
Abstract
The therapeutic scope of sodium–glucose cotransporter 2 (SGLT2) inhibitors has expanded beyond glycaemic regulation in the management of diabetes mellitus. Studies published in the past few years highlight their substantial effect on cardiovascular outcomes, notably in decreasing mortality and the need for heart failure-related hospitalization. These agents also lead to pronounced improvements in a range of renal outcomes. The primary actions of SGLT2 inhibition, glycosuria and natriuresis, are pivotal in enhancing glucose control, promoting weight loss and lowering blood pressure. These effects initiate a series of beneficial mechanisms: facilitating haemodynamic improvement by reducing interstitial volume, enhancing cardiac function, boosting energy efficiency through altered ketone body metabolism and mitigating inflammation and oxidative stress. Additional effects include heightened erythropoiesis, reduced hyperuricaemia and increased levels of angiotensin-converting enzyme 2 and angiotensin (1–7). SGLT2 inhibitors also attenuate sympathetic overactivity by modulating neurohumoral activation and renal afferent signalling, contributing to their cardioprotective and renoprotective profiles. This Review provides a comprehensive overview of the diverse mechanisms underpinning the cardiometabolic and renal effects of SGLT2 inhibitors, emphasizing their clinical relevance and therapeutic potential.
Key points
-
Clinical trials have demonstrated the therapeutic role of SGLT2 inhibitors beyond glycaemic control, and have demonstrated clinical benefits for cardiometabolic and renal outcomes mediated through multiple direct and indirect mechanisms.
-
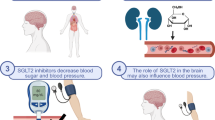
SGLT2 inhibition in the kidney induces glycosuria and natriuresis, resulting in reduced blood levels of glucose and sodium, which in turn contribute to weight loss and blood pressure reduction.
-
Haemodynamic effects combined with attenuation of sympathetic activity through SGLT2 inhibition are crucial for preventing progression of heart failure and chronic kidney disease.
-
SGLT2 inhibition can systematically induce metabolic shifts (reprogramming) towards ketogenesis and promote autophagy with anti-inflammatory and anti-fibrotic effects.
-
Major adverse effects of SGLT2 inhibitors include hypovolaemia due to osmotic diuresis, genital tract infection and euglycaemic ketoacidosis.
This is a preview of subscription content, access via your institution
Access options
Access Nature and 54 other Nature Portfolio journals
Get Nature+, our best-value online-access subscription
$32.99 / 30 days
cancel any time
Subscribe to this journal
Receive 12 print issues and online access
$189.00 per year
only $15.75 per issue
Buy this article
- Purchase on SpringerLink
- Instant access to the full article PDF.
USD 39.95
Prices may be subject to local taxes which are calculated during checkout


Similar content being viewed by others


References
Zinman, B. et al. Empagliflozin, cardiovascular outcomes, and mortality in type 2 diabetes. N. Engl. J. Med. 373, 2117–2128 (2015).
Neal, B. et al. Canagliflozin and cardiovascular and renal events in type 2 diabetes. N. Engl. J. Med. 377, 644–657 (2017).
Wiviott, S. D. et al. Dapagliflozin and cardiovascular outcomes in type 2 diabetes. N. Engl. J. Med. 380, 347–357 (2019).
Bhatt, D. L. et al. Sotagliflozin in patients with diabetes and chronic kidney disease. N. Engl. J. Med. 384, 129–139 (2021).
Perkovic, V. et al. Canagliflozin and renal outcomes in type 2 diabetes and nephropathy. N. Engl. J. Med. 380, 2295–2306 (2019).
The EMPA-KIDNEY Collaborative Group. Empagliflozin in patients with chronic kidney disease. N. Engl. J. Med. 388, 117–127 (2023).
Heerspink, H. J. L. et al. Dapagliflozin in patients with chronic kidney disease. N. Engl. J. Med. 383, 1436–1446 (2020).
Packer, M. et al. Cardiovascular and renal outcomes with empagliflozin in heart failure. N. Engl. J. Med. 383, 1413–1424 (2020).
Anker, S. D. et al. Empagliflozin in heart failure with a preserved ejection fraction. N. Engl. J. Med. 385, 1451–1461 (2021).
Bhatt, D. L. et al. Sotagliflozin in patients with diabetes and recent worsening heart failure. N. Engl. J. Med. 384, 117–128 (2021).
McMurray, J. J. V. et al. Dapagliflozin in patients with heart failure and reduced ejection fraction. N. Engl. J. Med. 381, 1995–2008 (2019).
Solomon, S. D. et al. Dapagliflozin in heart failure with mildly reduced or preserved ejection fraction. N. Engl. J. Med. 387, 1089–1098 (2022).
Moon, J. S. et al. 2023 clinical practice guidelines for diabetes management in Korea: full version recommendation of the Korean Diabetes Association. Diabetes Metab. J. 48, 546–708 (2024).
Shi, Q. et al. Benefits and harms of drug treatment for type 2 diabetes: systematic review and network meta-analysis of randomised controlled trials. BMJ 381, e074068 (2023).
Cannon, C. P. et al. Cardiovascular outcomes with ertugliflozin in type 2 diabetes. N. Engl. J. Med. 383, 1425–1435 (2020).
