
Abstract
Background
Metabolic bone disease of prematurity (MBD) is a common problem among preterm infants. Our previous study identified cholestasis as an important risk factor for the development of MBD. We conducted this study to determine the vitamin D status in preterm infants with MBD and cholestasis.
Methods
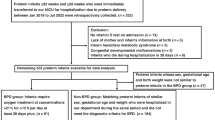
We retrospectively reviewed medical record of preterm infants evaluated in NICU at Holtz Children’s/Jackson Memorial Hospital between June 2014 and May 2016. Demographic, biochemical data, and vitamin D intake were collected and analyzed.
Results
We identified 58 preterm infants (median gestational age 25 weeks) with MBD during this period. Twenty five infants also developed cholestasis. Median serum 25-hydroxyvitamin D level at the time of diagnosis of MBD was similar in cholestasis (C), (29.1 ng/ml, IQR 24.4–33.5), and non-cholestasis (NC), (28.7 ng/ml, IQR 22.7–34.6), group (p = 0.41). At the second measurement, average 6 weeks after the first measurement; median serum 25-hydroxyvitamin D level was lower (p = 0.02) in the C group (31.2 ng/ml, IQR 23.0–38.8) than in the NC group (36.5 ng/ml, IQR 28–45). However, the actual percentage of infants with vitamin D deficiency was similar in both the groups.
Conclusion
Most preterm infants with cholestasis and MBD had normal vitamin D status.
Similar content being viewed by others

Log in or create a free account to read this content
Gain free access to this article, as well as selected content from this journal and more on nature.com
or
References
Viswanathan, S. et al. Metabolic bone disease: a continued challenge in extremely low birth weight infants. J. Parenter. Enter. Nutr. 38, 982–990 (2014).
Rustico, S. E., Calabria, A. C. & Garber, S. J. Metabolic bone disease of prematurity. J. Clin. Transl. Endocrinol. 1, 85–91 (2014).
Ukarapong, S., Venkatarayappa, S. K. B., Navarrete, C. & Berkovitz, G. Risk factors of metabolic bone disease of prematurity. Early Hum. Dev. 112, 29–34 (2017).
Lee, S. M. et al. High incidence of rickets in extremely low birth weight infants with severe parenteral nutrition-associated cholestasis and bronchopulmonary dysplasia. J. Korean Med. Sci. 27, 1552–1555 (2012).
Hojsak, I. et al. ESPGHAN Committee on Nutrition Position Paper. Intravenous lipid emulsions and risk of hepatotoxicity in infants and children: a systematic review and meta-analysis. J. Pediatr. Gastroenterol. Nutr. 62, 776–792 (2016).
Christensen, R. D., Henry, E., Wiedmeier, S. E., Burnett, J. & Lambert, D. K. Identifying patients, on the first day of life, at high-risk of developing parenteral nutrition-associated liver disease. J. Perinatol. 27, 284–290 (2007).
Heubi, J. E., Hollis, B. W., Specker, B. & Tsang, R. C. Bone disease in chronic childhood cholestasis. I. vitamin D absorption and metabolism. Hepatology 9, 258–264 (1989).
Mohammadi, B. et al. Prevalence of vitamin D deficiency and rickets in children with cholestasis in Iran. Acta Med. Iran 50, 482–485 (2012).
Samra, N. M., Emad El Abrak, S., El Dash, H. H., El Said El Raziky, M. & El Sheikh, M. A. Evaluation of vitamin D status bone mineral density and dental health in children with cholestasis. Clin. Res. Hepatol. Gastroenterol. 42, 368–377 (2018).
Jensen, M., Abu-El-Haija, M., Bishop, W. & Rahhal, R. M. Difficulty achieving vitamin D sufficiency with high-dose oral repletion therapy in infants with cholestasis. J. Pediatr. Gastroenterol. Nutr. 61, 187–189 (2015).
Wozniak, L. J., Bechtold, H. M., Reyen, L. E., Hall, T. R. & Vargas, J. H. Vitamin D deficiency in children with intestinal failure receiving home parenteral nutrition. JPEN J. Parent. Enter. Nutr. 39, 471–475 (2015).
