
Abstract
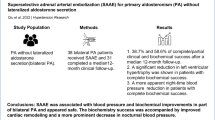
Superselective adrenal artery embolization (SAAE) offers a novel approach for treating primary aldosteronism (PA). In this study, we aimed to assess the efficacy and safety of SAAE for the treatment of PA based on the lateralization results obtained from adrenal vein sampling (AVS).In this prospective study, we enrolled 40 patients with PA who underwent SAAE. The patients were categorized into two groups, unilateral PA and bilateral PA, based on AVS results. Clinical parameters and biochemical markers were assessed at 3 and 12 months postoperatively. The primary outcomes were changes in blood pressure and defined daily dose (DDD) of antihypertensive medications compared to baseline. Thirty-eight patients achieved technical success, with favorable clinical and biochemical efficacy rates. At three months postoperatively, the clinical efficacy rates were 79.2% and 78.6% for the UPA and BPA groups, respectively. At 12 months, the rates were 83.3% and 71.4%, respectively. Both groups exhibited a significant decrease in average blood pressure at 3 and 12 months compared with baseline (P < 0.001), and there was also a notable reduction in DDD (P < 0.05). At three months, the biochemical efficacy rates were 61.9% and 58.3% in the UPA and BPA groups, respectively. Due to loss to follow-up, biochemical indicators were not assessed at 12 months postoperatively. No severe adverse reactions occurred during or after SAAE. Patients with both UPA and BPA can benefit from SAAE. The superiority of bilateral adrenal artery embolization in the treatment of BPA over unilateral adrenal artery embolization requires further investigation.

This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$259.00 per year
only $21.58 per issue
Buy this article
- Purchase on SpringerLink
- Instant access to the full article PDF.
USD 39.95
Prices may be subject to local taxes which are calculated during checkout
Similar content being viewed by others


References
Funder JW, Carey RM, Mantero F, Murad MH, Reincke M, Shibata H, et al. The management of primary aldosteronism: case detection, diagnosis, and treatment: an endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2016;101:1889–916.
Young WF Jr. Diagnosis and treatment of primary aldosteronism: practical clinical perspectives. J Intern Med. 2019;285:126–48.
Huang KH, Yu CC, Hu YH, Chang CC, Chan CK, Liao SC, et al. TAIPAI, Taiwan Primary Aldosteronism Investigator. Targeted treatment of primary aldosteronism - The consensus of Taiwan Society of Aldosteronism. J Formos Med Assoc. 2019;118:72–82.
Rossi GP, Bisogni V, Bacca AV, Belfiore A, Cesari M, et al. The 2020 Italian Society of Arterial Hypertension (SIIA) practical guidelines for the management of primary aldosteronism. Int J Cardiol Hypertens. 2020;5:100029.
Mulatero P, Sechi LA, Williams TA, Lenders JWM, Reincke M, Satoh F, et al. Subtype diagnosis, treatment, complications and outcomes of primary aldosteronism and future direction of research: a position statement and consensus of the Working Group on Endocrine Hypertension of the European Society of Hypertension. J Hypertens. 2020;38:1929–36.
Naruse M, Katabami T, Shibata H, Sone M, Takahashi K, Tanabe A, et al. Japan Endocrine Society clinical practice guideline for the diagnosis and management of primary aldosteronism 2021. Endocr J. 2022;69:327–59.
Hundemer GL, Curhan GC, Yozamp N, Wang M, Vaidya A. Cardiometabolic outcomes and mortality in medically treated primary aldosteronism: a retrospective cohort study. Lancet Diab Endocrinol. 2018;6:51–9.
Monticone S, D’Ascenzo F, Moretti C, Williams TA, Veglio F, et al. Cardiovascular events and target organ damage in primary aldosteronism compared with essential hypertension: a systematic review and meta-analysis. Lancet Diab Endocrinol. 2018;6:41–50.
