
Abstract
Background
Interpretations of pediatric COVID-19 severity are complicated by novel lineages and COVID-19 vaccine introduction. We estimated the risk of severe COVID-19 by SARS-CoV-2 lineage and vaccination status among hospitalized Canadian children.
Methods
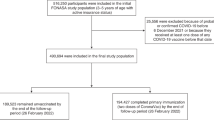
Data were collected through the Canadian Paediatric Surveillance Program (April 2020–May 2021) and Canadian Immunization Monitoring Program, ACTive (June 2021–December 2022). Patients <17 years hospitalized for COVID-19 (excluding incidental SARS-CoV-2) at 13 pediatric hospitals were included. Lineages were defined via genetic sequencing or dominant lineage upon hospitalization. Severe disease included intensive care, ventilatory/hemodynamic requirements, systemic complications, and/or death.
Results
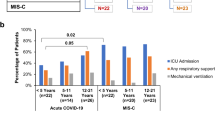
We analyzed 3218 COVID-19 hospitalizations, including 81.4% admitted during Omicron predominance. Median age was highest among Delta cases (2.9 years, interquartile range [IQR] 0.2–10.9) and lowest among Omicron BQ.1 cases (0.6 years, IQR 0.2–1.8). Severe COVID-19 remained common in Omicron vs. ancestral cases (27.2% vs. 23.2%). The proportion of hospitalized cases aged 5–16 years declined following the introduction of age-specific COVID-19 vaccines. Vaccination reduced the risk of in-hospital severe disease for ages 12–16 years (two vs. zero doses; adjusted risk ratio 0.49, 95% confidence interval 0.32–0.77).
Conclusion
More children were hospitalized with Omicron lineages than all prior lineages. COVID-19 vaccination was associated with a lower burden of severe disease among ages 5–16 years.
Impact statement
-
This study estimates the effect of SARS-CoV-2 lineage, Omicron sub-lineage, and vaccination on COVID-19 disease severity, using data from two Canadian national surveillance programs.
-
Few national studies describe the clinical presentation and severity of Omicron sub-lineages among hospitalized children.
-
In Canada, Omicron lineages were associated with substantially more pediatric COVID-19 hospitalizations than all prior lineages combined, though risk of severe COVID-19 was highest during the Delta period.
-
COVID-19 vaccines were associated with reductions in hospitalization (ages 5–16 years) and severe disease (ages 12–16 years) across Omicron sub-lineages.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 14 print issues and online access
$259.00 per year
only $18.50 per issue
Buy this article
- Purchase on SpringerLink
- Instant access to the full article PDF.
USD 39.95
Prices may be subject to local taxes which are calculated during checkout



Similar content being viewed by others

Data availability
Anonymized individual case data (including data dictionaries) from the CPSP and IMPACT COVID-19 studies can be made available to investigators whose secondary data analysis study protocol has been approved by an independent research ethics board, and which abides by the privacy rules of the Canadian Paediatric Society and Public Health Agency of Canada. Proposals should be submitted to the corresponding authors.
References
Markov, P. V. et al. The evolution of SARS-CoV-2. Nat. Rev. Microbiol. 21, 361–379 (2023).
Lin, L., Liu, Y., Tang, X. & He, D. The disease severity and clinical outcomes of the SARS-CoV-2 variants of concern. Front. Public Health 9, 775224 (2021).
Relan, P. et al. Severity and outcomes of Omicron variant of SARS-CoV-2 compared to Delta variant and severity of Omicron sublineages: a systematic review and metanalysis. BMJ Glob. Health 8, e012328 (2023).
Public Health Agency of Canada. COVID-19 Epidemiology Update: Current Situation. https://health-infobase.canada.ca/covid-19/current-situation.html (Government of Canada, 2024).
Wiedenmann, M. et al. SARS-CoV-2 variants of concern in children and adolescents with COVID-19: a systematic review. BMJ Open 13, e072280 (2023).
Ikuse, T. et al. Comparison of clinical characteristics of children infected with coronavirus disease 2019 between Omicron variant BA.5 and BA.1/BA.2 in Japan. Pediatr. Infect. Dis. J. 42, 503–509 (2023).
