
Key Points
-
Provides information on the safety of oral sedation in clinical paediatric dentistry.
-
Provides information on the efficacy of oral sedation when providing care to children.
-
Demonstrates the broad range of procedures in young children who would otherwise have had general anaesthesia.
Abstract
Introduction Conscious sedation for young children is a rapidly developing area of clinical activity. Many studies have shown positive results using oral midazolam on children. These case series investigated oral midazolam conscious sedation as an alternative to general anaesthesia in a clinical service setting.
Objective The purpose of this work was to determine the safety and efficacy of oral midazolam for conscious sedation in children undergoing dental treatment.
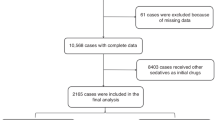
Methods Patients were selected by colleagues for treatment under oral sedation. The main general criteria were weight below 36 kilos and ASA I, II, or III. Midazolam 0.5 mg/kg was administered orally. A pulse oximeter was applied to a finger to monitor vital signs and the Houpt scale was used to assess behaviour.
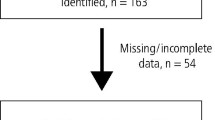
Results A total of 510 children aged between 13 months and 11 years were included. The behaviour of 379 (74%) was excellent or very good. The pulse rate and peripheral oxygenation were within the normal range for all patients. The main adverse effects were diplopia and post-sedation dysphoria.
Conclusions Oral midazolam is a safe and effective method of sedation although some children were agitated and distressed either during or after treatment. Parents need to be warned about this.
Similar content being viewed by others
Log in or create a free account to read this content
Gain free access to this article, as well as selected content from this journal and more on nature.com
or
References
Hosey M T . Managing anxious children: the use of conscious sedation in paediatric dentistry. Int J Paediatr Dent 2009; 12: 359–372.
Holroyd I, Roberts G J . Inhalation sedation with nitrous oxide: a review. Dent Update 2000; 27: 141–146.
Yagiela J A . Health hazards and nitrous oxide: a time for reappraisal. Anesth Prog 1991; 38: 1–11.
Gallardo F, Cornejo G, Borie R . Oral midazolam as premedication for the apprehensive child before dental treatment. J Clin Pediatr Dent 1994; 18: 123–127.
Haas D A, Nenniger S A, Yacobi R, Magathan J G, Grad H, Copp P E . A pilot study of the efficacy of oral midazolam for sedation in pediatric dental patients. Anesth Prog 1996; 43: 1–8.
Lima A R A, Costa L R R S, Costa P S S . A randomized controlled crossover trial of oral midazolam and hydroxyzine for pediatric dental sedation. Pesqui Odontol Bras 2003; 17: 206–211.
Downs T, Dembo J, Lyons T D, Pelphery A . A comparative study of midazolam to meperidine/promethazine as an IM sedative technique for the pediatric dental patient. ASDC J Dent Child 1997; 64: 197–200.
Hartgraves P M, Primosch R . An evaluation of oral and nasal midazolam for pediatric dental sedation. ASDC J Dent Child 1994; 61: 175–181.
Marshall W R, Weaver B D, McCutcheon P . A study of the effectiveness of oral midazolam as a dental pre-operative sedative and hypnotic. Spec Care Dentist 1999; 19: 259–266.
Musial K M, Wilson S, Preisch J, Weaver J . Comparison of the efficacy of oral midazolam alone versus midazolam and meperidine in the pediatric dental patient. Pediatr Dent 2003; 25: 468–474.
Roelofse J A, Joubert J J, Roelofse P G . A double-blind randomized comparison of midazolam alone and midazolam combined with ketamine for sedation of pediatric dental patients. J Oral Maxillofac Surg 1996; 54: 838–844.
Shapira J, Kupietzky A, Kadari A, Fuks A B, Holan G . Comparison of oral midazolam with and without hydroxyzine in the sedation of pediatric dental patients. Pediatr Dent 2004; 26: 492–496.
Singh N, Pandey R K, Paksena A K, Aiswal J N . A comparative evaluation of oral midazolam with other sedatives as premedication in pediatric dentistry. J Clin Pediatr Dent 2002; 26: 161–164.
Wilson K E, Welbury R R, Girdler N M . A randomised, controlled, crossover trial of oral midazolam and nitrous oxide for paediatric dental sedation. Anaesthesia 2002; 57: 860–867.
Wilson K E, Girdler N M, Welbury R R . A comparison of oral midazolam and nitrous oxide sedation for dental extractions in children. Anaesthesia 2006; 61: 1144.
Aydintug Y S, Okcu K M, Guner Y, Gunaydin Y, Sencimen M . Evaluation of oral or rectal midazolam as conscious sedation for pediatric patients in oral surgery. Mil Med 2004; 169: 270–273.
Lee-Kim S J, Fadavi S, Punwani I, Koerber A . Nasal versus oral midazolam sedation for pediatric dental patients. J Dent Child (Chic) 2004; 71: 126–130.
Craig D, Skelly M . Practical conscious sedation. pp 86. London: Quintessence Publishing, 2004.
Avery B S, Hulf J . Standards for conscious sedation in dentistry: alternative techniques. pp 1–31. London: Royal College of Anaesthetists and the Royal College of Surgeons of England, 2007.
ASA. ASA classification. New classification of physical status. Anaesthesiology 1963; 24: 111.
Payne J P, Severinghaus J W . Pulse oximetry. Berlin: Springer-Verlag, 1986.
Houpt M I, Kupietzky A, Tofsky N, Koenigsberg S . Effects of nitrous oxide on diazepam sedation of young children. Pediatr Dent 1996; 18: 236–241.
Department of Health. A conscious decision. A review of the use of conscious sedation and general anaesthesia in primary dental care. London: Department of Health, 2000.
Matharu L L, Ashley P F . What is the evidence for paediatric dental sedation? J Dent 2007; 35: 2–20.
Yasny J S, Asgari A . Consideration for the use of enteral sedation in pediatric dentistry. J Clin Pediatr Dent 2008; 32: 85–93.
Acknowledgements
The authors would like to thank Victoria Lucas for her assistance with the text.
Author information
Authors and Affiliations
Additional information
Refereed paper
Rights and permissions
About this article
Cite this article
Lourenço-Matharu, L., Roberts, G. Oral sedation for dental treatment in young children in a hospital setting. Br Dent J 209, E12 (2010). https://doi.org/10.1038/sj.bdj.2010.886
Accepted:
Published:
Issue date:
DOI: https://doi.org/10.1038/sj.bdj.2010.886
