
Abstract
There is a lack of knowledge about the effect of flavanols-rich dark chocolate intake on the anatomy and functionality of retinal vessels. The aim of this study prospective, randomized, blind, crossover clinical trial (ClinicalTrials.gov Identifier: NCT05227248, 07/02/2022) was to evaluate the effect of dark-chocolate intake on the functionality and anatomy of the retinal vessels in healthy subjects using dynamic vessel analyzer (DVA) and optical coherence tomography angiography (OCT-A). Twenty eyes of 20 healthy subjects (mean age, 24.4 ± 1.6 years; 12 females) were enrolled. Participants were randomized to consume 20 g of dark chocolate or 7.5 g of milk chocolate. Visual function, DVA and OCT-A parameters were evaluated before chocolate consumption and two hours later. One week later, the same participants were tested before and after consuming the opposite chocolate. Using OCT-A, no differences were disclosed in terms of perfusion density changes after dark-chocolate and milk-chocolate intake analyzing all chorioretinal plexuses (p > 0.09 in all analyses). Using DVA, a significant increase in the arterial dilation percentage after flicker stimulation was disclosed comparing baseline (2.750 ± 2.054%) with values after the dark chocolate intake (4.145 ± 3.055%, p = 0.016). This difference was not disclosed after the milk chocolate intake (p = 0.465). We disclosed that a reasonable amount of flavanols-rich chocolate in healthy subjects has benefic functional short-term effects in retinal vessels measured with DVA. This suggests a potential role of dark chocolate intake on retinal vessels. Further studies with long-term follow-up are warranted to show if the chronic assumption of dark chocolate could play a favorable role in the prevention of retinal diseases.
Similar content being viewed by others

Introduction
Cocoa and dark chocolate possess polyphenols as major constituents whose dietary consumption has been associated with beneficial effects1,2,3. Cocoa polyphenols exert antioxidant effects and anti-inflammatory activities on various signaling pathways inducing the release of nitric oxide (NO) and resulting in vasodilation and cardioprotective effects1,4,5,6,7. Indeed, polyphenols reduce blood pressure and improve blood flow to the brain in healthy subjects1. Furthermore, NO release causes arterial vasodilation in healthy subjects, and it exerts anti-inflammatory activity in situ by decreasing leukocyte recruitment and platelet aggregation7,8.
Studies published so far on the effects of chocolate on vision have led to different results. Briefly, Rabin et al.9 reported that the consumption of flavanol-rich chocolate significantly improves visual contrast sensitivity. On the other hand, Siedlecki et al.10 disclosed no effects on visual function after chocolate intake. The introduction of new imaging and functional methods, especially optical coherence tomography angiography (OCT-A) and dynamic vessel analyzer (DVA), has made it possible to highlight and clarify various aspects related to ocular pathophysiology and ocular diseases11,12,13,14. For this reason, the use of these new methods could clarify what the effects of chocolate are on the retinal vessels9,10,15,16. Siedlecki et al.10 reported no short-term effects of flavanol-rich dark chocolate consumption by analyzing the perfusion density (PD) of retinal vessels on OCT-A. However, no previous studies reported the effect of chocolate consumption using an anatomic-functional test as DVA. Indeed, DVA studies in a non-invasive way the endothelial function using the principle of neurovascular coupling17,18.
The main objective of this clinical trial is to evaluate the effect of dark chocolate administration on the functionality and anatomy of the retinal vessels in healthy subjects, by comparison with that given by the ingestion of milk chocolate and to baseline.
Methods
This is a prospective, randomized, blind, crossover clinical trial enrolling healthy subjects from April 2021 to July 2021 at the Medical Retina & Imaging Unit of the Department of Ophthalmology, University Vita-Salute, San Raffaele Hospital in Milan (Italy). The study was conducted in agreement with the Declaration of Helsinki for research involving human subjects and it was approved by the San Raffaele Ethics Committee on 05/02/2020 (number 4/INT/2020). The trial was registered on ClinicalTrials.gov (ID NCT05227248, registered on 07/02/2022). All included patients signed a written informed consent to participate in this study.
