
Abstract
The incidence of iodinated contrast media (ICM)-related adverse drug reactions (ADRs) varies significantly by procedure type. Compared other procedure types, cerebrovascular interventional procedures substantially increase the incidence of contrast-induced encephalopathy (0.38-2.90%). The associations of ioversol (nonionic low-osmolal ICM) with central nervous system (CNS) ADRs and iodixanol (nonionic ios-osmolal ICM) with cutaneous ADR manifestations have been establishe. This study aimed to compare the incidence of CNS ADRs and evaluate the occurrence, extent, and risk factors for ADRs associated with ioversol and iodixanol use during cerebrovascular interventional procedures. We conducted a prospective study involving 1,015 participants with suspected cerebrovascular diseases from July 2019 to July 2022. Participants underwent cerebrovascular interventional procedures with either iodixanol or ioversol administration. Data on ioversol and iodixanol-related CNS ADRs, data on other ADRs, and participants’ baseline information were collected. Out of 848 participants (average age, 61.5 ± 12.6 years; 205 females) who received ICM, 16.7% (142 of 848) experienced CNS ADRs. Compared with iodixanol, ioversol was associated with a greater rate of CNS ADRs (12.6% vs. 21.1%, P = 0.001, RR = 1.666). Iodixanol was associated with higher rates of numbness and blurred vision (29.1% vs. 14.9%, P = 0.042), whereas ioversol was associated with higher incidences of headache and overall ADRs during the procedures (20.0% vs. 46.0%, P = 0.002). Logistic regression analysis revealed that a history of allergic diseases was a risk factor for iodixanol-related ADRs (odds ratio [OR], 2.5; 95% confidence interval [CI]: 1.2–4.9; P = 0.010). Severe cerebral vascular stenosis (OR, 2.8; 95% CI: 1.8–4.4; P < 0.001), female sex (OR, 0.5; 95% CI: 0.3–0.8; P = 0.005) and relatively young age (OR, 0.97; 95% CI: 0.95–0.99; P = 0.004) were risk factors for ioversol-related ADRs. Iodixanol appears to have a lower likelihood of causing ICM-related CNS ADRs than does ioversol during cerebrovascular interventional procedures.
Similar content being viewed by others

Introduction
Iodinated contrast media (ICM) have become indispensable in endovascular imaging and procedures, particularly in cerebrovascular interventional procedures such as cerebral angiography, intra-arterial mechanical thrombectomy for acute ischaemic stroke, and endovascular treatment for cerebral stenosis or aneurysms. In the US, the approximately 75 million computed tomography (CT) scans are performed annually, and ICM is utilized in half of them1.
Statistics from China’s advanced stroke centres indicated a significant increase in the use of mechanical thrombectomy, increasing sharply from 1,821 procedures in 2014 to 29,580 procedures in 20192. Concurrently, as the clinical application of ICM in cerebrovascular diagnostic imaging and interventional procedures has expanded, reports of ICM-related adverse drug reactions (ADRs) have increased3,4,5. These ADRs, which range from allergic-like to physiological events, can be categorized by severity into mild, moderate, and severe reactions. While the majority of these events are noncritical, severe manifestations, especially contrast-induced encephalopathy (CIE)3,4,5, have garnered increased attention because of their potential implications for the central nervous system (CNS).
The existing data indicate that the incidence of ICM-related ADRs in patients undergoing enhanced CT or magnetic resonance imaging (MRI) examinations ranges from 0.13–0.99%6,7,8,9. However, studies focusing on coronary angiography suggest increased frequencies of acute ADRs ranging from 3.6 to 12.7%, and delayed ADRs ranging from 15.1–24.8%10,11. The incidence of ICM-related ADRs is low, with the majority of cases being noncritical. However, identifying severe manifestations, such as CIE, is crucial in clinical practice. The incidence of CIE in the coronary artery pathway is between 0.13% and 0.51%12,13, this incidence is notably greater in the cerebrovascular pathway, ranging from 0.38–2.90%4,14,15. This underscores the challenges in extrapolating data on coronary contrast-related ADRs to cerebrovascular ADRs, suggesting that the incidence and symptoms of ICM-related ADRs might differ on the basis of the intervention route.
