
Abstract
Introduction
Pregnancy-related spinal tumors (PRSTs) are unusual tumors that present during pregnancy or within a year after delivery. We describe a fatal holocord recurrence of a spinal ependymoma, which, to the best of our knowledge, is one of the most extensive PRSTs reported thus far.
Case presentation
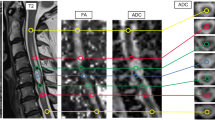
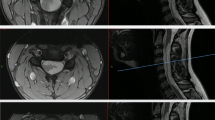
A 21-year-old primigravida presented at 6 months of gestation with urinary incontinence for 2 months and spastic paraparesis for 1 month. MRI showed a conus intramedullary lesion from T10 to 12. Near-total resection of the lesion was performed. The histopathological diagnosis was that of a cellular ependymoma (WHO grade II). The patient presented 6 months later with progressive quadriparesis and breathing difficulty. MRI demonstrated holocord recurrence of the tumor with edema extending to the pontomedullary junction. The patient succumbed to respiratory failure before decompression of the tumor could be performed.
Discussion
This case highlights an unusual clinical course of a pregnancy-related, low-grade spinal ependymoma. The possible hormonal and genetic mechanisms underlying the aggressive involvement of the entire spinal cord by the recurrent tumor are discussed in the light of a literature review. Future studies may shed light on the possibility of utilizing these mechanisms as therapeutic targets to alter the clinical course of aggressive spinal ependymomas.
Similar content being viewed by others

Log in or create a free account to read this content
Gain free access to this article, as well as selected content from this journal and more on nature.com
or
References
Schittenhelm J, Ebner FH, Tatagiba M, Wolff M, Nägele T, Meyermann R, et al. Holocord pilocytic astrocytoma-case report and review of the literature. Clin Neurol Neurosurg. 2009;111:203–7.
Epstein F, Epstein N. Surgical management of holocord intramedullary spinal cord astrocytomas in children. J Neurosurg. 1981;54:829–32.
Horrax G, Henderson DG. Encapsulated intramedullary tumor involving the whole spinal cord from medulla to conus: complete enucleation with recovery. Surg Gynecol Obstet. 1939;68:814–9.
Fischer G, Pierluca P, Sindou M, Pialat J. Pan-spinal ependymoma. Apropos of 2 cases with complete exeresis. Neurochirurgie. 1975;21:5–20.
Nakamura S, Yamada H, Tajima M, Yoshida J, Kobayashi T, Kagemaya N. Intramedullary tumor involving from brain stem to conus medullaris. Shoni No Noshinke. 1980;5:199–203.
Tanaka H, Shimizu H, Ishijima B, Nakamura Y. Myxopapillary ependymoma of the filum terminale with a holocord cyst: a case report. No Shinkei Geka. 1986;14:997–1003.
Gunes HF, Ozdemir N. Holocord ependymoma. Turk Neurosurg. 2012;22:250–3.
Aryan S, Ghosal N, Aziz ZA, Hegde AS, Dadlani R. Infantile holocord cellular ependymoma with communicating hydrocephalus: unusual presentation of a rare case. Brain Tumor Pathol. 2014;31:47–50.
Bhaisora KS, Sharma P, Srivastava AK, Mehrotra A, Das KK, Sardhara J, et al. Single staged complete length excision of the holocord ependymoma: team work. J Pediatr Neurosci. 2015;10:396–8.
Cushing H. The intracranial tumors of preadolescence. Am J Dis Child. 1927;33:551–84.
Pavlidis NA. Coexistence of pregnancy and malignancy. Oncologist. 2002;7:279–87.
Van Calsteren K, Heyns L, De Smet F, Van Eycken L, Gziri MM, Van Gemert W, et al. Cancer during pregnancy: an analysis of 215 patients emphasizing the obstetrical and the neonatal outcomes. J Clin Oncol. 2010;28:683–9.
Meng T, Yin H, Li Z, Li B, Zhou W, Wang J, et al. Therapeutic strategy and outcome of spine tumors in pregnancy: a report of 21 cases and literature review. Spine. 2015;40:E146–53.
Schweitzer JS, Batzdorf U. Ependymoma of the cauda equina region: diagnosis, treatment, and outcome in 15 patients. Neurosurgery. 1992;30:202–7.
Jaeger M, Rickels E, Schmidt A, Samii M, Blömer U. Lumbar ependymoma presenting with paraplegia following attempted spinal anaesthesia. Br J Anaesth. 2002;88:438–40.
Uzun Ş, Kara D, Akbay A. Anesthetic management of a pregnant woman with a cervical intramedullar ependymoma. Acta Med. 2014;45:86–8.
van der Hoeven ME, de Pont LM, Koppen H. Severe nightly thoracic pain presenting during pregnancy: a case report. Case Rep Neurol. 2018;10:135–9.