Inclusion criteria for the study group were: (1) age 18 or over; (2) healthy volunteers who can understand and sign informed consent.
Exclusion criteria included: (1) inability to follow planned procedures; (2) opacity of the dioptric influencing the execution of the examinations; (3) ocular pathologies and systemic hypertension; (4) myopia greater than − 8.0 diopters (D), hyperopia greater than 5.0D, and/or astigmatism greater than 3.0D.
Study protocol
Healthy subjects underwent a complete ophthalmologic evaluation at baseline, including the assessment of distance best-corrected visual acuity (BCVA) and multimodal imaging evaluation. In detail, the healthy subjects were evaluated using structural spectral-domain optical coherence tomography (SD-OCT, Spectralis, Heidelberg Engineering, Heidelberg, Germany), OCT-A (PlexElite 9000, Carl Zeiss Meditec, Inc., Dublin, USA), evaluation of retinal vascular functionality by DVA (Imedos, Jena, Germany), and evaluation of retinal vessel diameter using Retinal Vessel Analyzer (RVA, Imedos GmbH, Jena, Germany). The same subjects repeated the full ophthalmologic evaluation two hours after consuming dark chocolate or milk chocolate.
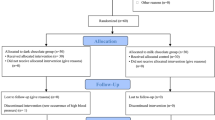
All subjects were randomized into two different groups flipping a coin by a senior investigator (RS): the first group started with dark chocolate administration (20 g containing 400 mg of flavanols and more than 90% of pure coca) and after a week repeated all the examinations after milk chocolate intake (7.5 g containing approximately 30% of pure cocoa), whereas the second group started with the administration of milk chocolate and after a week repeated all the examination after dark chocolate (Fig. 1). The choice of the quantity of both chocolate administrations was based on a previous published paper9. In order to maintain the blind design, the main examinator did not know which kind of chocolate was administrated. Also, the patient was not informed on the kind of chocolate that was administrated, even if the subjects could identify the type of chocolate by taste.

Flowchart reporting the design and the flow of participant in the study.
Participants were instructed to avoid smoking activity, and intake of caffeine, alcohol, and milk products 24 h prior to examinations. Furthermore, in order to avoid possible confounding effects due to blood pressure changes, all subjects were instructed to rest on the examination chair for 10 min prior to the examination. Finally, all patients were tested between 9 and 11 a.m. and all examinations were performed by a single-trained grader (M.P.).
The primary outcomes of the study were changes in retinal perfusion using OCT-A and changes in retinal vascular response to flicker stimulation using DVA after dark chocolate intake.
Structural SD-OCT measurements
Central macular thickness (CMT) was recorded with the Spectralis software (Heidelberg Eye Explorer, version 1.9.11.0 Heidelberg Engineering, Germany) in the central 1-mm-diameter circle of the ETDRS thickness map. Subfoveal choroidal thickness (ChT) was assessed by measuring the distance between Bruch’s membrane interface and sclerochoroidal interface. Mean ChT was assessed as the mean between subfoveal ChT, ChT measured 1000 μm nasally and temporally to the fovea19. All measurements were performed by two trained graders (M.P. and A.S.) and mean measurement was considered for the statistical analysis.
OCT-A image acquisition and analysis
In all subjects, a scanning area of 6 × 6 mm was adopted, centered on the foveal area. En-face flow images of superficial capillary plexus (SCP), deep vascular complex (DVC) including both intermediate and deep capillary plexuses20, and choriocapillaris (CC) were obtained and imported into ImageJ 1.50 software (National Institutes of Health, Bethesda, Maryland, USA).20 Foveal avascular zone (FAZ) area was manually outlined using the polygon selection tool in the whole retinal plexus, and its dimension was expressed as square millimeters (mm2). The area was outlined by two trained graders (R.S. and A.S.), and the mean area measurement was considered for the statistical analysis. Perfusion density of SCP, DVC, and CC was calculated as previously reported12,21. In detail, SCP and DVC images were binarized through the Mean’s thresholding and PD was calculated as the ratio of white pixels (i.e. vessels) and the total pixels after FAZ exclusion. Choriocapillaris images were binarized through Phansalkar’s thresholding (radius, 15 pixels) and PD was calculated as the ratio of white pixels (i.e. vessels) and the total pixels after exclusion of the CC directly beneath major superficial retinal vessels in order to eliminate potentially confounding shadow or projection artifacts.
