
Abstract
Study Design
Online survey of spinal cord injury (SCI) practitioners.
Objectives
Determine provider understanding and routine performance of International Standards for Neurologic Classification of Spinal Cord Injury (ISNCSCI) anorectal examination.
Setting
International online questionnaire.
Methods
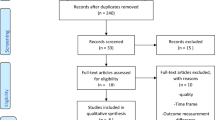
A descriptive survey was developed to assess current performance of the ISNCSCI anorectal exam. Information about this survey was disseminated through social email and international societies between the months of March and April 2017.
Results
Two hundred and fifteen SCI practitioners completed the survey. Of these, 157 (73%) were specialists in physical medicine and rehabilitation, 32 (15%) were physical therapists, 6 were neurologists, 6 were orthopedists, and 3 were neurosurgeons. Of responders, 90% routinely personally performed the anal exam of the ISNCSCI, of whom, 42 placed firm pressure against the anal sphincter, 58 placed firm pressure against the rectal wall, and 87 placed firm pressure against the anal sphincter and rectal wall as part of the exam. On a routine basis, 74% tested sensation at the junction of the anal sphincter and skin, 82% had the patient attempt to squeeze their finger, and 50% performed the bulbocavernosus reflex.
Conclusions
Marked inconsistency exists in the performance of the ISNCSCI anal examination. Researchers and clinicians need more education about the performance of the examination. Consideration should be given for the components of deep rectal sensation and anal pressure to be separately documented in the neurologic exam and for researchers to focus separately on recovery of sacral function vs. ambulatory function in clinical trials.
Similar content being viewed by others

Log in or create a free account to read this content
Gain free access to this article, as well as selected content from this journal and more on nature.com
or
References
Krishna V, Andrews H, Varma A, Mintzer J, Kindy MS, Guest J. Spinal cord injury: How can we improve the classification and quantification of its severity and prognosis. J. Neurotrauma. 2014;31:215–27.
Zariffa J, Kramer J, Jones L, Lammertse D, Curt A. European multicenter study about SCI Group, et al. sacral sparing in SCI; beyond the S4-S5 and anorectal examination. The Spine 2012;12:389–400.
Samdani A, Chafetz RS, Vogel LC, Betz RR, Gaughan JP, Mulcahey MJ. The international standards for neurological classification of spinal cord injury: relationship between S4-5 dermatome testing and anorectal testing. Spinal. Cord. 2011;49:352–6.
American Spinal Injury Association. International Standards for the Neurological Classification of Spinal Cord Injury. Chicago: American SpinalInjury Association; 2003.
American Spinal Injury Association. Standards for Neurological Classification of Spinal Cord Injury Patients. Chicago: American Spinal Injury Association; 1989.
American Spinal Injury Association. Standards for Neurological Classification of Spinal Cord Injury Patients. Chicago: American Spinal Injury Association; 1982.
American Spinal Injury Association/International Medical Society of Paraplegia (ASIA/IMSOP). International Standards for Neurological and Functional Classification of Spinal Cord Injury Patients (revised). Chicago: American Spinal Injury Association; 1992.
Marino RM, Schmidt-Read M, Kirshblum S, Dyson-Hudson TA, Tansey K, Morse LR, et al. Reliability and validity of S3 pressure sensation as an alternative to deep anal pressure in neurologic classification of persons with spinal cord injury. Arch. Phys. Med. Rehabil. 2016;97:1642–6.
Mulcahey MJ, Gaughan J, Betz RB, Vogel LC. Rater agreement on the ISCSCI motor and sensory scores obtained before and after formal training in testing technique. J. Spinal. Cord. Med. 2007;30:S146–9.
American Spinal Injury Association. Reference Manual for the International Standards for Neurological Classification of Spinal Cord Injury. Chicago: American SpinalInjury Association; 2003.
www.asia-spinalinjury.org/elearning. Accessed June 21, 2017.
American Spinal Injury Association. Reference Manual for the International Standards for Neurological Classification of Spinal Cord Injury. Chicago: American SpinalInjury Association; 1994.
Rogers J. Testing for and the role of anal and rectal sensation. Bailliers Clin Gastroenterol 1992;6:179–191.
Kirshblum SC, Burns S, Biering-Sorensen F, Donovan W, Graves D, Jha A, et al. International standards for neurological classification of spinal cord injury (Revised 2011). J. Spinal. Cord. Med. 2011;34:346–52.
Kirshblum S, Waring W. Updates for the international standards for neurological classification of spinal cord injury. Phys. Med. Rehabil. Clin. N. Am. 2014;25:505–17.