Fujii K, Orisaka M, Yamamoto M, Nishijima K, Yoshida Y. Primary intramedullary spinal cord tumour in pregnancy: a case report. Spinal Cord Ser Cases. 2018;4:1–5.
Bitterman J, Donovan J, Lam M. Diagnosis and rehabilitation of a pregnant woman with spinal cord disorder due to spinal cord tumor. Spinal Cord Ser Cases. 2019;5:1–4.
Ross AE, Bojescul JA, Kuklo TR. Giant cell tumor: a case report of recurrence during pregnancy. Spine. 2005;30:E332–5.
Kiroglu Y, Benek B, Yagci B, Cirak B, Tahta K. Spinal cord compression caused by vertebral hemangioma being symptomatic during pregnancy. Surg Neurol. 2009;71:487–92.
Hayden MG, Gephart R, Kalanithi P, Chou D. Von Hippel-Lindau disease in pregnancy: a brief review. J Clin Neurosci. 2009;16:611–3.
Terra Júnior JA, Daneze ER, Terra GA, Etchebehere RM, Barbosa AB, Terra SA. Subcostal schwannoma in pregnancy. Arq Neuropsiquiatr. 2012;70:901–2.
Roelvink NC, Kamphorst W, van Alphen HA, Rao BR. Pregnancy-related primary brain and spinal tumors. Arch Neurol. 1987;44:209–15.
Malawer M, Bray M, Kass M. Fluorescent histochemical demonstration of estrogen and progesterone binding in giant cell tumors of bone: preliminary observations. J Surg Oncol. 1984;25:148–52.
Olivera P, Perez E, Ortega A, Terual R, Gomes C, Moreno LF, et al. Estrogen receptor expression in giant cell tumors of the bone. Hum Pathol. 2002;33:165–9.
Yust-Katz S, de Groot JF, Liu D, Wu J, Yuan Y, Anderson MD, et al. Pregnancy and glial brain tumors. Neuro Oncol. 2014;16:1289–94.
Liu M, Zhang K, Zhao Y, Guo Q, Guo D, Zhang J. Evidence for involvement of steroid receptors and coactivators in neuroepithelial and meningothelial tumors. Tumour Biol. 2015;36:3251–61.
Khalid SI, Adogwa O, Kelly R, Metha A, Bagley C, Cheng J, et al. Adult spinal ependymomas: an epidemiologic study. World Neurosurg. 2018;111:e53–61.
Ostrom QT, Gittleman H, Truitt G, Boscia A, Kruchko C, Barnholtz-Sloan JS. CBTRUS statistical report: primary brain and other central nervous system tumors diagnosed in the United States in 2011–2015. Neuro Oncol. 2018;20:iv1–86.
Concolino G, Liccardo G, Conti C, Panfili C, Giuffre R. Hormones and tumours in central nervous system (CNS): steroid receptors in primary spinal cord tumours. Neurological Res. 1984;6:121–6.
Ghasemi DR, Sill M, Okonechnikov K, Korshunov A, Yip S, Schutz PW, et al. MYCN amplification drives an aggressive form of spinal ependymoma. Acta Neuropathol. 2019;138:1075–89.
Barone G, Anderson J, Pearson AD, Petrie K, Chesler L. New strategies in neuroblastoma: therapeutic targeting of MYCN and ALK. Clin Cancer Res. 2013;19:5814–21.
Colicchia V, Petroni M, Guarguaglini G, Sardina F, Sahún-Roncero M, Carbonari M, et al. PARP inhibitors enhance replication stress and cause mitotic catastrophe in MYCN dependent neuroblastoma. Oncogene. 2017;36:4682–91.
Gustafson WC, Meyerowitz JG, Nekritz EA, Chen J, Benes C, Charron E, et al. Drugging MYCN through an allosteric transition in Aurora kinase A. Cancer Cell. 2014;26:414–27.
Henssen A, Althoff K, Odersky A, Beckers A, Koche R, Speleman F, et al. Targeting MYCN-driven transcription by BET-bromodomain inhibition. Clin Cancer Res. 2016;22:2470–81.
Acknowledgements
The authors acknowledge the contribution of Mr. Nagesh B. (BPT, MPT-Neuro, and Neurosurgical Rehabilitation, MIAP), Head of Department, Department of Physiotherapy, SSSIHMS, Bangalore, in providing postoperative physiotherapy and rehabilitative care for the patient.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Thakar, S., Sivaraju, L., Ghosal, N. et al. Fatal holocord recurrence of a pregnancy-related, low-grade spinal ependymoma: case report and review of an unusual clinical phenomenon. Spinal Cord Ser Cases 6, 93 (2020). https://doi.org/10.1038/s41394-020-00343-9
Received:
Revised:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41394-020-00343-9