Dynamic vessel analysis
Dynamic Vessel Analyzer is a tool that dynamically assesses the degree of arterial and venous dilation upon stimulation with flicker light. All subjects were requested to remain focused on a tip bar along the examination while the fundus was enlightened with a green light (average luminance 130 cd/m2). In order to perform the dynamic analysis, a superior or inferior temporal venous and arterial segment located between one-half and two-disc diameters from the optic disc margin was chosen. During the examination (350 s) 3 cycles of flicker/non-flicker light were registered. The DVA creates a flicker with an optoelectronic shutter that interrupts the light source with a bright-to-dark ratio of 25:1 at a frequency of 12.5 Hz, to maximize vasodilation and blood flow during flicker22,23,24. Vessel diameters were expressed in measurement units (MU); vessel dilation was measured by calculating the percentage increase in vessel diameter relative to baseline after 20 s of flicker stimulation and averaging the 3 measurement cycles.
Static vessel analysis
Using the FF450 retinal camera, included in the DVA system, a 50-degree fundus photograph was acquired in each subject. VISUALIS and VesselMap Software allowed the analysis of these photographs using the brightness profile of the vessel25. In all subjects, we calculated the central retinal artery equivalent (CRAE), which relates to the diameter of the central retinal artery and the central retinal vein equivalent (CRVE), which relates to the diameter of the central retinal vein.
Statistical analysis
A sample size of 17 eyes has a greater than 80% power to identify a variation of 5% in PD of retinal plexuses between pre and post chocolate intake, with an estimated standard deviation of the change outcome of 1.5% and an alpha error of 0.0526. Allowing an additional 20% of the estimated sample size in order to counter possible withdrawn patients, we estimated that 20 eyes would be required.
Statistical analysis was performed using SPSS statistics software version 28.0.1.0 (SPSS Inc., cIBM, Chicago, IL, USA). Descriptive analyses were reported as counts and percentages for categorical variables, and as means ± standard deviation for quantitative variables. The intraclass correlation coefficient (ICC; 95% CI) was used to estimate the agreement between individual measurements from both readers. Continuous variables were tested for normal distributions, according to the Kolmogorov–Smirnov test. Comparisons of arterial diameter, arterial dilation, arterial constriction, venous diameter, venous dilation, CRAE, CRVE, FAZ, PD of SCP, PD of DVC, and PD of CC between different timepoints (before and after dark chocolate and milk chocolate intakes) were performed using repeated measures analysis of variance (ANOVA) with LSD post hoc analysis. Correlations between OCT-A parameters with age and refractive error were investigated using the Pearson correlation coefficient. In all analyses, p-values < 0.05 were considered as statistically significant.
Results
Demographics and main clinical findings
Twenty eyes of twenty healthy subjects with no prior ophthalmologic or medical history were included in this study. Twelve subjects (60%) were females, and 8 subjects (40%) were males. All patients were Caucasian and the mean age was 24.4 ± 1.6 years old (median 24, range 23–29). BCVA was 20/20 Snellen equivalent (0.0 ± 0.0 LogMAR) in all patients, and the mean refractive error was − 1.8 ± 2.1D (median − 0.75, range − 5.00 to + 0.50). All the demographics of the study population were reported in Table 1.
Dynamic vessel analysis
A dynamic vessel analysis was performed in order to evaluate the response of retinal vessels to flickering light. Importantly, the diameter of the artery and of the vein selected for the analyses was not different between the different DVA examinations (p = 0.210 and p = 0.415 for the arterial diameter and venous diameter analysis, respectively) (Table 2). This is of paramount importance, reflecting that the same kind of vessels was selected for the different examinations with reliable analysis.