Nassif, M. E. et al. The SGLT2 inhibitor dapagliflozin in heart failure with preserved ejection fraction: a multicenter randomized trial. Nat. Med. 27, 1954–1960 (2021).
Filippatos, G. et al. Empagliflozin for heart failure with preserved left ventricular ejection fraction with and without diabetes. Circulation 146, 676–686 (2022).
Usman, M. S. et al. Effect of SGLT2 inhibitors on heart failure outcomes and cardiovascular death across the cardiometabolic disease spectrum: a systematic review and meta-analysis. Lancet Diabetes Endocrinol. 12, 447–461 (2024).
Vallon, V. & Verma, S. Effects of SGLT2 inhibitors on kidney and cardiovascular function. Annu. Rev. Physiol. 83, 503–528 (2021).
Ferrannini, E. Sodium-glucose co-transporters and their inhibition: clinical physiology. Cell Metab. 26, 27–38 (2017).
Ferrannini, E. et al. Metabolic response to sodium-glucose cotransporter 2 inhibition in type 2 diabetic patients. J. Clin. Invest. 124, 499–508 (2014).
Santos-Gallego, C. G. et al. Empagliflozin ameliorates adverse left ventricular remodeling in nondiabetic heart failure by enhancing myocardial energetics. J. Am. Coll. Cardiol. 73, 1931–1944 (2019).
Lee, S. G. et al. Dapagliflozin attenuates diabetes-induced diastolic dysfunction and cardiac fibrosis by regulating SGK1 signaling. BMC Med. 20, 309 (2022).
Lee, T. M., Chang, N. C. & Lin, S. Z. Dapagliflozin, a selective SGLT2 inhibitor, attenuated cardiac fibrosis by regulating the macrophage polarization via STAT3 signaling in infarcted rat hearts. Free. Radic. Biol. Med. 104, 298–310 (2017).
Lim, S., Oh, T. J., Dawson, J. & Sattar, N. Diabetes drugs and stroke risk: intensive versus conventional glucose-lowering strategies, and implications of recent cardiovascular outcome trials. Diabetes Obes. Metab. 22, 6–15 (2020).
Ahn, C. H. & Lim, S. Effects of thiazolidinedione and new antidiabetic agents on stroke. J. Stroke 21, 139–150 (2019).
Lim, S., Sohn, M. & Nauck, M. A. Cardiovascular outcome with SGLT2i and GLP1RA. Eur. J. Intern. Med. 129, 133–136 (2024).
Pasqualotto, E. et al. The effect of sodium-glucose transporter 2 inhibitors on stroke in patients with type 2 diabetes: a meta-analysis. J. Stroke Cerebrovasc. Dis. 33, 107730 (2024).
Tian, Q., Guo, K., Deng, J., Zhong, Y. & Yang, L. Effects of SGLT2 inhibitors on haematocrit and haemoglobin levels and the associated cardiorenal benefits in T2DM patients: a meta-analysis. J. Cell Mol. Med. 26, 540–547 (2022).
Katakami, N. et al. Effect of tofogliflozin on arterial stiffness in patients with type 2 diabetes: prespecified sub-analysis of the prospective, randomized, open-label, parallel-group comparative UTOPIA trial. Cardiovasc. Diabetol. 20, 4 (2021).
Rizos, E. C. et al. The effect of SGLT2 inhibitors and GLP1 receptor agonists on arterial stiffness: a meta-analysis of randomized controlled trials. J. Diabetes Complicat. 38, 108781 (2024).
Akbari, A., Hadizadeh, S. & Heidary, L. Effects of glucagon-like peptide-1 receptor agonists and sodium-glucose cotransporter 2 inhibitors on intima-media thickness: systematic review and meta-analysis. J. Diabetes Res. 2024, 3212795 (2024).
Shigiyama, F. et al. Effectiveness of dapagliflozin on vascular endothelial function and glycemic control in patients with early-stage type 2 diabetes mellitus: DEFENCE study. Cardiovasc. Diabetol. 16, 84 (2017).
Butler, J. et al. Empagliflozin after acute myocardial infarction. N. Engl. J. Med. 390, 1455–1466 (2024).
Fujiki, S. et al. Effect of empagliflozin on ventricular arrhythmias in patients with type 2 diabetes treated with an implantable cardioverter-defibrillator: the EMPA-ICD trial. Cardiovasc. Diabetol. 23, 224 (2024).
Wang, X. et al. Association of sodium-glucose cotransporter 2 inhibitors (SGLT2i) with cardiac arrhythmias: a systematic review and meta-analysis of cardiovascular outcome trials. Rev. Cardiovasc. Med. 24, 258 (2023).
Zhan, G. et al. Dapagliflozin: a sodium-glucose cotransporter 2 inhibitor, attenuates angiotensin II-induced atrial fibrillation by regulating atrial electrical and structural remodeling. Eur. J. Pharmacol. 978, 176712 (2024).
Mustroph, J. et al. Empagliflozin inhibits cardiac late sodium current by Ca/calmodulin-dependent kinase II. Circulation 146, 1259–1261 (2022).
Muller, M. E. et al. Electrophysiological effects of the sodium-glucose co-transporter-2 (SGLT2) inhibitor dapagliflozin on human cardiac potassium channels. Int. J. Mol. Sci. 25, 5701 (2024).
