
Abstract
Study design:
Case report.
Setting:
Department of Neurosurgery, Sapporo Azabu Neurosurgical Hospital and Department of Neurosurgery, Hokkaido University Graduate School of Medicine, Sapporo, Japan.
Case report:
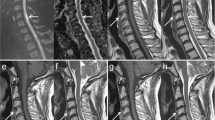
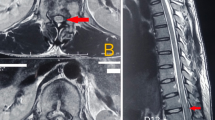
A patient presented to us with complete C4 tetraplegia after a 3-m fall. MRI performed 120 min after his fall showed spinal canal stenosis due to disk protrusion at the C3/4 level without spinal cord signal changes on T1- and T2-weighted images. He underwent laminoplasty between C2 and C6. Intraoperative ultrasound, performed 6 h after his fall, disclosed a hyperechoic lesion at the C3/4 level of the cervical cord; postoperative T2-weighted MRI, obtained at 8 h after his fall, showed high intensity at the same level.
Conclusion:
In patients with cerebral infarction, approximately 6 h between the insult and the acquisition of T2-weighted MRI are required to detect signal changes. We postulate that the time course on MRI scans obtained immediately after spinal cord injury is similar in patients with spinal cord injury and cerebral infarction and suggest that the absence of spinal cord abnormalities in the ultra-early post-injury stage is not always predictive of a good prognosis.
Similar content being viewed by others
Log in or create a free account to read this content
Gain free access to this article, as well as selected content from this journal and more on nature.com
or
References
Yuge I, Shiba K, Ueta T, Ohta H, Mori E, Takemitsu Y . MRI of cervical cord injuries (in Japanese). Sekitsui Sekizui 1997; 10: 423–431.
Maynard Jr FM et al. International standards for neurological and functional classification of spinal cord injury. American Spinal Injury Association. Spinal Cord 1997; 35: 266–274.
Koyamagi I . Spine and spinal cord injury (in Japanese). In: Iwasaki Y and Hida K (eds). The Basic Textbook of Spinal Surgery. Miwa shoten: Tokyo 2006, pp 248–266.
Tator CH, Koyanagi I . Vascular mechanisms in the pathophysiology of human spinal cord injury. J Neurosurg 1997; 86: 483–492.
Ueta T . MRI of spine and spinal cord injuries (in Japanese). MB Orthopaed 1994; 7 (11 Suppl): 59–74.
Gonzalez RG et al. Diffusion-weighted MR imaging: diagnostic accuracy in patients imaged within 6 hours of stroke symptom onset. Radiology 1999; 210: 155–162.
Mohr JP et al. Magnetic resonance versus computed tomographic imaging in acute stroke. Stroke 1995; 26: 807–812.
Minematsu K et al. Effects of a novel NMDA antagonist on experimental stroke rapidly and quantitatively assessed by diffusion-weighted MRI. Neurology 1993; 43: 397–403.
Warach S, Chien D, Li W, Ronthal M, Edelman RR . Fast magnetic resonance diffusion-weighted image of acute human stroke. Neurology 1992; 42: 1717–1723.
Sorensen AG et al. Hyperacute stroke: evaluation with combined multisection diffusion-weighted and hemodynamically weighted echo-planar MR imaging. Radiology 1996; 199: 391–401.
Shinoyama M, Takahashi T, Shimizu H, Tominaga T, Suzuki M . Spinal cord infarction demonstrated by diffusion-weighted magnetic resonance imaging. J Clin Neurosci 2005; 12: 466–468.
Shen H et al. Applications of diffusion-weighted MRI in thoracic spinal cord injury without radiographic abnormality. Int Orthop 2006; 12 (E-pub ahead of print).
van Velthoven V . Intraoperative ultrasound imaging: comparison of pathomorphological findings in US versus CT, MRI and intraoperative findings. Acta Neurochir 2002; 85 (Suppl): 95–99.
Aoyama T, Terasaka S, Kashiwazaki D, Ushikoshi S, Nunomura M . Usefulness of intraoperative ultrasound in neurosurgery (in Japanese). Neurosonology 2005; 18: 63–68.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Aoyama, T., Hida, K., Akino, M. et al. Ultra-early MRI showing no abnormality in a fall victim presenting with tetraparesis. Spinal Cord 45, 695–699 (2007). https://doi.org/10.1038/sj.sc.3102014
Published:
Issue date:
DOI: https://doi.org/10.1038/sj.sc.3102014