Analyzing the response of the retinal vessels to the flicker light, we disclosed a significant increase in the arterial dilation percentage after the dark chocolate intake in comparison to the baseline (mean arterial dilation of 2.750 ± 2.054% at the baseline vs 4.145 ± 3.055% after the dark chocolate intake, p = 0.016) (Fig. 2A,B). This difference was not disclosed after the milk chocolate intake (p = 0.465) (Table 2) (Fig. 2C,D). On the other hand, the arterial constriction after the dilation due to the flicker light showed no changes after both dark chocolate and milk chocolate intake (p = 0.934 and p = 0.575, respectively).

DVA analysis of a representative case. DVA analysis showing the arterial dilation and constriction after flicker stimulation before and after dark chocolate intake (A,B) and before and after milk chocolate intake (C,D). Of note, arterial dilation was greater after dark chocolate intake (B) in comparison to the pre-intake examination.
Analyzing the venous dilation percentage, there was an increasing trend after the dark chocolate intake (mean venous dilation of 3.265 ± 3.159% at the baseline vs 4.465 ± 2.969% after the dark chocolate intake, p = 0.086), and lower changes after the milk chocolate intake (p = 0.124) (Table 2).
Static vessel analysis
By means of RVA, the static analysis disclosed no significant difference in mean CRAE and mean CRVE before and after the dark chocolate and milk chocolate intake. Since CRAE and CRVE are related to the diameter of the central retinal artery and vein, respectively, we did not disclose any significant change in the mean diameter of major retinal vessels after both chocolate intakes. All data are reported in Table 2.
OCT-angiography analysis
Regarding the analysis of retinal plexuses using OCT-A, no significant change was found in FAZ area by comparing examinations before and after dark chocolate intake (p = 0.095) and milk chocolate intake (p = 0.502). Interobserver variability between readers was excellent for FAZ measurements (ICC = 0.991 [0.978–0.996]). Perfusion density among SCP, DVC, and CC did not show any significant change before and after dark chocolate and milk-chocolate intakes (Table 3). Of note, the only trend that was disclosed in this analysis, was a greater PD of the SCP after the dark chocolate intake, although this difference was not statistically significant (p = 0.090).
The signal strength index (SSI) of examinations did not show any significant difference among the different examinations (p > 0.2 in all analyses). Sex, patient age, and refractive error did not influence significantly the FAZ area, and PD of the whole analyzed plexuses (p > 0.1 in all analyses).
Discussion
In this study, using a multimodal imaging evaluation including DVA and OCT-A, we analyzed the functional and structural changes induced by dark chocolate intake in comparison to milk chocolate intake. We disclosed a significantly greater dilation response of arterial vessels to flicker stimulus after dark chocolate intake, suggesting a beneficial effect of dark chocolate on retinal circulation.
Our hypothesis is that the greater dilation response of arterial vessels after dark chocolate intake is due to the chocolate flavonoids. Flavonoids, one of the major constituents of dark chocolate, have long been known to have beneficial effects on the cardiovascular system1. The potential health benefits of flavanol span a wide range of organs and indications: in cardiovascular disease, for example, flavanols have been reported to lower systemic blood pressure, optimize coronary perfusion, and limit thrombocyte aggregation1. Cocoa flavonoids, in fact, cause the NO release by activation of endothelial NO synthase, resulting in vasodilation and cardioprotective benefits27. NO can activate soluble guanylate cyclase in smooth muscle cells and platelets, resulting in an increase in cyclic guanosine monophosphate (cGMP). Smooth muscle cell relaxation and platelet aggregation inhibition result from the subsequent blockage of calcium flow and decrease in cytosolic calcium concentration28. Furthermore, cGMP can raise cyclic adenosine monophosphate (cAMP), which activates prostacyclin28. Interestingly, prostacyclin serves as a vasodilator in conjunction with NO, helping to protect against thrombosis. Furthermore, prostacyclin's ability to lower plasma leukotrienes enhances its anti-inflammatory and vasoprotective characteristics29. The potential of cocoa flavonoids to improve cerebral blood flow in healthy young people, as measured by functional magnetic resonance imaging (FMRI), is an important neurotrophic impact of cocoa flavonoids30. Increased blood flow in the middle cerebral artery has been linked to protective benefits in the treatment of dementia and stroke31.