Kidney Disease: Improving Global Outcomes (KDIGO) CKD Working Group. KDIGO 2024 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int. 105, S117–S314 (2024).
Fioretto, P., Stefansson, B. V., Johnsson, E., Cain, V. A. & Sjostrom, C. D. Dapagliflozin reduces albuminuria over 2 years in patients with type 2 diabetes mellitus and renal impairment. Diabetologia 59, 2036–2039 (2016).
Ferreira, J. P. et al. Association of empagliflozin treatment with albuminuria levels in patients with heart failure: a secondary analysis of EMPEROR-pooled. JAMA Cardiol. 7, 1148–1159 (2022).
Sohn, M., Dietrich, J. W., Nauck, M. A. & Lim, S. Characteristics predicting the efficacy of SGLT-2 inhibitors versus GLP-1 receptor agonists on major adverse cardiovascular events in type 2 diabetes mellitus: a meta-analysis study. Cardiovasc. Diabetol. 22, 153 (2023).
Cherney, D. Z. I. et al. Effects of the SGLT2 inhibitor dapagliflozin on proteinuria in non-diabetic patients with chronic kidney disease (DIAMOND): a randomised, double-blind, crossover trial. Lancet Diabetes Endocrinol. 8, 582–593 (2020).
Tuttle, K. R. et al. Efficacy and safety of aldosterone synthase inhibition with and without empagliflozin for chronic kidney disease: a randomised, controlled, phase 2 trial. Lancet 403, 379–390 (2024).
Smeijer, J. D. et al. Endothelin receptor antagonists in chronic kidney disease. Nat. Rev. Nephrol. 21, 175–188 (2025).
Farias, R. S. et al. Inhibition of SGLT2 co-transporter by dapagliflozin ameliorates tubular proteinuria and tubule-interstitial injury at the early stage of diabetic kidney disease. Eur. J. Pharmacol. 942, 175521 (2023).
Lee, H. C. et al. The sodium-glucose co-transporter 2 inhibitor empagliflozin attenuates cardiac fibrosis and improves ventricular hemodynamics in hypertensive heart failure rats. Cardiovasc. Diabetol. 18, 45 (2019).
Cassis, P. et al. SGLT2 inhibitor dapagliflozin limits podocyte damage in proteinuric nondiabetic nephropathy. JCI Insight 3, e98720 (2018).
Davies, M. J., Trujillo, A., Vijapurkar, U., Damaraju, C. V. & Meininger, G. Effect of canagliflozin on serum uric acid in patients with type 2 diabetes mellitus. Diabetes Obes. Metab. 17, 426–429 (2015).
Zhao, Y. et al. Effects of sodium-glucose co-transporter 2 (SGLT2) inhibitors on serum uric acid level: a meta-analysis of randomized controlled trials. Diabetes Obes. Metab. 20, 458–462 (2018).
Tesfaye, H. et al. Empagliflozin and risk of incident gout: analysis from the empagliflozin comparative effectiveness and SafEty (EMPRISE) cohort study. J. Gen. Intern. Med. 39, 1870–1879 (2024).
Spiga, R. et al. Uric acid is associated with inflammatory biomarkers and induces inflammation via activating the NF-κB signaling pathway in HepG2 cells. Arterioscler. Thromb. Vasc. Biol. 37, 1241–1249 (2017).
Chino, Y. et al. SGLT2 inhibitor lowers serum uric acid through alteration of uric acid transport activity in renal tubule by increased glycosuria. Biopharm. Drug. Dispos. 35, 391–404 (2014).
Billing, A. M. et al. Metabolic communication by SGLT2 inhibition. Circulation 149, 860–884 (2024).
Cefalu, W. T. et al. Efficacy and safety of canagliflozin versus glimepiride in patients with type 2 diabetes inadequately controlled with metformin (CANTATA-SU): 52 week results from a randomised, double-blind, phase 3 non-inferiority trial. Lancet 382, 941–950 (2013).
Palmer, S. C. et al. Sodium-glucose cotransporter protein-2 (SGLT-2) inhibitors and glucagon-like peptide-1 (GLP-1) receptor agonists for type 2 diabetes: systematic review and network meta-analysis of randomised controlled trials. BMJ 372, m4573 (2021).
Lim, S., Sohn, M., Shin, Y. & Ferrannini, E. Initial combination of metformin, sitagliptin, and empagliflozin in drug-naive patients with type 2 diabetes: safety and metabolic effects. Diabetes Obes. Metab. 24, 757–762 (2022).
Merovci, A. et al. Dapagliflozin improves muscle insulin sensitivity but enhances endogenous glucose production. J. Clin. Invest. 124, 509–514 (2014).
Ferrannini, G. et al. Energy balance after sodium-glucose cotransporter 2 inhibition. Diabetes Care 38, 1730–1735 (2015).
Kang, S. M., Yun, H. M., Sohn, M. & Lim, S. Vascular and metabolic effects of ipragliflozin versus sitagliptin (IVS) in type 2 diabetes treated with sulphonylurea and metformin: IVS study. Diabetes Obes. Metab. 25, 1922–1931 (2023).
Shin, Y., Choi, H. & Lim, S. Comparison betweeen dapagliflozin add-on therapy and insulin dose escalation in patients with uncontrolled type 2 diabetes treated with insulin: DVI study. Diabetes Res. Clin. Pract. 175, 108843 (2021).
