
Abstract
This study aimed to survey the efficacy of chemotherapy regimens in the real world setting and explore the most promising regimen for patients experiencing early recurrence for gastric cancer. We retrospectively reviewed the clinical course of 207 patients with gastric cancer, who developed early recurrence during or within 6 months after completing S-1 adjuvant therapy at 19 Japanese institutions between 2012 and 2016. The treatment regimens after recurrence were fluoropyrimidines plus platinum-based regimens (FP) in 91 (44%) patients, paclitaxel-based regimens (PTX) in 102 (49%), and irinotecan-based regimens (IRI) in 14 (7%). The overall response and disease control rates were 28.7% and 54.1%. Median progression-free survival (PFS) and overall survival (OS) were 5.1 and 12.9 months, respectively. In the FP, PTX, and IRI regimens, the median PFS and OS were 5.9, 4.1, 4.1 months and 12.8, 12.9, and 11.8 months, respectively. The combination of PTX and ramucirumab showed survival comparable to capecitabine plus platinum. Multivariate analyses for OS showed that recurrence during adjuvant chemotherapy and undifferentiated histological type were independent poor prognostic factors. Although the prognosis of patients with early recurrence even with adjuvant S-1 was poor, PTX plus ramucirumab therapy could be a potential treatment option.
Similar content being viewed by others

Introduction
Gastric cancer (GC) is the six most common cancer, and the fourth leading cause of cancer deaths worldwide1. According to the results of the ACTS-GC phase III trial, surgery followed by adjuvant chemotherapy with S-1 alone for 1 year, has been the standard postoperative adjuvant chemotherapy for pStage II/III GC in Japan2,3. Recently, the JACCRO GC-07 trial demonstrated the superiority of adjuvant chemotherapy with docetaxel plus S-1 (DS) over S-1 monotherapy in patients with pStage III GC after D2 gastrectomy4,5, thereby recommending the DS regimen as a new option of the standard adjuvant chemotherapy for stage III GC in Japan. S-1-based postoperative adjuvant chemotherapy is a common practice in the Asia–Pacific region6,7.
Even after curative resection followed by adjuvant chemotherapy, some patients experience early relapse. Approximately 10–15% of patients in the S-1 group experienced relapse during adjuvant chemotherapy or within 6 months after completing S-1 monotherapy in the ACTS-GC trial8. As previous studies reported that patients with early relapse during or within 6 months after completing adjuvant chemotherapy exhibited poor prognosis, no established standard chemotherapy exists. It is thus necessary to establish the most optimal chemotherapy for these patients9,10.
In clinical practice, palliative chemotherapy regimen for patients with early relapse is selected depending on each doctor’s opinion and/or the policy of each institute. Following the failure of first-line chemotherapy with fluoropyrimidine plus platinum, some doctors opt for chemotherapy regimens containing taxane, which are considered the standard second-line chemotherapy. This preference arises from prior use of fluoropyrimidine (S-1) in postoperative adjuvant chemotherapy. Additionally, some doctors prefer combining platinum with fluoropyrimidine other than S-1 because it was not used in postoperative treatment. Thus, no consensus optimal chemotherapy regimen exists for patients with GC experiencing early relapse.
The present study aimed to survey the efficacy of chemotherapy regimens in the real world setting and explore the most promising regimen for early recurrence during or within 6 months after completing S-1 monotherapy.
Materials and methods
Patients
We retrospectively reviewed the data of patients with GC, who experienced early relapse during or within 6 months after completing adjuvant chemotherapy with S‑1 alone at 19 institutions in Japan between 2012 and 2016. We selected patients who met the following selection criteria: age ≥ 20 years old; Eastern Cooperative Oncology Group (ECOG) performance status (PS) 0–2; histological confirmation of gastric adenocarcinoma; early recurrence (during or within 6 months after completing S-1 adjuvant chemotherapy with S-1 alone) following R0 resection; no prior preoperative chemotherapy; palliative chemotherapy regimens after recurrence with fluoropyrimidine plus platinum-based, paclitaxel-based, or irinotecan-based treatments; and adequate organ function. The follow-up until recurrence was conducted regularly according to the Japanese guidelines. As a routine examination, the patient underwent computed tomography (CT) scans every 6 months after surgery, and tumor markers were tested at each visit. The CT scans were performed as needed when symptoms of recurrence or elevated tumor markers appeared. The study was approved by the institutional review boards of each institution.