Differently from other specialists, the ophthalmologist has the opportunity to directly visualize and analyze arterial and venous vessels. This is the reason why we decided to take advantage of this possibility and we used a multimodal analysis to evaluate the effect linked to the administration of dark chocolate on the functionality and anatomy of the retinal vessels in healthy subjects. Concerning visual function, Rabin et al.9 in 2018, have reported that consuming flavanol-rich chocolate significantly improves visual contrast sensitivity owing to supposedly improved oxygenation of the retina. Subsequently, Siedlecki et al.10 further investigated the correlation of subjective flavanol effects on visual function and on the retinal perfusion measured with OCT-A. Including 20 healthy patients, the authors found no relevant changes in retinal perfusion after consumption of dark or milk chocolate. Most recently, a study conducted by Scuderi et al.32 confirmed previously reported data, showing no significant changes of retinal and CC perfusion using OCT-A after intake of dark or white chocolate32.
Our analysis confirmed the results of previously cited studies because we disclosed no significant difference in the PD of SCP, DVC, and CC after dark chocolate or milk chocolate intake. We found a slightly positive trend of greater perfusion in the SCP after the ingestion of dark chocolate compared to the baseline (PD of 41.9 ± 2.5% vs 43.2 ± 2.7%, p = 0.090) that was not disclosed after milk chocolate intake. Nevertheless, based on previous studies, the sample size of our study was calculated based on a variation of 5% in the PD of retinal plexuses. The difference in PD after dark chocolate intake was lower than 5% and, for this reason, we did not consider it clinically significant.
The novelty of our study was the application for the first time of DVA and RVA. While OCT-A studies mainly anatomical changes of retinal vessels, DVA studies retinal vessels from a functional point of view, allowing the identification of endothelial function18. The mechanisms involved in the retinal vasodilation due to flicker are, however, not yet fully understood. It was suggested that the main mechanism related to flicker-related vasodilation is mediated by the endogenous NO18,33,34. Several factors influenced the flicker-related vasodilation, such as preeclampsia35, cardiovascular disease36, hypercholesterolaemia37, obesity38, diabetes36, and systemic hypertension39. Using DVA, we found a significantly greater dilation response of arterial vessels to flicker stimulus after the intake of dark chocolate, compared to the dilation response at baseline (arterial dilation after flicker of 2.750 ± 2.054 vs 4.145 ± 3.055 before and after the dark chocolate intake, respectively, p = 0.016). The greater dilation response has been partially evident also for the venous vessels, although no significance was found (p = 0.086). This difference in the dilation response between the artery and the vein could be due to the different anatomical composition of the two vessels, allowing retinal arteries more responsive to the NO vasodilation effect. Indeed, thanks to the presence of smooth muscle cells, arterial vessels respond more in terms of dilation after NO release in comparison to venous vessels and capillaries (explaining the no differences disclosed by OCT-A). The flavonoids contained in high quantities inside the administered dark chocolate should be able to trigger endothelial NO synthase to produce more NO. NO is known to play a key role in arterial smooth muscle vasodilation and this could explain the results we found40. Supporting the positive role of flavonoids, we also found that the arterial vessel dilation at the flicker analysis has no significance in the same subjects after the ingestion of milk chocolate. This is explained by the low dose of flavonoids in milk chocolate (approximately 30% of pure cocoa) in comparison to dark chocolate (approximately 90% of pure cocoa).
Limitations of the present study should be kept in mind. First of all, the relatively small sample size. Another important issue in the design of prospective studies on this topic is that the subject can easily recognize using taste what is the type of chocolate she/he is ingesting. For this reason, the double-blind study is difficult to carry. However, being our study based on morphological analyses, this should not have a great impact on the analysis. Furthermore, since visual function evaluations after chocolate intake were not conducted, the clinical significance of the observed retinal artery dilation due to dark chocolate intake remains unclear.
