
Abstract
Study design:
Retrospective chart review.
Objectives:
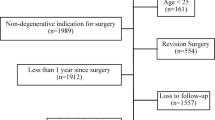
The objective of the current study was to evaluate the correlation between neurological deficits and the severity of narrowing of the spinal canal in patients with thoracic, thoracolumbar and lumbar burst-type fractures by comparing the classifications of Denis and Magerl. From 1989 to 2005, a total of 227 patients with burst fractures following Denis' criteria were studied.
Setting:
Tertiary teaching institution.
Methods:
Computed tomographic scans of the fractured spine were analyzed to assess the narrowing of the spinal canal. Following Magerl's criteria, patients were later subdivided into two groups according to the presence of associated ligament injuries, out of which 185 patients had no such injuries and the remaining 42 patients were classified as Megerl group B.
Results:
Results were evaluated based on the initial neurological status of patients according to Frankel and based on the midsagittal diameter of the fractured vertebra. A significant correlation was found between the narrowing of the spinal canal and neurological deficits in both classifications, with no significant differences between either.
Conclusion:
The percentage of narrowing of the spinal canal proved to be a pre-disposing factor for the severity of the neurological status in thoracolumbar and lumbar burst-type fractures according to the classifications of Denis and Magerl. The greater the bone fragment in the spinal canal, the greater will be the probability of neurological deficits in both fracture classifications, equally.
Similar content being viewed by others

Log in or create a free account to read this content
Gain free access to this article, as well as selected content from this journal and more on nature.com
or
References
Denis F . The three column spine and its significance in the classification of acute thoracolumbar spinal injuries. Spine (Philadelphia, PA, 1976) 1983; 8: 817–831.
Magerl F, Aebi M, Gertzbein SD, Harms J, Nazarian S . A comprehensive classification of thoracic and lumbar injuries. Eur Spine J 1994; 3: 184–201.
Fontijne WP, de Klerk LW, Braakman R, Stijnen T, Tanghe HL, Steenbeek R et al. CT scan prediction of neurological deficit in thoracolumbar burst fractures. J Bone Joint Surg Br 1992; 74: 683–685.
Frankel HL, Hancock DO, Hyslop G, Melzak J, Michaelis LS, Ungar GH et al. The value of postural reduction in the initial management of closed injuries of the spine with paraplegia and tetraplegia. I. Paraplegia 1969; 7: 179–192.
Trafton PG, Boyd Jr CA . Computed tomography of thoracic and lumbar spine injuries. J Trauma 1984; 24: 506–515.
Neumann P, Wang Y, Kärrholm J, Malchau H, Nordwall A . Determination of inter-spinous process distance in the lumbar spine. Evaluation of reference population to facilitate detection of severe trauma. Eur Spine J 1999; 8: 272–278.
Hounsfield GN . Computerized transverse axial scanning (tomography). 1. Description of system. Br J Radiol 1973; 46: 1016–1022.
Meves R, Avanzi O . Correlation between neurological deficit and spinal canal compromise in 198 patients with thoracolumbar and lumbar fractures. Spine (Philadelphia, PA, 1976) 2005; 30: 787–791.
Vaccaro AR, Baron EM, Sanfilippo J, Jacoby S, Steuve J, Grossman E et al. Reliability of a novel classification system for thoracolumbar injuries: the Thoracolumbar Injury Severity Score. Spine (Philadelphia, PA, 1976) 2006; 31 (Suppl): S62–S69; discussion S104.
Kim NH, Lee HM, Chun IM . Neurologic injury and recovery in patients with burst fracture of the thoracolumbar spine. Spine (Philadelphia, PA, 1976) 1999; 24: 290–293; discussion 294.
Leibl T, Funke M, Dresing K, Grabbe E . Instabität von Wirbelsäulenfrakturen--Thepapeutische Relevanz unterschiedlicher Klassifikationen [Instability of spinal fractures--therapeutic relevance of different classifications]. Rofo 1999; 170: 174–180.
Oner FC, Ramos LM, Simmermacher RK, Kingma PT, Diekerhof CH, Dhert WJ et al. Classification of thoracic and lumbar spine fractures: problems of reproducibility. A study of 53 patients using CT and MRI. Eur Spine J 2002; 11: 235–245.
Saifuddin A, Noordeen H, Taylor BA, Bayley I . The role of imaging in the diagnosis and management of thoracolumbar burst fractures: current concepts and a review of the literature. Skeletal Radiol 1996; 25: 603–613.
Oner FC, van Gils AP, Dhert WJ, Verbout AJ . MRI findings of thoracolumbar spine fractures: a categorisation based on MRI examinations of 100 fractures. Skeletal Radiol 1999; 28: 433–443.
Eberl R, Kaminski A, Müller EJ, Muhr G . Die Bedeutung des Wirbelkanaldurchmessers im thorakolumbalen und lumbalen Bereich nach Trauma. Korreliert. Orthopade 2003; 32: 859–864.
Sar C, Bilen FE . Thoracolumbar flexion-distraction injuries combined with vertebral body fractures. Am J Orthop (Belle Mead NJ) 2002; 31: 147–151.
Sasso RC, Renkens K, Hanson D, Reilly T, McGuire Jr RA, Best NM . Unstable thoracolumbar burst fractures: anterior-only versus short-segment posterior fixation. J Spinal Disord Tech 2006; 19: 242–248.
Petersilge CA, Pathria MN, Emery SE, Masaryk TJ . Thoracolumbar burst fractures: evaluating with MRI imaging. Radiology 1995; 194: 49–54.
Petersilge CA, Emery SE . Thoracolumbar burst fracture: evaluating stability. Semin Ultrasound CT MR 1996; 17: 105–113.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article
Cite this article
Caffaro, M., Avanzi, O. Is there a difference between narrowing of the spinal canal and neurological deficits comparing Denis and Magerl classifications?. Spinal Cord 49, 297–301 (2011). https://doi.org/10.1038/sc.2010.112
Received:
Revised:
Accepted:
Published:
Issue date:
DOI: https://doi.org/10.1038/sc.2010.112