For this study informed consent has been waived by Osaka Medical and Pharmaceutical University Hospital Institutional review board (IRB)/ethics committee due to the anonymity and retrospective nature of the study. An information disclosure document that was approved by the Ethics Review Committee of our hospital was published on the hospital’s website. The information disclosure document guarantees research participants and others the opportunity to refuse the implementation or continuation of research. In addition, this study was approved by the Ethical Review Committee of the Osaka Medical and Pharmaceutical University Hospital (No. 743-2539) and conducted with the research permission of the President. All methods were performed in accordance with relevant guidelines and regulations.
Evaluation and statistical analysis
The patients were divided into three groups according to the first chemotherapy regimens after recurrence: fluoropyrimidines plus platinum-based (FP) group, paclitaxel-based (PTX) group, and irinotecan-based (IRI) group.
We compared the overall survival (OS) and progression-free survival (PFS) among these three groups. OS was defined as the time from the initiation of chemotherapy after recurrence to death from any cause or censored at the last visit of surviving patients. PFS was calculated from the date of the initiation of chemotherapy to the date of progression, as assessed by image examination according to the RECIST ver. 1.1 or death from any cause, and surviving patients without disease progression were censored at the visit. Survival functions of OS and PFS were estimated using the Kaplan–Meier method and compared by the log-rank test.
To adjust for the patients’ background, survival differences, presented as the hazard ratio (HR) and 95% confidence interval (CI), among the treatment groups were estimated by multivariable analyses using Cox proportional hazard regression models, which included the chemotherapy regimens (FP-based versus PTX-based versus IRI-based), peritoneal dissemination (absent versus present), ascites (absent versus present), number of metastatic sites (0–1 versus ≥ 2), time of recurrence (during or within 6 months after completing adjuvant chemotherapy), and histology as covariates. Two-sided P-values < 0.05 indicated statistically significant differences. Statistical analyses were performed using the R software, version 4.2.3 (R Foundation for Statistical Computing, Vienna, Austria).
Results
Patient characteristics
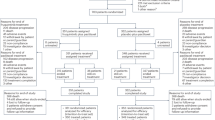
The data of 289 patients were collected. Figure 1 shows the CONSORT diagram of the study population. Eighty-two patients were excluded as they did not meet the selection criteria (best supportive care n = 29, other postoperative adjuvant chemotherapy n = 22, other treatment n = 16, and insufficient data n = 15). Finally, a total of 207 patients were analyzed in this study and their characteristics are shown in Table 1. The median age of the patients was 66 (range 42–84) years, and 147 (71%) were male. The median duration of adjuvant chemotherapy with S-1 was 245 (range 10–371) days, and 125 (60%) patients experienced recurrence during adjuvant chemotherapy. A total of 126 patients (61%) had diffuse-type histology, and 42 (20%) was positive for human epidermal growth factor receptor 2 (HER2). The detail of metastatic sites listed in Supplementary Table 1. The chemotherapy regimens were FP-based in 91 (44%), PTX-based in 102 (49%), and IRI-based in 14 (7%) patients.

Consort diagram.