Previous research has demonstrated that nonionic low-osmolal iodinated contrast media (LOCM) predominantly results in CNS symptoms16, whereas nonionic iso-osmolal iodinated contrast media (IOCM) primarily causes cutaneous system symptoms17. These findings suggest that specific ICM types might predispose patients to distinct patterns of ADRs, especially concerning CNS events. However, there remains a glaring gap in research—the absence of a systematic study furnishing clinical evidence on the best ICM type for use in cerebrovascular interventional procedures. Previous ICM-related ADR studies have been retrospective, and researchers often ignore transient and mild ADRs during intravascular ICM injection6,8.
In this prospective, randomized controlled trial, we compared ADRs associated with ioversol (LOCM) and iodixanol (IOCM). Our objective was to determine the incidence of CNS ADRs and to delineate the occurrence, magnitude, and risk factors for other ADRs associated with the use of these agents during cerebrovascular interventions. To date, no substantial studies have focused on elucidating the frequency and severity of CNS ADRs by comparing ioversol and iodixanol in this context.
Materials and methods
Study design and participants
All participants or their representatives provided written informed consent before entering the trial. All identifiable participant data were anonymized. This study was a double-blind, monocentric, randomized controlled trial aimed at evaluating CNS and overall ADRs associated with ioversol and iodixanol use during cerebrovascular interventional procedures. The research took place from July 2019 to July 2022. Neither patients nor the public were involved in the design, conduct, reporting, or dissemination plans of our research. The trial has been reported in line with the Consolidated Standards of Reporting Trials (CONSORT) Guidelines18. We confirmed that all methods were performed in accordance with the American College of Radiology Manual on Contrast Media 2019. The study protocol received approval from the Ethics Committee of the 940th Hospital of Joint Logistics Support Force of the Chinese People’s Liberation Army (Approval No. 2018KYLL082). We registered this study on the Chinese Clinical Trial Registry and received a trial number (www.chictr.org.cn, ChiCTR1900024679, 20/07/2019).
The inclusion criteria were as follows:1 suspected cerebrovascular disease, encompassing cerebral arterial thrombosis, transient ischaemic attack, aneurysm, arteriovenous malformation, arteriovenous fistula, venous thrombus, or idiopathic intracranial hypertension;2 reexamination for cerebrovascular disease; and3 the provision of informed consent.
The exclusion criteria for participants were as follows:1 were under 18 years of age;2 had local infection at the puncture site;3 were pregnant or breastfeeding;4 had a cerebral hernia;5 were on dialysis;6 had an international normalized ratio (INR) > 1.7 or platelet count < 100 × 10^9/L;7 had a KILLIP class ≥ III or a New York Heart Association class ≥ III;8 had severe nervous system injury diseases (National Institutes of Health Stroke Scale score > 5);9 could not communicate normally due to deafness, aphasia, a psychiatric disorder, or general anaesthesia (patients undergoing cerebrovascular interventional procedure for arterial vascular malformation, acute ischaemic stroke, aneurysms, or intracranial vascular stenosis); and10 had hyperthyroidism.
Randomization and masking
Random numbers were generated for participant assignment to either the iodixanol or ioversol group at a 1:1 ratio using SPSS 25.0. Both assessors and participants remained blind to the treatment allocation. The sealed randomization list was unsealed only in cases of severe ADRs necessitating treatment intervention.
Procedures
A detailed medical history covering patient baseline characteristics, previous allergic reactions, laboratory test results, specifics on ioversol and iodixanol administration, and details of any AE occurrence was obtained prior to ioversol and iodixanol administration.
Before enrolling, participants agreed to provide informed consent according to the American College of Radiology (version 10.3) standards. Preprocedural medication procedures were followed. Iodixanol (Visipaque320, GE Healthcare Ireland, Supplemental Table 3) or ioversol (Optiray320, Mallinckrodt Medical, Supplemental Table 3) was used, as dictated by the random assignment table.
To ascertain the accuracy of the ADRs induced by ioversol and iodixanol, the symptoms of new-onset ADRs following the injection of ioversol and iodixanol were evaluated by two neurologists in an independent assessment.