Pokorska-Śpiewak M., et al. Differences in Clinical Presentation of COVID-19 in Children Hospitalized During Domination of Early (BA.1, BA.2) and Late (BA.5, BA.2.75, BQ.1 and XBB.1.5) SARS-CoV-2 Omicron Subvariants. Pediatr. Infect. Dis. J. Published online November 3, https://doi.org/10.1097/INF.0000000000004167 (2023).
Naeimi, R. et al. SARS-CoV-2 seroprevalence in children worldwide: a systematic review and meta-analysis. EClinicalMedicine 56, 101786 (2023).
Mathieu, E. et al. A global database of COVID-19 vaccinations. Nat. Hum. Behav. 5, 947–953 (2021).
Bardsley, M. et al. Epidemiology of respiratory syncytial virus in children younger than 5 years in England during the COVID-19 pandemic, measured by laboratory, clinical, and syndromic surveillance: a retrospective observational study. Lancet Infect. Dis. 23, 56–66 (2023).
Ujiie, M., Tsuzuki, S., Nakamoto, T. & Iwamoto, N. Resurgence of respiratory syncytial virus infections during COVID-19 pandemic, Tokyo, Japan. Emerg. Infect. Dis. 27, 2969–2970 (2021).
White, E. B. et al. High influenza incidence and disease severity among children and adolescents aged <18 years—United States, 2022-23 Season. Morb. Mortal. Wkly Rep. 72, 1108–1114 (2023).
Zambrano, L. D. et al. Durability of original monovalent mRNA vaccine effectiveness against COVID-19 Omicron-associated hospitalization in children and adolescents - United States, 2021-2023. Morb. Mortal. Wkly Rep. 73, 330–338 (2024).
Anderson, E. J. et al. Evaluation of mRNA-1273 Vaccine in Children 6 Months to 5 Years of Age. N. Engl. J. Med. 387, 1673–1687 (2022).
Government of Canada. Drug and Vaccine Authorizations for COVID-19: List of Authorized Drugs, Vaccines and Expanded Indications.; 2024. Accessed Feb 28, 2024. https://www.canada.ca/en/health-canada/services/drugs-health-products/covid19-industry/drugs-vaccines-treatments/authorization/list-drugs.html
Canadian Paediatric Surveillance Program. About the CPSP. https://cpsp.cps.ca/about-apropos
Drouin, O. et al. Characteristics of children admitted to hospital with acute SARS-CoV-2 infection in Canada in 2020. CMAJ 193, E1483–E1493 (2021).
Farrar, D. S. et al. Risk factors for severe COVID-19 in hospitalized children in Canada: a national prospective study from March 2020-May 2021. Lancet Reg. Health Am. 15, 100337 (2022).
Bettinger, J. A. et al. The Canadian Immunization Monitoring Program, ACTive (IMPACT): active surveillance for vaccine adverse events and vaccine-preventable diseases. Can. Commun. Dis. Rep. 40, 41–44 (2014).
Shu, Y. & McCauley, J. GISAID: Global initiative on sharing all influenza data - from vision to reality. Eur. Surveill. 22, 30494 (2017).
WHO Working Group on the Clinical Characterisation and Management of COVID-19 infection. A minimal common outcome measure set for COVID-19 clinical research. Lancet Infect. Dis. 20, e192–e197 (2020).
StataCorp. Stata Statistical Software: Release 18.; (2023).
Ward, J. L. et al. Pediatric hospitalizations and ICU admissions Due to COVID-19 and pediatric inflammatory multisystem syndrome temporally associated with SARS-CoV-2 in England. JAMA Pediatr. 177, 947–955 (2023).
Zhu, Y. et al. International Pediatric COVID-19 severity over the course of the pandemic. JAMA Pediatr. 177, 1073–1084 (2023).
Public Health Agency of Canada. Canadian COVID-19 Vaccination Coverage Report. Public Health Agency of Canada; 2024. https://health-infobase.canada.ca/covid-19/vaccination-coverage/
Krumbein, H. et al. Respiratory viral co‐infections in patients with COVID‐19 and associated outcomes: a systematic review and meta‐analysis. Rev. Med. Virol. 33, e2365 (2023).