In the FP-based group, the chemotherapy regimens were capecitabine plus cisplatin (XP) (n = 27, 30%), capecitabine plus oxaliplatin (XELOX) (n = 25, 27%), S-1 plus cisplatin (SP) (n = 9, 10%), XP plus trastuzumab (XP + Tmab) (n = 19, 21%), and others (n = 11, 12%). In the PTX-based group, the chemotherapy regimens were paclitaxel plus ramucirumab (PTX + RAM) (n = 44, 43%), PTX alone (n = 36, 35%), nab-PTX alone (n = 16, 16%), and others (n = 6, 6%). In the IRI-based group, the chemotherapy regimens were irinotecan plus cisplatin (IRI + CDDP) (n = 12, 86%) and IRI alone (n = 2, 14%). The details of the regimens in each group are listed in Table 2.
Efficacy of all analyzed patients
The median follow-up time was 14.2 (range 0.5–75.1) months. At the time of data cutoff, 20, 23, and 2 patients in the FP-, PTX-, and IRI-based groups, respectively, were continuing the chemotherapy, which were initiated after recurrence. The median PFS and OS were 5.1 months (95% CI 4.1–5.9) and 12.9 months (95% CI 11.4–15.7), respectively, in all analyzed patients (Fig. 2a,b). Among patients with measurable lesions (n = 122), the overall response rate (ORR) was 28.7% and disease control rates (DCR) was 54.1%. Of the 207 patients who discontinued each regimen, 137 (66.1%) received subsequent treatments.

(a,b) Kaplan–Meier analysis of overall survival and relapse-free survival.
Efficacy in treatment groups
Median PFS was 5.9 months (95% CI 5.1–8.0) in the FP-based group, 3.9 months (95% CI 2.7–5.9) in the PTX-based group, and 4.1 months (95% CI 2.4–N.A.) in the IRI-based group (Fig. 3a). Median Meanwhile, the OS was 12.8 months (95% CI 11.3–17.1) in the FP-based group, 12.9 months (95% CI 10.0–17.8) in the PTX-based group, and 11.8 months (95% CI 6.7–N.A.) in the IRI-based group, respectively (Fig. 3b). In the FP-based group, median OS was 6.2 months (95% CI 4.2–N.A.) in the S-1 plus cisplatin regimen group and 17.6 months (95% CI 11.4–27.5) in the capecitabine plus cisplatin regimen group (hazard ratio [HR] 0.37, 95% CI 0.16–0.83, P = 0.017) (Fig. 4a). In the PTX-based group, median OS was 11.5 months (95% CI 6.9–14.7) in the taxane-alone regimen group and 18.0 months (95% CI 10.1–30.1) in the taxane + RAM regimen group (HR 0.64, 95% CI 0.41–1.02, P = 0.063) (Fig. 4b).

(a,b) Kaplan–Meier analysis of overall survival and relapse-free survival in the treatment groups.

(a) Internal comparison of the S-1 plus cisplatin and capecitabine plus cisplatin groups; Kaplan–Meier analysis of overall survival. (b) Internal comparison of the taxane-alone and taxane plus ramucirumab groups; Kaplan–Meier analysis of overall survival.
Prognostic factors
Multivariate analysis for OS identified the timing of early recurrence (during vs after adjuvant chemotherapy, HR 1.456, 95% CI 1.05–2.01, P = 0.024) and histological type (undifferentiated vs differentiated, HR 1.489, 95% CI 1.06–2.09, P = 0.021) as independent prognostic factors. Chemotherapy regimens did not show statistically significant differences in OS (FP vs PTX vs IRI, HR 1.00 vs 0.92 [95% CI 0.66–1.27, P = 0.61] vs 1.12 [95% CI 0.59–2.09, P = 0.72]) (Table 3).
