion of neurosurgical and neuropathological findings and review of the literature.
Results: The patient underwent open neurosurgical excisional biopsy of the intramedullary mass which revealed a non-neoplastic inflammatory mass that slowly resolved with medical management.
Conclusions: While no definitive etiology was found in this case we offer two interesting mechanisms: (1) maldevelopment of the cervical spine or (2) this inflammatory mass is in response to an abnormal motion at the level of the Klippel–Feil.
Similar content being viewed by others


Log in or create a free account to read this content
Gain free access to this article, as well as selected content from this journal and more on nature.com
or
References
Sheehan JP, Sheehan JM, Lopes MB, Jane Sr JA . Thoracic diastematomyelia with concurrent intradural epidermoid spinal cord tumor and cervical syrinx in an adult. Case Report. J Neurosurg 2002; 97: 231–234.
Steinbok P . Dysraphic lesions of the cervical spinal cord. Neurosurg Clin N Am 1995; 6: 367–376.
Whittle IR, Besser M . Congenital neural abnormalities presenting with mirror movements in a patient with Klippel–Feil syndrome. Case Report. J Neurosurg 1983; 59: 891–894.
Nagashima H, Morio Y, Teshima R . No neurological involvement for more than 40 years in Klippel–Feil syndrome with severe hypermobility of the upper cervical spine. Arch Orthop Trauma Surg 2001; 121: 99–101.
Kinne RW, Brauer R, Stuhlmuller B, Palombo-Kinne E, Burmester G . Macrophages in rheumatoid arthritis. Arthritis Res 2000; 2: 189–202.
Blight AR . Macrophages and inflammatory damage in spinal cord injury. J Neurotrauma 1992; 9: 83–91.
Benzel EC . Biomechanics of Spine Stabilization. American Association of Neurological Surgeons: Rollins Meadows, Illinois, USA 2001, pp 36–37.
Lee M, Epstein FJ, Rezai AR, Zagzag D . Nonneoplastic intramedullary spinal cord lesions mimicking tumors. Neurosurgery 1998; 43: 788–794.
Vaquero J, Herrero J, Cabezudo J, Leunda G . Klippel–Feil syndrome with epidural fibroblastoma in the area of vertebral fusion. Arch Neurol 1982; 39: 318–319.
Young WF, Boyko O . Magnetic resonance imaging confirmation of resolution of periodontoid pannus formation following C1/2 posterior transarticular screw fixation. J Clin Neurosci 2002; 9: 434–436.
Vaidyanathan S, Hughes PL, Soni BM, Singh G, Sett P . Klippel–Feil syndrome – the risk of cervical spinal cord injury: case report. BMC Fam Pract 2002; 3: 6.
Kulkarni V, Rajshekhar V, Raghuram L . Accelerated spondylotic changes adjacent to the fused segment following central cervical corpectomy: magnetic resonance imaging evidence. J Neurosurg 2004; 100(1 Suppl): 2–6.
Whiting DM, Chou SM, Lanzieri CF, Kalfas IH, Hardy RW . Cervical neurenteric cyst associated with Klippel–Feil syndrome: a case report and review of the literature. Clin Neuropathol 1991; 10: 285–290.
Cohen-Gadol AA, Zikel OM, Miller GM, Aksamitt A, Scheithauer BW, Krauss WE . Spinal cord biopsy: a review of 38 cases. Neurosurgery 2003; 52: 806–816.
Dias MS, Walker ML . The embryogenesis of complex dysraphic malformations: a disorder of gastrulation? Pediatr Neurosurg 1992; 18: 229–253.
David KM, Copp AJ, Stevens JM, Hayward RD, Crockard HA . Split cervical spinal cord with Klippel–Feil syndrome: seven cases. Brain 1996; 119: 1859–1872.
Epstein NE, Epstein JA, Zilkha A . Traumatic myelopathy in a seventeen-year old child with cervical stenosis (without fracture or dislocation) and a C2–C3 Klippel–Feil fusion. A case report. Spine 1984; 4: 344–347.
Holliday PO, Davis C, Angelo J . Multiple meningiomas of the cervical spinal cord associated with Kippel–Feil malformation and atlantooccipital assimilation. Neurosurgery 1984; 14: 353–357.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Dickerman, R., Colle, K. & Mittler, M. Intramedullary inflammatory mass dorsal to the Klippel–Feil deformity: error in development or response to an abnormal motion segment?. Spinal Cord 42, 720–722 (2004). https://doi.org/10.1038/sj.sc.3101645
Published:
Issue date:
DOI: https://doi.org/10.1038/sj.sc.3101645
Keywords
This article is cited by
-
Cervical split cord malformation (diastematomyelia) with associated Klippel–Feil deformity presenting in adulthood with bimanual synkinesis
European Spine Journal (2024)
-
Cervical spinal cord neurapraxia in the setting of Klippel–Feil anomaly: a diagnostic and therapeutic challenge
Spinal Cord (2007)