Eickhoff SB, Lotze M, Wietek B, Amunts K, Enck P, Zilles K. Segregation of visceral and somatosensory afferents: an fMRI and cytoarchitectonic mapping study. Neuroimage. 2006;31:1004–1014.
Chan CLH, Ponsford S, Scott SM, Swash M, Lunniss PJ. Contribution of the pudendal nerve to sensation of the distal rectum. Br. J. Surg. 2005;92:859–865.
van Middendorp JJ, Hosman AJF, Pouw MH, Van de Meent H. Is determination between complete and incomplete traumatic spinal cord injury clinically relevant? Validation of the ASIA sacral sparing criteria in a prospective cohort of 432 patients. Spinal. Cord. 2009;47:809–816.
Wietek BM, Baron CH, Erb M, Hinninghofen H, Baktke A, Kaps H, et al. Cortical processing of residual ano-rectal sensation in patients with spinal cord injury: an fMRI study. Neurogastroenterol. Motil. 2008;20:488–497.
Krisa L, Middleton D, Faro S, Calhoun C, Mohamed F, Mulcahey M. Cerebral activation during the test of spinal cord injury severity in children; an fMRI methodological study. Top Spinal Cord Injury Rehabil 2013;19:121–8.
Vogel L, Samdani A, Chafetz R, Gaughan J, Betz R, Mulcahey MJ. Intra-rater agreement of the anorectal exam and classification of injury severity in children with spinal cord injury. Spinal. Cord. 2009;47:687–691.
Lammertse DP, Jones LA, Charlifue SB, Kirshblum SC, Apple DF, Ragnarsson KT, et al. Autologous incubated macrophage therapy in acute, complete spinal cord injury: results of the phase 2 randomized controlled multicenter trial. Spinal. Cord. 2012;50:661–671.
Kirshblum S, Botticello A, Lammertse DP, Marino RJ, Chiodo AE, Jha A. The impact of sacral sensory sparing in motor complete spinal cord injury. Arch. Phys. Med. Rehabil. 2011;92:376–383.
Alexander MS, Carr C, Chen YY, McLain A. The use of the neurologic examination to predict awareness of lower urinary tract function post SCI. Spinal. Cord. 2017;55:795, https://doi.org/10.1038/sc2017.55.
Weiss DJ, Fried GW, Chancellor MB, Herbison GH, Ditunno JF, Staas WE. Spinal cord injury and bladder recovery. Arch. Phys. Med. Rehabil. 1996;77:1133–5.
Sipski ML, Alexander CJ, Rosen RC. Sexual arousal and orgasm in women: effects of spinal cord injury. Ann. Neurol. 2001;49:35–44.
Sipski M, Alexander CJ, Gomez-Marin O. Effects of level and degree of spinal cord injury on male orgasm. Spinal. Cord. 2006;44:798–804.
Anderson KD. Targeting Recovery: Priorities of the Spinal Cord-Injured Population. J. Neurotrauma. 2004;21:1371–83.
Alexander MS, Biering-Sorensen F, Bodner D, Brackett NL, Cardenas D, Charlifue S, et al. International standards to document remaining autonomic function after spinal cord injury. Spinal. Cord. 2009;47:36–43.
Krassioukov A, Biering-Sorensen F, Donovan W, Kennelly M, Kirshblum S, Krogh K, et al. International standards to document remaining autonomic function after spinal CordInjury (ISAFSCI). Top SCI Rehabil 2012;18:283–96. First Edition 2012
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
MA is a consultant for in-vivo therapeutics. The remaining authors declare that they have no competing interests.
Rights and permissions
About this article

Cite this article
Alexander, M., Aslam, H. & Marino, R.J. Pulse article: How do you do the international standards for neurological classification of SCI anorectal exam?. Spinal Cord Ser Cases 3, 17078 (2017). https://doi.org/10.1038/s41394-017-0015-x
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41394-017-0015-x
This article is cited by
-
What is the clinical meaning of a negative bulbocavernosus reflex in spinal cord injury patients?
Spinal Cord Series and Cases (2022)
-
The sacral exam—what is needed to best care for our patients?
Spinal Cord Series and Cases (2020)
-
Use of the ice water test as an early predictor of recovery of erectile function in patients with spinal cord injury
Spinal Cord Series and Cases (2020)
-
Anal reflex versus bulbocavernosus reflex in evaluation of patients with spinal cord injury
Spinal Cord Series and Cases (2020)
-
An interview based approach to the anorectal portion of the International Standards of Neurological Classification of Spinal Cord Injury Exam (I-A-ISNCSCI): a pilot study
Spinal Cord (2020)