Exploratory comparisons between FP-based regimen and taxane plus RAM regimens
This exploratory analysis compared the survival between capecitabine plus platinum (n = 52) and taxane plus RAM (n = 47) receiving groups, excluding patients who received trastuzumab-containing therapy. Capecitabine containing regimens included XP (n = 27) and XELOX (n = 25), and the taxane plus RAM regimens comprised PTX plus RAM (n = 44) and nab-PTX plus RAM (n = 3). No significant differences were observed in the baseline characteristics between the capecitabine containing group and taxane plus RAM group (Supplementary Table 2). Median PFS was 5.9 months (95% CI 4.1–8.4) for capecitabine containing regimens and 5.7 months (95% CI 4.6–9.4) for PTX plus RAM regimens (HR 1.10; 95% CI 0.63–1.95, P = 0.71) (Supplementary Fig. S1a). The median OS was 13.9 months (95% CI 9.1–20.4) for capecitabine containing regimens and 18.0 months (95% CI 10.1–30.1) for taxane plus RAM regimens. (Supplementary Fig. S1b).
Discussion
This study collected the data of 207 patients who experienced early relapse during or within 6 months after adjuvant chemotherapy with S-1, which is the largest cohort compared with those of previous reports. This multicenter, cohort study revealed some important results. First, most of the patients received non-S-1 containing regimens, and more than half received a PTX containing chemotherapy. While previous reports of systemic chemotherapy for early recurrence showed a response rate of 24.7%, median PFS of 3.7 months, and median OS of 11.4 months10, this study demonstrated a response rate of 25.9%, median PFS of 5.1 months, and median OS of 12.9 months. These efficacy parameters were consistently worse than those reported in the clinical trials using first-line chemotherapy for advanced GC, which included patients with “not-early” recurrence. In the multivariate analysis, the timing of early relapse and histological type were independent and poor prognostic factors for OS (P < 0.05). The poor prognosis of patients with early recurrence during or within 6 months after postoperative adjuvant chemotherapy was potentially attributed to the rapid growth and resistance to chemotherapy.
For patients who experience recurrence during or within 6 months after completing adjuvant chemotherapy, the 2021 edition of the Gastric Cancer Treatment Guidelines in Japan recommends avoiding chemotherapy regimens containing drugs previously administered in the adjuvant setting11. This recommendation is partly based on the retrospective analysis reporting that S-1 plus cisplatin was ineffective in patients with recurrent GC, especially with a relapse-free interval (RFI) of less than 6 months after adjuvant S-1 chemotherapy9. In their report, the efficacy of S-1 plus cisplatin was less in patients with an RFI of < 6 months than in those with an RFI of ≥ 6 months, with a response rate of 37.5 vs. 5.0%, a median PFS of 6.2 vs. 2.3 months, and a median OS of 16.6 vs. 7.3 months. Moreover, the JACCRO-GC05 and CCOG0701 trials investigated the clinical significance of continuing S-1 in the second-line chemotherapy in combination with irinotecan and paclitaxel, respectively, beyond disease progression during the first-line chemotherapy with S-1 plus cisplatin12,13. The results of these trials suggested no benefit of continuous use of S-1 beyond progression, which could be applied for patients with early recurrence during or within 6 months of adjuvant chemotherapy containing S-1.
Conversely, since platinum is a key drug which is not used in the adjuvant chemotherapy for the treatment of patients with early relapse after adjuvant chemotherapy with S-1, platinum plus capecitabine is a candidate treatment for these patients, considering that capecitabine has a different mode of action than S-1. A phase II study conducted in Korea evaluated the efficacy and safety of capecitabine plus cisplatin in patients with recurrent CG after fluorinated pyrimidine-based adjuvant chemotherapy, and revealed a response rate of 28% and median PFS of 5.8 months14. Furthermore, a phase II study conducted in Japan evaluated the efficacy and safety of capecitabine plus cisplatin in patients with early relapse after adjuvant S-1 chemotherapy, and the response rate was 26.7% and the median PFS was 4.4 months15. In our study, the capecitabine plus cisplatin regimen showed statistically significant superiority over the S1 plus cisplatin regimen in OS (HR 0.37, 95% CI 0.16–0.83, P = 0.017). These results suggest that capecitabine plus cisplatin may be more effective than S-1 plus cisplatin for patients with early relapse after S-1 adjuvant chemotherapy. Recently, S-1 plus docetaxel has emerged as a new standard adjuvant chemotherapy for pathological stage III GC4. Capecitabine plus platinum is anticipated to demonstrate certain efficacy for early relapse after adjuvant chemotherapy with S-1 plus docetaxel. Furthermore, the addition of immune checkpoint inhibitors or approved molecular targeted agents to platinum plus fluoropyrimidine is expected to enhance efficacy.