Vasilakou, D. et al. Sodium-glucose cotransporter 2 inhibitors for type 2 diabetes: a systematic review and meta-analysis. Ann. Intern. Med. 159, 262–274 (2013).
Bolinder, J. et al. Effects of dapagliflozin on body weight, total fat mass, and regional adipose tissue distribution in patients with type 2 diabetes mellitus with inadequate glycemic control on metformin. J. Clin. Endocrinol. Metab. 97, 1020–1031 (2012).
Shin, Y., Moon, J. H., Chin, H. J., Ferrannini, E. & Lim, S. Glycemic efficacy and metabolic consequences of an empagliflozin add-on versus conventional dose-increasing strategy in patients with type 2 diabetes inadequately controlled by metformin and sulfonylurea. Endocrinol. Metab. 35, 329–338 (2020).
Han, E., Lee, Y. H., Lee, B. W., Kang, E. S. & Cha, B. S. Ipragliflozin additively ameliorates non-alcoholic fatty liver disease in patients with type 2 diabetes controlled with metformin and pioglitazone: a 24-week randomized controlled trial. J. Clin. Med. 9, 259 (2020).
Sargeant, J. A. et al. A review of the effects of glucagon-like peptide-1 receptor agonists and sodium-glucose cotransporter 2 inhibitors on lean body mass in humans. Endocrinol. Metab. 34, 247–262 (2019).
Iacobellis, G. & Gra-Menendez, S. Effects of dapagliflozin on epicardial fat thickness in patients with type 2 diabetes and obesity. Obesity 28, 1068–1074 (2020).
Sargeant, J. A. et al. The effects of empagliflozin, dietary energy restriction, or both on appetite-regulatory gut peptides in individuals with type 2 diabetes and overweight or obesity: the SEESAW randomized, double-blind, placebo-controlled trial. Diabetes Obes. Metab. 24, 1509–1521 (2022).
Yates, T. et al. Initiation of new glucose-lowering therapies may act to reduce physical activity levels: pooled analysis from three randomized trials. Diabetes Care 45, 2749–2752 (2022).
Miao, L., Targher, G., Byrne, C. D., Cao, Y.-Y. & Zheng, M.-H. Current status and future trends of the global burden of MASLD. Trends Endocrinol. Metab. 35, 697–707 (2024).
Lee, H. H. et al. Metabolic dysfunction-associated steatotic liver disease and risk of cardiovascular disease. Gut 73, 533–540 (2023).
Song, T. et al. Meta-analysis of the effect of sodium-glucose cotransporter 2 inhibitors on hepatic fibrosis in patients with type 2 diabetes mellitus complicated with non-alcoholic fatty liver disease. Hepatol. Res. 51, 641–651 (2021).
Moon, J. S. et al. SGLT-2 inhibitors and GLP-1 receptor agonists in metabolic dysfunction-associated fatty liver disease. Trends Endocrinol. Metab. 33, 424–442 (2022).
Kuchay, M. S. et al. Effect of empagliflozin on liver fat in patients with type 2 diabetes and nonalcoholic fatty liver disease: a randomized controlled trial (E-LIFT trial). Diabetes Care 41, 1801–1808 (2018).
Chehrehgosha, H. et al. Empagliflozin improves liver steatosis and fibrosis in patients with non-alcoholic fatty liver disease and type 2 diabetes: a randomized, double-blind, placebo-controlled clinical trial. Diabetes Ther. 12, 843–861 (2021).
Akuta, N. et al. Impact of sodium glucose cotransporter 2 inhibitor on histological features and glucose metabolism of non-alcoholic fatty liver disease complicated by diabetes mellitus. Hepatol. Res. 49, 531–539 (2019).
Srikanth, V., Sinclair, A. J., Hill-Briggs, F., Moran, C. & Biessels, G. J. Type 2 diabetes and cognitive dysfunction-towards effective management of both comorbidities. Lancet Diabetes Endocrinol. 8, 535–545 (2020).
Wiciński, M., Wódkiewicz, E., Górski, K., Walczak, M. & Malinowski, B. Perspective of SGLT2 inhibition in treatment of conditions connected to neuronal loss: focus on Alzheimer’s disease and ischemia-related brain injury. Pharmaceuticals 13, 379 (2020).
Yamato, M., Kato, N., Yamada, K. I. & Inoguchi, T. The early pathogenesis of diabetic retinopathy and its attenuation by sodium-glucose transporter 2 inhibitors. Diabetes 73, 1153–1166 (2024).
Sim, A. Y. et al. SGLT2 and DPP4 inhibitors improve Alzheimer’s disease-like pathology and cognitive function through distinct mechanisms in a T2D-AD mouse model. Biomed. Pharmacother. 168, 115755 (2023).
Mone, P. et al. Empagliflozin improves cognitive impairment in frail older adults with type 2 diabetes and heart failure with preserved ejection fraction. Diabetes Care 45, 1247–1251 (2022).
Wu, C. Y. et al. Association of sodium-glucose cotransporter 2 inhibitors with time to dementia: a population-based cohort study. Diabetes Care 46, 297–304 (2023).
Ferrannini, E. et al. Role of glycosuria in SGLT2 inhibitor-induced cardiorenal protection: a mechanistic analysis of the CREDENCE trial. Diabetes 73, 250–259 (2024).