As a strength, our study is the first that integrated DVA, RVA, and OCT-A and investigated changes in vessel morphology and functionality as objective parameters for the evaluation of possible flavanol effects. The results of our study show a greater dilation response, especially of the arteries following the intake of dark chocolate. Of course, this is not enough to state that the benefits in vessel dilation inside by dark chocolate intake has effects on retinal diseases. Further longitudinal studies with a chronic assumption of dark chocolate should be carried out in order to evaluate the potential beneficial role of dark chocolate in terms of prevention of pandemic retinal diseases (i.e. age-related macular degeneration, diabetic retinopathy, and others) and/or in terms of slowing the progression of cited retinal diseases. Indeed, due to the study's focus on healthy young participants, there is a possibility that there is no impact on patients with retinal diseases.
We hypothesized that the effects of dark chocolate intake on arterial vessels were due the effects of the flavonoids; however, this correlation need further studied in order to be proven.
Furthermore, the study did not investigate the amount of flavanols that the subjects regularly consume in their daily lives. We cannot exclude that healthy participants already had a high baseline level of flavanols, thus additional benefits from supplementation may not be apparent.
In conclusion, we disclosed that a reasonable amount of cocoa in healthy subjects has benefic functional short-term effects in retinal vessels. This could suggest a potential role of dark chocolate intake in the prevention of retinal diseases. However, our results need a cautious interpretation due to targeting healthy young individuals and lack of confirmation of long-term effects. Further studies are warranted to better understand if the chronic assumption of dark chocolate could play a favorable role in the clinical course of retinal diseases.
Data availability
The data used to support the findings of this study are available from the corresponding author upon request.
References
Fisher, N. D., Hughes, M., Gerhard-Herman, M. & Hollenbergh, N. K. Flavanol-rich cocoa induces nitric-oxide-dependent vasodilation in healthy humans. J. Hypertens. 21, 2281–2286 (2003).
Ried, K., Fakler, P., & Stocks, N.P. Effect of cocoa on blood pressure. Cochrane Database Syst Rev. 4, CD008893 (2017).
Flammer, A. J. et al. Dark chocolate improves coronary vasomotion and reduces platelet reactivity. Circulation. 116, 2376–2382 (2007).
Mao, T. K. et al. The effect of cocoa procyanidins on the transcription and secretion of interleukin 1 beta in peripheral blood mononuclear cells. Life Sci. 66, 1377–1386 (2000).
Vogel, R. A. Measurement of endothelial function by brachial artery flow-mediated vasodilation. Am. J. Cardiol. 88, 31E-34E (2001).
Yeboah, J. et al. Predictive value of brachial flow-mediated dilation for incident cardiovascular events in a population-based study: The multi-ethnic study of atherosclerosis. Circulation. 120, 502–509 (2009).
Selmi, C., Cocchi, C. A., Lanfredini, M., Keen, C. L. & Gershwin, M. E. Chocolate at heart: The anti-inflammatory impact of cocoa flavanols. Mol. Nutr. Food Res. 52, 1340–1348 (2008).
Magrone, T., Candore, G., Caruso, C., Jirillo, E. & Covelli, V. Polyphenols from red wine modulate immune responsiveness: Biological and clinical significance. Curr. Pharm. Des. 14, 2733–2748 (2008).
Rabin, J. C., Karunathilake, N. & Patrizi, K. Effects of milk vs dark chocolate consumption on visual acuity and contrast sensitivity within 2 hours: A randomized clinical trial. JAMA Ophthalmol. 136, 678–681 (2018).
Siedlecki, J. et al. Effects of flavanol-rich dark chocolate on visual function and retinal perfusion measured with optical coherence tomography angiography: A randomized clinical trial. JAMA Ophthalmol. 137, 1373–1379 (2019).