Currently, ramucirumab, a fully human monoclonal antibody that selectively targets vascular endothelial growth factor receptor-2, plus paclitaxel (RAM plus PTX), is the standard second-line treatment after failure of fluoropyrimidine plus platinum in the first-line16,17. This is the first report showing the efficacy of taxan plus RAM in patients with early recurrence after S1. In this study, the taxane plus RAM regimen showed an OS benefit comparable to that of the capecitabine containing regimens (HR 0.85; 95% CI 0.53–1.38, P = 0.52). This suggests that the combination of taxane plus RAM may be a favorable treatment option for GC with early recurrence after adjuvant S‑1 monotherapy. Recently, fluoropyrimidine plus oxaliplatin showed survival benefits in the peri-operative setting. It is considered that taxane plus RAM may be the first-choice for early recurrence after the platinum doublet peri-operative chemotherapy because the clinical significance of switching platinum from oxaliplatin to cisplatin has not been clarified yet.
Furthermore, the IRI-based group showed a certain level of efficacy. Recently, peri-operative chemotherapy with FLOT (docetaxel plus oxaliplatin plus leucovorin plus 5-fluorouracil) has become a standard of care for patients with resectable locally advanced GC, demonstrating significant survival benefits compared with that of ECF (epirubicin plus cisplatin plus continuous infusion 5-fluorouracil)18,19. Thus, progression under or rapid disease recurrence after FLOT in the peri-operative setting raises another demand for an alternative chemotherapy after early recurrence. The phase II RAMIRIS trial (NCT03081143) was conducted to compare RAM plus FOLFIRI with PTX plus RAM, as a second line treatment for patients with advanced or metastatic gastroesophageal adenocarcinoma, including those who have progressed after chemotherapy with FLOT20. The trial demonstrated promising efficacy of FOLFIRI plus RAM compared with that of PTX plus RAM in FLOT-pretreated subgroup, with an ORR of 25% vs. 8% and median PFS of 4.6 vs. 2.1 months. Accordingly, FOLFIRI plus RAM regimen is regarded as one of the optimal second-line chemotherapy for early recurrence after peri-operative triplet chemotherapy. In Japan, the OGSG1901 study is currently underway to evaluate the efficacy of IRI plus Ram for patients with GC with early recurrence during or after adjuvant DS21.
This study has some limitations. First, it was a retrospective study, which might include some bias in selecting the various treatment regimens. Second, the chemotherapy dose, duration, and confirmation of HER2 status were not unified. Thus, potential differences exist in treatment approaches among the participating institutions. Third, there were no information about subsequent treatments. Fourth, the combination therapy of cytotoxic agents and immune checkpoint inhibitors or molecular target agents were not included in this study. The combination therapy containing immune checkpoint inhibitors or molecular targeted agents might be also a promising approach for future progress for patients with GC who are experiencing early relapse after adjuvant S-1 chemotherapy. Moreover, biomarkers such as HER2, PD-L1, microsatellite status, and Claudin 18.2 were not collected in this study. These biomarkers will be essential in future studies of this patient population. Sixth, this study is real-world data and has not been adjusted for patient background factors in the prognostic analysis. Therefore, patient background bias may have had a confounding effect on prognosis. Finally, data regarding toxicities and quality of life were not collected during our study.