Tezuka Y, Turcu AF. Real-world effectiveness of mineralocorticoid receptor antagonists in primary aldosteronism. Front Endocrinol. 2021;12:625457.
Deinum J, Riksen NP, Lenders JW. Pharmacological treatment of aldosterone excess. Pharmacol Ther. 2015;154:120–33.
Stavropoulos K, Papadopoulos C, Koutsampasopoulos K, Lales G, Mitas C, Doumas M. Mineralocorticoid receptor antagonists in primary aldosteronism. Curr Pharm Des. 2018;24:5508–16.
Young WF. Primary aldosteronism: renaissance of a syndrome. Clin Endocrinol. 2007;66:607–18.
Wang X, Luo Q, Wang M, Hu J, Zhang D, Zhang W, et al. Long-term impact of spironolactone compliance on microalbuminuria in patients with primary aldosteronism. Hypertens Res. 2021;44:426–34.
Araujo-Castro M, Paja Fano M, González Boillos M, Pla Peris B, Pascual-Corrales E, García Cano AM, et al. Evolution of the cardiometabolic profile of primary hyperaldosteronism patients treated with adrenalectomy and with mineralocorticoid receptor antagonists: results from the SPAIN-ALDO Registry. Endocrine. 2022;6:687–96.
Chen YL, Xu TY, Xu JZ, Zhu LM, Li Y, et al. A prospective comparative study on cardiac alterations after surgery and drug treatment of primary aldosteronism. Front Endocrinol. 2021;12:770711.
Zennaro MC, Boulkroun S, Fernandes-Rosa FL. Pathogenesis and treatment of primary aldosteronism. Nat Rev Endocrinol. 2020;16:578–89.
Hundemer GL, Vaidya A. Management of endocrine disease: the role of surgical adrenalectomy in primary aldosteronism. Eur J Endocrinol. 2020;183:R185–96.
Hokotate H, Inoue H, Baba Y, Tsuchimochi S, Nakajo M. Aldosteronomas: experience with superselective adrenal arterial embolization in 33 cases. Radiology. 2003;227:401–6.
Zhang H, Li Q, Liu X, Zhao Z, He H, et al. Adrenal artery ablation for primary aldosteronism without apparent aldosteronoma: an efficacy and safety, proof-of-principle trial. J Clin Hypertens. 2020;22:1618–26.
Dong H, Zou Y, He J, Deng Y, Chen Y, Song L, et al. Superselective adrenal arterial embolization for idiopathic hyperaldosteronism: 12-month results from a proof-of-principle trial. Catheter Cardiovasc Interv. 2021;97:976–81.
Qiu J, Li N, Xiong HL, Yang J, Li YD, Hu CK, et al. Superselective adrenal arterial embolization for primary aldosteronism without lateralized aldosterone secretion: an efficacy and safety, proof-of-principle study. Hypertens Res. 2023;46:1297–310.
ElSayed NA, Aleppo G, Aroda VR, Bannuru RR, Brown FM, Bruemmer D, et al. 2. Classification and diagnosis of diabetes: standards of care in Diabetes-2023. Diabetes Care. 2023;46:S19–40.
Williams TA, Lenders JWM, Mulatero P, Burrello J, Rottenkolber M, Adolf C, et al. Outcomes after adrenalectomy for unilateral primary aldosteronism: an international consensus on outcome measures and analysis of remission rates in an international cohort. Lancet Diabetes Endocrinol. 2017;5:689–99.
Sun F, Liu X, Zhang H, Zhou X, Zhao Z, He H, et al. Catheter-based adrenal ablation: an alternative therapy for patients with aldosterone-producing adenoma. Hypertens Res. 2023;46:91–9.
Yang S, Wang G, Li N, Zhu Q. The outcomes of transcatheter adrenal ablation in patients with primary aldosteronism: a systematic review and meta-analysis. BMC Endocr Disord. 2023;23:103.