Corbelli, E., Sacconi, R., Rabiolo, A., et al. Optical coherence tomography angiography in the evaluation of geographic atrophy area extension [published correction appears in Invest Ophthalmol Vis Sci. 2018 Apr 1;59(5):1801]. Invest. Ophthalmol. Vis. Sci. 58, 5201–5208 (2017).
Sacconi, R. et al. Choriocapillaris flow impairment could predict the enlargement of geographic atrophy lesion. Br. J. Ophthalmol. 105, 97–102 (2021).
Sacconi, R. et al. Nonexudative perifoveal vascular anomalous complex: The subclinical stage of perifoveal exudative vascular anomalous complex?. Am. J. Ophthalmol. 218, 59–67 (2020).
Sacconi, R. et al. Towards a better understanding of non-exudative choroidal and macular neovascularization. Prog. Retin. Eye Res. 92, 101113 (2023).
Field, D. T., Williams, C. M. & Butler, L. T. Consumption of cocoa flavanols results in an acute improvement in visual and cognitive functions. Physiol. Behav. 103, 255–260 (2011).
Bernstein, P. S. Does dark chocolate enhance visual function?. JAMA Ophthalmol. 137, 1380 (2019).
Sacconi, R. et al. Multimodal imaging assessment of vascular and neurodegenerative retinal alterations in type 1 diabetic patients without fundoscopic signs of diabetic retinopathy. J. Clin. Med. 8, 1409 (2019).
Newman, E. A. Functional hyperemia and mechanisms of neurovascular coupling in the retinal vasculature. J. Cereb. Blood Flow Metab. 33, 1685–1695 (2013).
Sacconi, R. et al. SD-OCT choroidal thickness in advanced primary open-angle glaucoma. J. Glaucoma. 26, 523–527 (2017).
Sacconi, R. et al. Morphofunctional analysis of the retina in patients with type 1 diabetes without complications after 30 years of disease. Sci. Rep. 10, 206 (2020).
Sacconi, R. et al. Optical coherence tomography angiography in pseudophakic cystoid macular oedema compared to diabetic macular oedema: Qualitative and quantitative evaluation of retinal vasculature. Br. J. Ophthalmol. 102, 1684–1690 (2018).
Polak, K., Schmetterer, L. & Riva, C. E. Influence of flicker frequency on flicker-induced changes of retinal vessel diameter. Invest. Ophthalmol. Vis. Sci. 43, 2721–2726 (2002).
Riva, C. E., Falsini, B. & Logean, E. Flicker-evoked responses of human optic nerve head blood flow: Luminance versus chromatic modulation. Invest. Ophthalmol. Vis. Sci. 42, 756–762 (2001).
Falsini, B., Riva, C. E. & Logean, E. Flicker-evoked changes in human optic nerve blood flow: Relationship with retinal neural activity. Invest. Ophthalmol. Vis. Sci. 43, 2309–2316 (2002).
Garhofer, G. et al. Use of the retinal vessel analyzer in ocular blood flow research. Acta Ophthalmol. 88, 717–722 (2010).
Carnevali, A. et al. Optical coherence tomography angiography analysis of retinal vascular plexuses and choriocapillaris in patients with type 1 diabetes without diabetic retinopathy. Acta Diabetol. 54, 695–702 (2017).
Moreno-Ulloa, A., Romero-Perez, D., Villarreal, F., Ceballos, G. & Ramirez-Sanchez, I. Cell membrane mediated (-)-epicatechin effects on upstream endothelial cell signaling: Evidence for a surface receptor. Bioorg. Med. Chem. Lett. 24, 2749–2752 (2014).
Moncada, S. & Higgs, A. The l-arginine-nitric oxide pathway. N. Engl. J. Med. 329, 2002–2012 (1993).
Schwab, U. S. et al. Different effects of palmitic and stearic acid-enriched diets on serum lipids and lipoproteins and plasma cholesteryl ester transfer protein activity in healthy young women. Metabolism. 45, 143–149 (1996).
Francis, S. T., Head, K., Morris, P. G. & Macdonald, I. A. The effect of flavanol-rich cocoa on the fMRI response to a cognitive task in healthy young people. J. Cardiovasc. Pharmacol. 47, S215-220 (2006).