Yuan, Z., Shao, Z., Ma, L. & Guo, R. Clinical severity of SARS-CoV-2 variants during COVID-19 vaccination: a systematic review and meta-analysis. Viruses 15, 1994 (2023).
Huai Luo, C. et al. Infection with the severe acute respiratory syndrome Coronavirus 2 (SARS-CoV-2) delta variant is associated with higher recovery of infectious virus compared to the alpha variant in both unvaccinated and vaccinated individuals. Clin. Infect. Dis. 75, e715–e725 (2022).
Menni, C. et al. Symptom prevalence, duration, and risk of hospital admission in individuals infected with SARS-CoV-2 during periods of omicron and delta variant dominance: a prospective observational study from the ZOE COVID Study. Lancet 399, 1618–1624 (2022).
Fisman, D. N. & Tuite, A. R. Age-specific changes in virulence associated with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) variants of concern. Clin. Infect. Dis. 75, e69–e75 (2022).
Martin, B. et al. Characteristics, outcomes, and severity risk factors associated with SARS-CoV-2 infection among children in the US national COVID cohort collaborative. JAMA Netw. Open 5, e2143151 (2022).
Wolter, N. et al. Clinical severity of SARS-CoV-2 Omicron BA.4 and BA.5 lineages compared to BA.1 and Delta in South Africa. Nat. Commun. 13, 5860 (2022).
Public Health Agency of Canada. Respiratory Virus Detection Report - December 25 to December 31, 2022 (Surveillance Week 2022-52). Public Health Agency of Canada; 2023. https://www.canada.ca/en/public-health/services/surveillance/respiratory-virus-detections-canada/2022-2023/week-52-ending-december-31-2022.html
Viñeta Paramo, M. et al. Respiratory syncytial virus epidemiology and clinical severity before and during the COVID-19 pandemic in British Columbia, Canada: a retrospective observational study. Lancet Reg. Health Am. 25, 100582 (2023).
Scotta, M. C. et al. Respiratory viral coinfection and disease severity in children: A systematic review and meta-analysis. J. Clin. Virol. 80, 45–56 (2016).
Olson, S. M. et al. Effectiveness of Pfizer-BioNTech mRNA vaccination against COVID-19 hospitalization among persons aged 12-18 years - United States, June-September 2021. Morb. Mortal. Wkly Rep. 70, 1483–1488 (2021).
Price, A. M. et al. BNT162b2 protection against the Omicron variant in children and adolescents. N. Engl. J. Med. 386, 1899–1909 (2022).
Piché-Renaud, P. P. et al. COVID-19 vaccine effectiveness against omicron infection and hospitalization. Pediatrics 151, e2022059513 (2023).
Halasa, N. B. et al. Maternal vaccination and risk of hospitalization for Covid-19 among infants. N. Engl. J. Med. 387, 109–119 (2022).
Jorgensen, S. C. J. et al. Newborn and early infant outcomes following maternal COVID-19 vaccination during pregnancy. JAMA Pediatr. 177, 1314–1323 (2023).
Zinszer, K. et al. Seroprevalence of SARS-CoV-2 antibodies among children in school and day care in Montreal, Canada. JAMA Netw. Open 4, e2135975 (2021).
Skowronski, D. M. et al. Serial cross-sectional estimation of vaccine-and infection-induced SARS-CoV-2 seroprevalence in British Columbia, Canada. CMAJ 194, E1599–E1609 (2022).
Acknowledgements
We acknowledge all past IMPACT site investigators and working group members involved in IMPACT at the time of data collection, as well as the pediatricians, pediatric subspecialists, and health professionals who voluntarily respond to CPSP surveys. We thank Annick Audet (IMPACT Nurse Monitor Liaison) and Melanie Laffin Thibodeau (former CPSP Surveillance Manager) for their stewardship in the IMPACT and CPSP studies, respectively. We are also grateful to all IMPACT Nurse Monitors who collected data for the IMPACT COVID-19 study, and staff of the IMPACT data center. CPSP and IMPACT are joint projects of the Canadian Paediatric Society (CPS) and the Public Health Agency of Canada (PHAC). Funding for the surveillance activities conducted by these programs was provided by PHAC, in collaboration with the COVID-19 Immunity Task Force (CITF) for this project.