In conclusion, the prognosis of patients with early recurrence of adjuvant chemotherapy with S-1 alone was poor. S-1 should be discontinued, and PTX plus RAM therapy could be a treatment option. However, it remains unclear which is better: PTX plus RAM, capecitabine plus platinum with/without immune checkpoint inhibitors, or molecular targeted agents.
Data availability
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
References
Sung, H. et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 71(3), 209–249 (2021).
Sakuramoto, S. et al. Adjuvant chemotherapy for gastric cancer with S-1, an oral fluoropyrimidine. N. Engl. J. Med. 357, 1810–1820 (2007).
Sasako, M. et al. Five-year outcomes of a randomized phase III trial comparing adjuvant chemotherapy with S-1 versus surgery alone in stage II or III gastric cancer. J. Clin. Oncol. 29, 4387–4393 (2011).
Yoshida, K. et al. Addition of docetaxel to oral fluoropyrimidine improves efficacy in patients with stage III gastric cancer: Interim analysis of JACCRO GC-07, a randomized controlled trial. J. Clin. Oncol. 37, 1296–1304 (2019).
Kodera, Y. et al. Addition of docetaxel to S-1 results in significantly superior 5-year survival outcomes in Stage III gastric cancer: A final report of the JACCRO GC-07 study. Gastric Cancer. 26, 1063–1068 (2023).
Muro, K. et al. Pan-Asian adapted ESMO Clinical Practice Guidelines for the management of patients with metastatic gastric cancer: A JSMO-ESMO initiative endorsed by CSCO, KSMO, MOS, SSO and TOS. Ann. Oncol. 30, 19–33 (2019).
Shitara, K. et al. Pan-Asian adapted ESMO Clinical Practice Guidelines for the diagnosis, treatment and follow-up of patients with gastric cancer. ESMO Open. 9, 102226 (2024).
Ito, S., Ohashi, Y. & Sasako, M. Survival after recurrence in patients with gastric cancer who receive S-1 adjuvant chemotherapy: Exploratory analysis of the ACTS-GC trial. BMC Cancer. 18, 449 (2018).
Shitara, K. et al. Combination chemotherapy with S-1 plus cisplatin for gastric cancer that recurs after adjuvant chemotherapy with S-1: Multi-institutional retrospective analysis. Gastric Cancer. 15, 245–251 (2012).
Mitani, S. et al. Systemic chemotherapy for gastric cancer with early recurrence after adjuvant S-1 monotherapy: A multicenter retrospective study. Int. J. Clin. Oncol. 24, 1197–1203 (2019).
Japanese Gastric Cancer Association. Japanese gastric cancer treatment guidelines 2021 (6th edition). Gastric Cancer. 26, 1–25 (2023).
Tanabe, K. et al. Phase II/III study of second-line chemotherapy comparing irinotecan-alone with S-1 plus irinotecan in advanced gastric cancer refractory to first-line treatment with S-1 (JACCRO GC-05). Ann. Oncol. 26, 1916–1922 (2015).
Nakanishi, K. et al. Phase II multi-institutional prospective randomized trial comparing S-1 plus paclitaxel with paclitaxel alone as second-line chemotherapy in S-1 pretreated gastric cancer (CCOG0701). Int. J. Clin. Oncol. 21, 557–565 (2016).
Kang, H. J. et al. Phase II study of capecitabine and cisplatin as first-line combination therapy in patients with gastric cancer recurrent after fluoropyrimidine-based adjuvant chemotherapy. Br. J. Cancer. 92, 246–251 (2005).
Nishikawa, K. et al. A phase II trial of capecitabine plus cisplatin (XP) for patients with advanced gastric cancer with early relapse after S-1 adjuvant therapy: XParTS-I trial. Gastric Cancer. 21, 811–818 (2018).
Fuchs, C. S. et al. Ramucirumab monotherapy for previously treated advanced gastric or gastro-oesophageal junction adenocarcinoma (REGARD): An international, randomised, multicentre, placebo-controlled, phase 3 trial. Lancet. 383, 31–39 (2014).