Packer, M. SGLT2 inhibitors: role in protective reprogramming of cardiac nutrient transport and metabolism. Nat. Rev. Cardiol. 20, 443–462 (2023).
Kim, J. H. et al. Sodium-glucose cotransporter 2 inhibitors regulate ketone body metabolism via inter-organ crosstalk. Diabetes Obes. Metab. 21, 801–811 (2019).
Suga, T. et al. Ipragliflozin-induced improvement of liver steatosis in obese mice may involve sirtuin signaling. World J. Hepatol. 12, 350–362 (2020).
Koyani, C. N. et al. Empagliflozin protects heart from inflammation and energy depletion via AMPK activation. Pharmacol. Res. 158, 104870 (2020).
Yurista, S. R. et al. Sodium-glucose co-transporter 2 inhibition with empagliflozin improves cardiac function in non-diabetic rats with left ventricular dysfunction after myocardial infarction. Eur. J. Heart Fail. 21, 862–873 (2019).
Lee, Y. H. et al. Empagliflozin attenuates diabetic tubulopathy by improving mitochondrial fragmentation and autophagy. Am. J. Physiol. Ren. Physiol. 317, F767–F780 (2019).
Fukushima, K., Kitamura, S., Tsuji, K., Sang, Y. & Wada, J. Sodium glucose co-transporter 2 inhibitor ameliorates autophagic flux impairment on renal proximal tubular cells in obesity mice. Int. J. Mol. Sci. 21, 4054 (2020).
Moellmann, J. et al. The sodium-glucose co-transporter-2 inhibitor ertugliflozin modifies the signature of cardiac substrate metabolism and reduces cardiac mTOR signalling, endoplasmic reticulum stress and apoptosis. Diabetes Obes. Metab. 24, 2263–2272 (2022).
Mone, P. et al. SGLT2 inhibition via empagliflozin improves endothelial function and reduces mitochondrial oxidative stress: insights from frail hypertensive and diabetic patients. Hypertension 79, 1633–1643 (2022).
van Bommel, E. J. M. et al. The renal hemodynamic effects of the SGLT2 inhibitor dapagliflozin are caused by post-glomerular vasodilatation rather than pre-glomerular vasoconstriction in metformin-treated patients with type 2 diabetes in the randomized, double-blind RED trial. Kidney Int. 97, 202–212 (2020).
Cherney, D. Z. et al. Renal hemodynamic effect of sodium-glucose cotransporter 2 inhibition in patients with type 1 diabetes mellitus. Circulation 129, 587–597 (2014).
Kraus, B. J. et al. Characterization and implications of the initial estimated glomerular filtration rate ‘dip’ upon sodium-glucose cotransporter-2 inhibition with empagliflozin in the EMPA-REG OUTCOME trial. Kidney Int. 99, 750–762 (2021).
Jongs, N. et al. Correlates and consequences of an acute change in eGFR in response to the SGLT2 inhibitor dapagliflozin in patients with CKD. J. Am. Soc. Nephrol. 33, 2094–2107 (2022).
Ferrannini, E. et al. Shift to fatty substrate utilization in response to sodium-glucose cotransporter 2 inhibition in subjects without diabetes and patients with type 2 diabetes. Diabetes 65, 1190–1195 (2016).
Kim, S. R. et al. SGLT2 inhibition modulates NLRP3 inflammasome activity via ketones and insulin in diabetes with cardiovascular disease. Nat. Commun. 11, 2127 (2020).
Nielsen, R. et al. Cardiovascular effects of treatment with the ketone body 3-hydroxybutyrate in chronic heart failure patients. Circulation 139, 2129–2141 (2019).
Butler, J. et al. Semaglutide versus placebo in people with obesity-related heart failure with preserved ejection fraction: a pooled analysis of the STEP-HFpEF and STEP-HFpEF DM randomised trials. Lancet 403, 1635–1648 (2024).
Tomita, I. et al. SGLT2 inhibition mediates protection from diabetic kidney disease by promoting ketone body-induced mTORC1 inhibition. Cell Metab. 32, 404–419.e6 (2020).
Lopaschuk, G. D., Karwi, Q. G., Tian, R., Wende, A. R. & Abel, E. D. Cardiac energy metabolism in heart failure. Circ. Res. 128, 1487–1513 (2021).
Kato, T. et al. Analysis of metabolic remodeling in compensated left ventricular hypertrophy and heart failure. Circ. Heart Fail. 3, 420–430 (2010).
Roberts, D. J. & Miyamoto, S. Hexokinase II integrates energy metabolism and cellular protection: Akting on mitochondria and TORCing to autophagy. Cell Death Differ. 22, 248–257 (2015).
Lauritsen, K. M. et al. SGLT2 inhibition does not affect myocardial fatty acid oxidation or uptake, but reduces myocardial glucose uptake and blood flow in individuals with type 2 diabetes: a randomized double-blind, placebo-controlled crossover trial. Diabetes 70, 800–808 (2021).
Docherty, K. F. et al. Iron deficiency in heart failure and effect of dapagliflozin: findings from DAPA-HF. Circulation 146, 980–994 (2022).
Ferrannini, E. et al. Mechanisms of sodium-glucose cotransporter 2 inhibition: insights from large-scale proteomics. Diabetes Care 43, 2183–2189 (2020).