Sorond, F. A., Lipsitz, L. A., Hollenberg, N. K. & Fisher, N. D. Cerebral blood flow response to flavanol-rich cocoa in healthy elderly humans. Neuropsychiatr. Dis. Treat. 4, 433–440 (2008).
Scuderi, G. et al. Short-term effects of dark chocolate on retinal and choriocapillaris perfusion in young, healthy subjects using optical coherence tomography angiography. Nutrients. 12, 664 (2020).
Dorner, G. T. et al. Nitric oxide regulates retinal vascular tone in humans. Am. J. Physiol. Heart Circ. Physiol. 285, H631–H636 (2003).
Kur, J., Newman, E. A. & Chan-Ling, T. Cellular and physiological mechanisms underlying blood flow regulation in the retina and choroid in health and disease. Prog. Retin. Eye Res. 31, 377–406 (2012).
Sharifizad, M. et al. Retinal vessel diameters, flicker-induced retinal vasodilation and retinal oxygen saturation in high- and low-risk pregnancy. Acta Ophthalmol. 99, 628–636 (2021).
Heitmar, R., Lip, G. Y. H., Ryder, R. E. & Blann, A. D. Retinal vessel diameters and reactivity in diabetes mellitus and/or cardiovascular disease. Cardiovasc. Diabetol. 16, 56 (2017).
Nagele, M. P. et al. Retinal microvascular dysfunction in hypercholesterolemia. J. Clin. Lipidol. 12, 1523–1531 (2018).
Kotliar, K. E. et al. Dynamic retinal vessel response to flicker in obesity: A methodological approach. Microvasc. Res. 81, 123–128 (2011).
Machalinska, A. et al. Correlation between flicker-induced retinal vessel vasodilatation and plasma biomarkers of endothelial dysfunction in hypertensive patients. Curr. Eye Res. 43, 128–134 (2018).
Chen, K., Pittman, R. N. & Popel, A. S. Nitric oxide in the vasculature: where does it come from and where does it go? A quantitative perspective. Antioxid. Redox. Signal. 10, 1185–1198 (2008).
Disclosures
Riccardo Sacconi is a consultant for: Allergan Inc (Irvine, California, USA), Bayer Shering-Pharma (Berlin, Germany), Carl Zeiss Meditec (Dublin, USA), Novartis (Basel, Switzerland). Mario Pezzella, Nicolo’ Ribarich, Matteo Menean, Andrea Servillo: none. Francesco Bandello is a consultant for: Alcon (Fort Worth, Texas, USA), Alimera Sciences (Alpharetta, Georgia, USA), Allergan Inc (Irvine, California, USA), Farmila-Thea (Clermont-Ferrand, France), Bayer Shering-Pharma (Berlin, Germany), Bausch And Lomb (Rochester, New York, USA), Genentech (San Francisco, California, USA), Hoffmann-La-Roche (Basel, Switzerland), Novagali Pharma (Évry, France), Novartis (Basel, Switzerland), Sanofi-Aventis (Paris, France), Thrombogenics (Heverlee, Belgium), Zeiss (Dublin, USA). Giuseppe Querques is a consultant for: Alimera Sciences (Alpharetta, Georgia, USA), Allergan Inc (Irvine, California, USA), Bayer Shering-Pharma (Berlin, Germany), Heidelberg (Germany), Novartis (Basel, Switzerland), Sandoz (Berlin, Germany), Zeiss (Dublin, USA).
Author information
Authors and Affiliations
Contributions
RS, GQ: research design, data acquisition and analysis, interpretation of data, drafting the manuscript and critical revision of the manuscript. MP, NR, MM, AS: data acquisition and analysis, critical revision of the manuscript. FB: interpretation of data and critical revision of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Sacconi, R., Pezzella, M., Ribarich, N. et al. Benefits of dark chocolate intake on retinal vessels functionality: a randomized, blind, crossover clinical trial. Sci Rep 14, 20203 (2024). https://doi.org/10.1038/s41598-024-70289-7
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-024-70289-7