Wilke, H. et al. Ramucirumab plus paclitaxel versus placebo plus paclitaxel in patients with previously treated advanced gastric or gastro-oesophageal junction adenocarcinoma (RAINBOW): A double-blind, randomised phase 3 trial. Lancet Oncol. 15, 1224–1235 (2014).
Al-Batran, S. E. et al. Effect of neoadjuvant chemotherapy followed by surgical resection on survival in patients with limited metastatic gastric or gastroesophageal junction cancer: The AIO-FLOT3 trial. JAMA Oncol. 3, 1237–1244 (2017).
Al-Batran, S. E. et al. FLOT4-AIO Investigators. Perioperative chemotherapy with fluorouracil plus leucovorin, oxaliplatin, and docetaxel versus fluorouracil or capecitabine plus cisplatin and epirubicin for locally advanced, resectable gastric or gastro-oesophageal junction adenocarcinoma (FLOT4): A randomised, phase 2/3 trial. Lancet. 393, 1948–1957 (2019).
Lorenzen, S. et al. FOLFIRI plus ramucirumab versus paclitaxel plus ramucirumab for patients with advanced or metastatic adenocarcinoma of the stomach or gastroesophageal junction as second-line therapy: Interim safety and efficacy results from the phase II RAMIRIS Study (AIO-STO-0415) of the German Gastric Group at AIO. J. Clin. Oncol. 37(15), 4023 (2019).
Yamaguchi, T. et al. Protocol of OGSG 1901: A phase II trial of ramucirumab plus irinotecan for patients with early relapsed gastric cancer during or after adjuvant docetaxel plus S-1 therapy. BMC Cancer. 22, 773 (2022).
Acknowledgements
We thank all the study participants, their families, physicians, nurses, and staff members who supported this research.
Funding
No funding source was involved in the study.
Author information
Authors and Affiliations
Contributions
T.Y.: drafting of the article. T.Y. and N.B.: conception and design. T.Y. and K.N.: formal analysis. T.Y., K.K., S.Y., T.N., K.N., M.W., R.M., K.K., T.M., S.K., S.H., H.C., N.K., S.O., T.Y., Y.I. and N.B.: investigation and resources. All authors: writing—review and final approval of the article.
Corresponding author
Ethics declarations
Competing interests
Dr. Kengo Nagashima reports consulting fees from SENJU Pharmaceutical Co., Ltd, Toray Industries, Inc., and Kowa Company, Ltd, outside the submitted work. Dr. Takanobu Yamada reports personal fees from Taiho, Ono pharmaceutical, Bristol Squib Mayers, and Johnson and Johnson, outside the submitted work. Dr. Haruhiko Cho reports personal fees from Yakult Honsha, outside the submitted work. Dr. Shigenori Kadowaki reports personal fees from MSD, Merck KgaA, Eli Lilly, Bayer, Daiichi Sankyo, Eisai, Taiho, Ono pharmaceutical, Bristol Squib Mayers, and Chugai Pharmaceutical, outside the submitted work. Dr. Narikazu Boku reports personal fees from Taiho and Ono, Eli Lilly, Taiho, Daiichi Sankyo, and Bristol-Myers Squibb, outside the submitted work. All remaining authors have declared no conflicts of interest.
Ethics approval and consent to participate
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1964 and later versions. For this study informed consent has been waived by Osaka Medical and Pharmaceutical University Hospital Institutional review board/ethics committee due to the anonymity and retrospective nature of the study. An information disclosure document that was approved by the Ethics Review Committee of our hospital was published on the hospital’s website.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Yamaguchi, T., Kumagai, K., Yagi, S. et al. Efficacy of chemotherapy for patients with gastric cancer with early recurrence during or after adjuvant chemotherapy with S-1 alone: a multicenter retrospective study. Sci Rep 14, 21854 (2024). https://doi.org/10.1038/s41598-024-72423-x
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-024-72423-x