Zannad, F. et al. Effect of empagliflozin on circulating proteomics in heart failure: mechanistic insights into the EMPEROR programme. Eur. Heart J. 43, 4991–5002 (2022).
Kolkailah, A. A. et al. Effect of dapagliflozin on hematocrit in patients with type 2 diabetes at high cardiovascular risk: observations from DECLARE-TIMI 58. Diabetes Care 45, e27–e29 (2022).
Kanbay, M. et al. Effect of sodium-glucose cotransporter 2 inhibitors on hemoglobin and hematocrit levels in type 2 diabetes: a systematic review and meta-analysis. Int. Urol. Nephrol. 54, 827–841 (2022).
Fuchs Andersen, C. et al. Effects of empagliflozin on erythropoiesis in heart failure: data from the empire HF trial. Eur. J. Heart Fail. 25, 226–234 (2023).
Heyman, S. N., Armaly, Z., Hamo-Giladi, D. B. & Abassi, Z. Novel perspectives regarding the physiologic mechanisms by which gliflozins induce reticulocytosis and erythrocytosis. Am. J. Physiol. Endocrinol. Metab. 325, E621–E623 (2023).
Han, J. H. et al. The beneficial effects of empagliflozin, an SGLT2 inhibitor, on atherosclerosis in ApoE−/− mice fed a western diet. Diabetologia 60, 364–376 (2017).
Yang, Z. et al. SGLT2 inhibitor dapagliflozin attenuates cardiac fibrosis and inflammation by reverting the HIF-2α signaling pathway in arrhythmogenic cardiomyopathy. FASEB J. 36, e22410 (2022).
Kraker, K. et al. Effects of empagliflozin and target-organ damage in a novel rodent model of heart failure induced by combined hypertension and diabetes. Sci. Rep. 10, 14061 (2020).
Dihoum, A., Brown, A. J., McCrimmon, R. J., Lang, C. C. & Mordi, I. R. Dapagliflozin, inflammation and left ventricular remodelling in patients with type 2 diabetes and left ventricular hypertrophy. BMC Cardiovasc. Disord. 24, 356 (2024).
Herat, L. Y. et al. SGLT2 inhibitor-induced sympathoinhibition: a novel mechanism for cardiorenal protection. JACC Basic. Transl. Sci. 5, 169–179 (2020).
Matthews, V. B. et al. Role of the sympathetic nervous system in regulation of the sodium glucose cotransporter 2. J. Hypertens. 35, 2059–2068 (2017).
Gueguen, C. et al. Empagliflozin modulates renal sympathetic and heart rate baroreflexes in a rabbit model of diabetes. Diabetologia 63, 1424–1434 (2020).
Forrester, E. A. et al. Crucial role for sensory nerves and Na/H exchanger inhibition in dapagliflozin- and empagliflozin-induced arterial relaxation. Cardiovasc. Res. 120, 1811–1824 (2024).
Sano, M. A new class of drugs for heart failure: SGLT2 inhibitors reduce sympathetic overactivity. J. Cardiol. 71, 471–476 (2018).
Singh, J. S. S. et al. Dapagliflozin versus placebo on left ventricular remodeling in patients with diabetes and heart failure: the REFORM trial. Diabetes Care 43, 1356–1359 (2020).
Savage, P. et al. Impact of SGLT2 inhibition on markers of reverse cardiac remodelling in heart failure: systematic review and meta-analysis. Esc. Heart Fail. 11, 3636–3648 (2024).
Hundertmark, M. J. et al. Assessment of cardiac energy metabolism, function, and physiology in patients with heart failure taking empagliflozin: the randomized, controlled EMPA-VISION trial. Circulation 147, 1654–1669 (2023).
Hess, D. A. et al. SGLT2 inhibition with empagliflozin increases circulating provascular progenitor cells in people with type 2 diabetes mellitus. Cell Metab. 30, 609–613 (2019).
Zhao, Y. et al. Sodium-glucose exchanger 2 inhibitor canagliflozin promotes mitochondrial metabolism and alleviates salt-induced cardiac hypertrophy via preserving SIRT3 expression. J. Adv. Res. 70, 255–269 (2024).
Baartscheer, A. et al. Empagliflozin decreases myocardial cytoplasmic Na+ through inhibition of the cardiac Na+/H+ exchanger in rats and rabbits. Diabetologia 60, 568–573 (2017).
Onishi, A. et al. A role for tubular Na+/H+ exchanger NHE3 in the natriuretic effect of the SGLT2 inhibitor empagliflozin. Am. J. Physiol. Ren. Physiol. 319, F712–F728 (2020).
Wu, Q. et al. Dapagliflozin protects against chronic heart failure in mice by inhibiting macrophage-mediated inflammation, independent of SGLT2. Cell Rep. Med. 4, 101334 (2023).
Li, X. et al. Direct cardiac actions of the sodium glucose co-transporter 2 inhibitor empagliflozin improve myocardial oxidative phosphorylation and attenuate pressure-overload heart failure. J. Am. Heart Assoc. 10, e018298 (2021).
Ying, Y. et al. Phloretin protects against cardiac damage and remodeling via restoring SIRT1 and anti-inflammatory effects in the streptozotocin-induced diabetic mouse model. Aging 11, 2822–2835 (2019).