Zhao Z, Liu X, Zhang H, Li Q, He H, Yan Z, et al. Catheter-based adrenal ablation remits primary aldosteronism: a randomized medication-controlled trial. Circulation. 2021;144:580–2.
Weinberger MH, Grim CE, Hollifield JW, Kem DC, Ganguly A, Kramer NJ, et al. Primary aldosteronism: diagnosis, localization, and treatment. Ann Intern Med. 1979;90:386–95.
Sukor N, Gordon RD, Ku YK, Jones M, Stowasser M. Role of unilateral adrenalectomy in bilateral primary aldosteronism: a 22-year single center experience. J Clin Endocrinol Metab. 2009;94:2437–45.
Lu YC, Liu KL, Wu VC, Wang SM, Lin YH, Chueh SJ, et al. Unilateral adrenalectomy in bilateral adrenal hyperplasia with primary aldosteronism. J Formos Med Assoc. 2023;122:393–9.
Szabo Yamashita T, Shariq OA, Foster TR, Lyden ML, Dy BM, Young WF, et al. Unilateral adrenalectomy for primary aldosteronism due to bilateral adrenal disease can result in resolution of hypokalemia and amelioration of hypertension. World J Surg. 2023;47:314–8.
Moran W, Goetz FC, Melby J, Zimmermann B, Kennedy BJ. Primary hyperaldosteronism without adrenal tumor. Am J Med. 1960;28:638–47.
Marín-Martínez L, Ríos-Vergara AJ, Kyriakos G, Álvarez-Martín MC, Hernández-Alonso E. Bilateral adrenalectomy in a patient with refractory primary aldosteronism due to adrenal hyperplasia. Cureus. 2022;14:e24267.
Therien B, Mellinger RC, Caldwell JR, Howard PJ.Primary aldosteronism due to adrenal hyperplasia; occurrence in a boy aged 10 years.AMA J Dis Child. 1959;98:90–9.
Aune A, Gerdts E, Kokorina M, Kringeland E, Midtbø H, Løvås K, et al. Persistent cardiac organ damage in surgically and medically treated primary aldosteronism. J Hypertens. 2022;40:1204–11.
Catena C, Colussi GL, Marzano L, Sechi LA. Predictive factors of left ventricular mass changes after treatment of primary aldosteronism. Horm Metab Res. 2012;44:188–93.
Huang M, Li J, Zhao X, Fu R, Li X, Jiang W. Global and regional prevalence and cardiovascular risk of primary aldosteronism: a systematic review and meta-analysis. Curr Probl Cardiol. 2024;49:102791.
Nanba K, Rainey WE. Genetics in endocrinology: impact of race and sex on genetic causes of aldosterone-producing adenomas. Eur J Endocrinol. 2021;185:R1–11.
Acknowledgements
We thank He-Xuan Zhang (Army Specialty Medical Center, Army Medical University, Chongqing, China) for his guidance and advice on our adrenal artery embolization efforts. We thank Guo-Shu Wang (The First Affiliated Hospital of Chongqing Medical University, Chongqing, China) for his guidance in the imaging of the re-adrenal gland.
Author information
Authors and Affiliations
Corresponding authors
Ethics declarations
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Li, X., Feng, R., Xiang, R. et al. Bilateral superselective adrenal artery embolization for bilateral primary aldosteronism: a novel approach in an efficacy and safety proof-of-principle trial. Hypertens Res 48, 189–199 (2025). https://doi.org/10.1038/s41440-024-01881-7
Received:
Revised:
Accepted:
Published:
Version of record:
Issue date:
DOI: https://doi.org/10.1038/s41440-024-01881-7
Keywords
This article is cited by
-
68Ga-Pentixafor PET/CT for the assessment of therapeutic outcomes following superselective adrenal arterial embolization in patients with primary aldosteronism
EJNMMI Research (2025)
-
The application value of ipsilateral superselective adrenal arteriography and adrenal venography in patients with primary aldosteronism undergoing adrenal artery embolization
Hypertension Research (2025)