Author information
Authors and Affiliations
Consortia
Contributions
Daniel Farrar planned and conducted the statistical analysis, and drafted the initial manuscript. Julie A. Bettinger conceptualized and designed the study, oversaw the analysis, and reviewed and revised the manuscript. Aaron Campigotto, Joanne E. Embree, Scott A. Halperin, Tajdin Jadavji, Kescha Kazmi, Jesse Papenburg, Rupeena Purewal, Manish Sadarangani, and Laura Sauvé contributed to the study design, data collection, and reviewed and revised the manuscript. Oliver Drouin and Charlotte Moore Hepburn were co-leads of the CPSP COVID-19 study, and reviewed and revised the manuscript. Melanie King was the Surveillance Manager of the Canadian Paediatric Surveillance Program when the analysis was conducted, and reviewed and revised the manuscript. Karina A. Top was co-Principal Investigator of the IMPACT COVID-19 study, conceptualized and designed the study, contributed to funding acquisition and data collection, oversaw the analysis, and reviewed and revised the manuscript. Fatima Kakkar and Shaun K. Morris were co-principal Investigators of the CPSP and IMPACT COVID-19 studies, conceptualized and designed the study, contributed to funding acquisition and data collection, oversaw the analysis, and reviewed and revised the manuscript. All authors approved the final manuscript as submitted and agreed to be accountable for all aspects of the work.
Corresponding authors
Ethics declarations
Competing interests
O.D. and F.K. are supported by a Clinical Research Scholars Award from the Fonds de recherche du Québec—Santé. S.A.H. received funding from multiple vaccine manufacturers to undertake phase 1–3 clinical trials of candidate COVID-19 vaccines. J.P. reported grants from Merck, and personal fees from Enanta, outside the submitted work. M.S. is supported via salary awards from the BC Children’s Hospital Foundation and Michael Smith Health Research BC. M.S. has also been an investigator on projects funded by GlaxoSmithKline, Merck, Moderna, Pfizer, and Sanofi-Pasteur. All funds have been paid to his institute, and he has not received any personal payments. K.A.T. received grants from the Coalition for Epidemic Preparedness Innovations outside the submitted work. S.K.M. has received honoraria for lectures from GlaxoSmithKline and Sanofi Pasteur and has been a member of ad hoc advisory boards for Pfizer, Sanofi Pasteur, and Apotex, all unrelated to this study. All other authors have no conflicts of interest to disclose.
Consent statement
The CPSP collects data elements for national child and youth health surveillance purposes on PHAC’s behalf, whose purpose is to support health protection and promotion under the Department of Health Act 4(2)c and the Public Health Agency of Canada Act 3(15). Healthcare providers are authorized under their provincial health privacy legislation (with the exception of Quebec) to disclose protected health information to public health agencies at the local, provincial, and federal levels for surveillance purposes. CPSP does not collect any individual data elements deemed to be unique identifiers. In Quebec, CPSP studies are conducted under center-specific research ethics board approvals and data transfer agreements. This is consistent with the Canadian Medical Association and Tri-Council Policy Statements, which allow for the collection of non-nominal and nonidentifiable information for conditions under surveillance. For the IMPACT COVID-19, investigators at each IMPACT center also obtained Research Ethics Board or hospital approvals from their institution, and received waivers of consent for secondary use of patient-level data.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Farrar, D.S., Bettinger, J.A., Campigotto, A.J. et al. Pediatric COVID-19 severity by SARS-CoV-2 lineage and vaccine status in Canada: an IMPACT study. Pediatr Res 98, 697–705 (2025). https://doi.org/10.1038/s41390-025-03853-0
Received:
Revised:
Accepted:
Published:
Version of record:
Issue date:
DOI: https://doi.org/10.1038/s41390-025-03853-0