Sun, P. et al. Canagliflozin attenuates lipotoxicity in cardiomyocytes and protects diabetic mouse hearts by inhibiting the mTOR/HIF-1α pathway. iScience 24, 102521 (2021).
Philippaert, K. et al. Cardiac late sodium channel current is a molecular target for the sodium/glucose cotransporter 2 inhibitor empagliflozin. Circulation 143, 2188–2204 (2021).
Borges-Junior, F. A. et al. Empagliflozin inhibits proximal tubule NHE3 activity, preserves GFR, and restores euvolemia in nondiabetic rats with induced heart failure. J. Am. Soc. Nephrol. 32, 1616–1629 (2021).
Zhang, Y. et al. A sodium-glucose cotransporter 2 inhibitor attenuates renal capillary injury and fibrosis by a vascular endothelial growth factor-dependent pathway after renal injury in mice. Kidney Int. 94, 524–535 (2018).
Neuen, B. L. et al. SGLT2 inhibitors for the prevention of kidney failure in patients with type 2 diabetes: a systematic review and meta-analysis. Lancet Diabetes Endocrinol. 7, 845–854 (2019).
Park, C. H. et al. Canagliflozin protects against cisplatin-induced acute kidney injury by AMPK-mediated autophagy in renal proximal tubular cells. Cell Death Discov. 8, 12 (2022).
Kim, M. N., Moon, J. H. & Cho, Y. M. Sodium-glucose cotransporter-2 inhibition reduces cellular senescence in the diabetic kidney by promoting ketone body-induced NRF2 activation. Diabetes Obes. Metab. 23, 2561–2571 (2021).
Jaikumkao, K. et al. Dapagliflozin, a sodium-glucose co-transporter-2 inhibitor, slows the progression of renal complications through the suppression of renal inflammation, endoplasmic reticulum stress and apoptosis in prediabetic rats. Diabetes Obes. Metab. 20, 2617–2626 (2018).
Hodrea, J. et al. Reduced O-GlcNAcylation and tubular hypoxia contribute to the antifibrotic effect of SGLT2 inhibitor dapagliflozin in the diabetic kidney. Am. J. Physiol. Ren. Physiol. 318, F1017–F1029 (2020).
Shao, M. et al. Canagliflozin regulates metabolic reprogramming in diabetic kidney disease by inducing fasting-like and aestivation-like metabolic patterns. Diabetologia 67, 738–754 (2024).
Cherney, D. Z. et al. Sodium glucose cotransport-2 inhibition and intrarenal RAS activity in people with type 1 diabetes. Kidney Int. 86, 1057–1058 (2014).
Jiang, F. et al. Angiotensin-converting enzyme 2 and angiotensin 1-7: novel therapeutic targets. Nat. Rev. Cardiol. 11, 413–426 (2014).
Lim, S., Taskinen, M. R. & Boren, J. Crosstalk between nonalcoholic fatty liver disease and cardiometabolic syndrome. Obes. Rev. 20, 599–611 (2019).
Liao, X. et al. Sodium-glucose cotransporter 2 (SGLT2) inhibitor increases circulating zinc-α2-glycoprotein levels in patients with type 2 diabetes. Sci. Rep. 6, 32887 (2016).
Goldberg, E. L. et al. β-Hydroxybutyrate deactivates neutrophil NLRP3 inflammasome to relieve gout flares. Cell Rep. 18, 2077–2087 (2017).
Shimazu, T. et al. Suppression of oxidative stress by β-hydroxybutyrate, an endogenous histone deacetylase inhibitor. Science 339, 211–214 (2013).
Puchalska, P. et al. Hepatocyte-macrophage acetoacetate shuttle protects against tissue fibrosis. Cell Metab. 29, 383–398.e7 (2019).
Galsgaard, K. D., Pedersen, J., Knop, F. K., Holst, J. J. & Wewer Albrechtsen, N. J. Glucagon receptor signaling and lipid metabolism. Front. Physiol. 10, 413 (2019).
Tahara, A. et al. Effects of SGLT2 selective inhibitor ipragliflozin on hyperglycemia, hyperlipidemia, hepatic steatosis, oxidative stress, inflammation, and obesity in type 2 diabetic mice. Eur. J. Pharmacol. 715, 246–255 (2013).
Leng, W. et al. The SGLT2 inhibitor dapagliflozin attenuates the activity of ROS-NLRP3 inflammasome axis in steatohepatitis with diabetes mellitus. Ann. Transl. Med. 7, 429 (2019).
Xu, L. et al. SGLT2 inhibition by empagliflozin promotes fat utilization and browning and attenuates inflammation and insulin resistance by polarizing M2 macrophages in diet-induced obese mice. eBioMedicine 20, 137–149 (2017).
Chun, H. J. et al. Increased expression of sodium-glucose cotransporter 2 and O-GlcNAcylation in hepatocytes drives non-alcoholic steatohepatitis. Metabolism 145, 155612 (2023).
Hawley, S. A. et al. The Na+/glucose cotransporter inhibitor canagliflozin activates AMPK by inhibiting mitochondrial function and increasing cellular AMP levels. Diabetes 65, 2784–2794 (2016).
Radlinger, B. et al. Empagliflozin protects mice against diet-induced obesity, insulin resistance and hepatic steatosis. Diabetologia 66, 754–767 (2023).
