
Abstract
Introduction
Discovering the source of a patient’s fever, in the absence of clinical localizing signs, can be a formidable undertaking. Without a clear symptom pattern to narrow the focus of a diagnostic workup, this task can require numerous noninvasive and invasive procedures, imaging studies, and laboratory tests to arrive at a conclusion. Identifying the source of a patient’s fever in the setting of an acute spinal cord injury can present a unique challenge because this population is at risk for many different conditions that can cause fever, some of which are rarely seen in the general population.
Case presentation
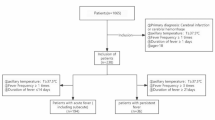
This case report describes a unique case and diagnostic workup of fever of unknown origin in a 51-year-old male with multiple medical comorbidities who presented to an inpatient rehabilitation service following an acute traumatic cervical spinal cord injury. Ultimately, it was determined that the patient had several different factors that were causing him to have intermittent fevers over a 5-week period.
Discussion
This case demonstrates the importance of obtaining serial medical histories and physical examinations during the investigation for fever of unknown origin. It also supports why additional workup of a patient’s fever may need to be considered even after a potential source is found. Finally, it demonstrates the need for increased awareness of quadriplegic fever so that this condition can be more effectively recognized, prevented, and managed in the future.
Similar content being viewed by others

Log in or create a free account to read this content
Gain free access to this article, as well as selected content from this journal and more on nature.com
or
References
Arnow PM, Flaherty JP. Fever of Unknown Origin. Lancet. 1997;350:575–80.
Vanderschueren S, Knockaert D, Adriaenssens T, Demey W, Durnez A, Blockmans D, et al. From prolonged febrile illness to fever of unknown origin: the challenge continues. Arch Intern Med. 2003;163:1033–41.
Mourad O, Palda V, Detsky A. A Comprehensive Evidence-Based Approach to Fever of Unknown Origin. Arch Intern Med. 2003;163:545.
Petersdorf RG, Beeson PB. Fever of unexplained origin: report on 100 cases. Medicine (Baltimore). 1961;40:1–30.
Durack DT, Street AC. Fever of unknown origin — reexamined and redefined. Curr Clin Top Infect Dis. 1991;11:35–51.
Sugarman B, Brown D, Musher D. Fever and infection in spinal cord injury patients. JAMA. 1982;248:66–70.
Price MJ, Trbovich M. Thermoregulation following spinal cord injury. Handb Clin Neurol. 2018;157:799–820.
Savage KE, Oleson CV, Schroeder GD, Sidhu GS, Vaccaro AR. Neurogenic fever after acute traumatic spinal cord injury: A qualitative systematic review. Global Spine J. 2016;6:607–14.
Held KS, Lane TE. Spinal cord injury, immunodepression, and antigenic challenge. Semin Immunol. 2014;26:415–20.
Colachis SC, Otis SM. Occurrence of fever associated with thermoregulatory dysfunction after acute traumatic spinal cord injury. Am J Phys Med Rehabil. 1995;74:114–9.
Yu CG, Jagid J, Ruenes G, Dietrich WD, Marcillo AE, Yezierski RP. Detrimental effects of systemic hyperthermia on locomotor function and histopathological outcome after traumatic spinal cord injury in the rat. Neurosurgery. 2001;49:152–8.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Connolly, B.R., Harden, J.K. An approach to the management of fever of unknown origin in the setting of acute spinal cord injury. Spinal Cord Ser Cases 7, 19 (2021). https://doi.org/10.1038/s41394-021-00385-7
Received:
Revised:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41394-021-00385-7