Ubesie, A. C. et al. Vitamin D deficiency and low bone mineral density in pediatric and young adult intestinal failure. J. Pediatr. Gastroenterol. Nutr. 57, 372–376 (2013).
Moon, R. J., Harvey, N. C., Davies, J. H. & Cooper, C. Vitamin D and skeletal health in infancy and childhood. Osteoporos. Int. 25, 2673–2684 (2014).
Duro, D. et al. Risk factors for parenteral nutrition-associated liver disease following surgical therapy for necrotizing enterocolitis: a Glaser Pediatric Research Network Study [corrected]. J. Pediatr. Gastroenterol. Nutr. 52, 595–600 (2011).
Koseesirikul, P., Chotinaruemol, S. & Ukarapol, N. Incidence and risk factors of parenteral nutrition-associated liver disease in newborn infants. Pediatr. Int. 54, 434–436 (2012).
Satrom, K. & Gourley, G. Cholestasis in preterm infants. Clin. Perinatol. 43, 355–373 (2016).
Alkharfy, T. M., Ba-Abbad, R., Hadi, A., Sobaih, B. H. & AlFaleh, K. M. Total parenteral nutrition-associated cholestasis and risk factors in preterm infants. Saudi J. Gastroenterol. 20, 293–296 (2014).
Koo, W. W. et al. Minimal vitamin D and high calcium and phosphorus needs of preterm infants receiving parenteral nutrition. J. Pediatr. Gastroenterol. Nutr. 8, 225–233 (1989).
Kimura, S. et al. Serum levels of vitamin D metabolites in children receiving total parenteral nutrition. JPEN J. Parent. Enter. Nutr. 10, 191–194 (1986).
Wortsman, J., Matsuoka, L. Y., Chen, T. C., Lu, Z. & Holick, M. F. Decreased bioavailability of vitamin D in obesity. Am. J. Clin. Nutr. 72, 690–693 (2000).
Gangloff, A. et al. Effect of adipose tissue volume loss on circulating 25-hydroxyvitamin D levels: results from a 1-year lifestyle intervention in viscerally obese men. Int. J. Obes. (Lond.) 39, 1638–1643 (2015).
Chhina, A. S., Shenoi, A., Nagendra, N., Rao, N. & Raja, M. Vitamin D and metabolic bone parameters in preterm neonates. Indian Pediatr. 53, 1023–1024 (2016).
Moreira, A. et al. Parathyroid hormone as a marker for metabolic bone disease of prematurity. J. Perinatol. 34, 787–791 (2014).
Ruiz-Gaspà, S. et al. Effects of bilirubin and sera from jaundiced patients on osteoblasts: Contribution to the development of osteoporosis in liver diseases. Hepatology 54, 2104–2113 (2011).
Ruiz-Gaspà, S. et al. Lithocholic acid downregulates vitamin D effects in human osteoblasts. Eur. J. Clin. Investig. 40, 25–34 (2010).
Kolodziejczyk, A. & Borszewska-Kornacka, M. K. Monitored supplementation of vitamin D in preterm neonates–a primary report. Dev. Period Med. 19(3 Pt 1), 313–318 (2015).
Nako, Y., Tomomasa, T. & Morikawa, A. Risk of hypervitaminosis D from prolonged feeding of high vitamin D premature infant formula. Pediatr. Int. 46, 439–443 (2004).
Author information
Authors and Affiliations
Contributions
S.U., W.Z. and C.N. collected and analyzed the data and drafted the manuscript. T.S. and G.B. extensively revised and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Ukarapong, S., Zegarra, W., Navarrete, C. et al. Vitamin D status among preterm infants with cholestasis and metabolic bone disease. Pediatr Res 86, 725–731 (2019). https://doi.org/10.1038/s41390-019-0501-x
Received:
Revised:
Accepted:
Published:
Issue date:
DOI: https://doi.org/10.1038/s41390-019-0501-x
This article is cited by
-
Effect of early preventive supplementation with calcium and phosphorus on metabolic bone disease in premature infants
BMC Pediatrics (2024)
-
Establishment of a nomogram model for predicting metabolic bone disease in preterm infants: A case‒control study
European Journal of Pediatrics (2023)