Tanaka, H. et al. Factors affecting canagliflozin-induced transient urine volume increase in patients with type 2 diabetes mellitus. Adv. Ther. 34, 436–451 (2017).
Peters, A. L. et al. Euglycemic diabetic ketoacidosis: a potential complication of treatment with sodium-glucose cotransporter 2 inhibition. Diabetes Care 38, 1687–1693 (2015).
Hayes, A. G., Raven, L. M., Viardot, A., Kotlyar, E. & Greenfield, J. R. SGLT2 inhibitor-induced ketoacidosis in a patient without diabetes. Diabetes Care 47, e4–e5 (2024).
Handelsman, Y. et al. American Association of Clinical Endocrinologists and American College of Endocrinology position statement on the association of Sglt-2 inhibitors and diabetic ketoacidosis. Endocr. Pract. 22, 753–762 (2016).
Joubert, M. et al. The sodium-glucose cotransporter 2 inhibitor dapagliflozin prevents cardiomyopathy in a diabetic lipodystrophic mouse model. Diabetes 66, 1030–1040 (2017).
Terami, N. et al. Long-term treatment with the sodium glucose cotransporter 2 inhibitor, dapagliflozin, ameliorates glucose homeostasis and diabetic nephropathy in db/db mice. PLoS ONE 9, e100777 (2014).
Hare, G. M. T. et al. Impact of sodium glucose linked cotransporter-2 inhibition on renal microvascular oxygen tension in a rodent model of diabetes mellitus. Physiol. Rep. 9, e14890 (2021).
Layton, A. T. & Vallon, V. SGLT2 inhibition in a kidney with reduced nephron number: modeling and analysis of solute transport and metabolism. Am. J. Physiol. Ren. Physiol. 314, F969–F984 (2018).
Verma, S. et al. Empagliflozin increases cardiac energy production in diabetes: novel translational insights into the heart failure benefits of SGLT2 inhibitors. JACC Basic. Transl. Sci. 3, 575–587 (2018).
Mazer, C. D. et al. Effect of empagliflozin on erythropoietin levels, iron stores, and red blood cell morphology in patients with type 2 diabetes mellitus and coronary artery disease. Circulation 141, 704–707 (2020).
Umino, H. et al. High basolateral glucose increases sodium-glucose cotransporter 2 and reduces sirtuin-1 in renal tubules through glucose transporter-2 detection. Sci. Rep. 8, 6791 (2018).
Li, J. et al. Renal protective effects of empagliflozin via inhibition of EMT and aberrant glycolysis in proximal tubules. JCI Insight 5, e129034 (2020).
Cai, T. et al. Sodium-glucose cotransporter 2 inhibition suppresses HIF-1α-mediated metabolic switch from lipid oxidation to glycolysis in kidney tubule cells of diabetic mice. Cell Death Dis. 11, 390 (2020).
Vallon, V. et al. Knockout of Na-glucose transporter SGLT2 attenuates hyperglycemia and glomerular hyperfiltration but not kidney growth or injury in diabetes mellitus. Am. J. Physiol. Ren. Physiol. 304, F156–F167 (2013).
Acknowledgements
The authors appreciate the Medical Illustration & Design (MID) team, a member of Medical Research Support Services of Yonsei University College of Medicine, Seoul, South Korea, for their excellent support with medical illustration and M. Sohn for her valuable assistance in the preparation of the tables.
Author information
Authors and Affiliations
Contributions
The authors contributed equally to all aspects of the article.
Corresponding authors
Ethics declarations
Competing interests
Y.L. has received research grants from Asen, Chong Kun Dang Pharmaceutical, Daewoong Pharmaceutical, Jeil Pharmaceutical and Yuhan Corporation; and clinical investigator fees from Eli Lilly, Hanmi Pharmaceutical and Novo Nordisk. S.L. has received research grants from LG Chem, Merck Sharp & Dohme and Novo Nordisk, and honoraria as a consultant or speaker from Abbott, AstraZeneca, Boehringer Ingelheim, Chong Kun Dang Pharmaceutical, Daewoong Pharmaceutical, LG Chem and Novo Nordisk. M.J.D. has acted as consultant, advisory board member and speaker for Boehringer Ingelheim, Lilly, Novo Nordisk and Sanofi; has been an advisory board member and speaker for AstraZeneca; has acted as an advisory board member for Janssen, Lexicon, Pfizer and ShouTi Pharma; has acted as a speaker for Napp Pharmaceuticals, Novartis and Takeda Pharmaceuticals International; and has received grants in support of investigator-initiated trials from AstraZeneca, Boehringer Ingelheim, Lilly, Janssen, Novo Nordisk and Sanofi-Aventis.
Peer review
Peer review information
Nature Reviews Endocrinology thanks Dimitrios Patoulias, who co-reviewed with Paschalis Karakasis; Markus Schlaich and the other, anonymous, reviewer(s) for their contribution to the peer review of this work.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Lee, Yh., Lim, S. & Davies, M.J. Cardiometabolic and renal benefits of sodium–glucose cotransporter 2 inhibitors. Nat Rev Endocrinol 21, 783–798 (2025). https://doi.org/10.1038/s41574-025-01170-4
Accepted:
Published:
Version of record:
Issue date:
DOI: https://doi.org/10.1038/s41574-025-01170-4