Outcomes
The primary outcome was the incidence of CNS ADRs induced by ioversol and iodixanol during and after the procedures. The secondary outcomes included the frequency, severity, and risk factors for ioversol- and iodixanol-related ADRs. A patient’s new symptoms of discomfort were not considered ioversol- or iodixanol-related ADRs until ioversol and iodixanol were injected into their artery. ADRs were graded as mild in patients whose symptoms were self-limited without evidence of progression, moderate in patients whose symptoms were more pronounced and required medical management, severe in patients showing symptoms were life-threatening and resulted in permanent morbidity or death if not managed appropriately19. Further details on ADR classification are provided in supplementary information Table 1. ADRs were evaluated by two independent neurologists not involved in the procedures. Discrepancies were settled by a senior neurologist. Assessments for acute ADRs were performed during and one hour after the procedure, whereas delayed ADRs were assessed at intervals of 1, 2,and 7 days after the procedure.
Statistical analysis
Baseline data are summarized using standard descriptive statistics. Continuous variables were evaluated using t- tests, and categorical variables were evaluated through the X2 test. Kaplan-Meier curves were used to compare the cumulative incidence of ADRs to 7 days after randomization, which was tested by the log-rank test. Associations between potential risk factors and ioversol and iodixanol-related ADRs were explored using binary logistic regression. Significant potential risk factors were identified by univariate logistic regression analyses (t test or χ2 test) (P < 0.05), and subsequently entered into a multivariate logistic regression analysis with candidate variables of risk factors from previous studies to identify risk factors (P < 0.05). Analyses were conducted using SPSS version 25.0, with statistical significance set at P < 0.05.
Results
Baseline information of the Ioversol group and Iodixanol group
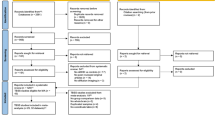
A total of 1015 participants were assessed for eligibility. Among these participants, 916 met the eligibility and exclusion criteria and were subsequently randomized. Specifically, 462 participants received iodixanol, whereas 454 received ioversol. Sixty-eight participants (27 from the iodixanol group and 41 from the ioversol group) were subsequently excluded because they withdrew from the follow-up after their respective procedures.
The final analysis incorporated data from 848 participants (Fig. 1). The average age of these participants was 61.5 ± 12.6 years, and the sample included 205 females. Notably, the baseline characteristics, such as personal and medication histories, were evenly distributed between the two groups, as shown in Table 1. The proportions of participants who received various types of interventions are shown in supplementary information Table 2.

Patient flowchart delineating (a) the number of eligible participants assessed for enrolment, (b) enrolment outcomes (inclusions/exclusions and reasons), and (c) final cohort allocation with complete adverse drug reaction data ascertained for analysis of the ioversol and iodixanol groups. INR = International normalized ratio, NYHA = New York Heart Association.
Primary outcomes
Among the 848 participants analysed in this study, 142 (16.7%) experienced CNS ADRs. Importantly, some participants reported experiencing multiple symptoms. When the two groups were compared, ioversol had a statistically significant association with a higher rate of CNS ADRs. Specifically: in the iodixanol group: 55 out of 435 participants (12.6%) experienced CNS ADRs; in the ioversol group: 87 out of 413 participants (21.1%) experienced CNS ADRs. The difference was statistically significant (P = 0.001, RR = 1.666), The risk of CNS ADRs was 1.67 times greater in patients who received ioversol injections than in those who received iodixanol injections. Ioversol was associated with greater rates of headache: 11 of 55 (20.0%) for iodixanol vs. 40 of 87 (46.0%) for ioversol (P = 0.002); iodixanol was associated with greater rates of numbness: 5 of 55 (9.1%) for iodixanol vs. 1 of 87 (1.1%) for ioversol (P = 0.032); and iodixanol was associated with greater rates of blurred vision: 16 of 55 (29.1%) for iodixanol vs. 13 of 87 (14.9%) for ioversol (P = 0.042). There was no significant difference in the occurrence of other CNS symptoms between the iodixanol and ioversol groups. These results are described in Table 2.
Secondary outcomes
Among the 848 participants analysed in this study, 266 (31.4%) experienced ioversol and iodixanol-related ADRs. Ioversol was associated with a greater overall occurrence of ADRs: 143 of 413 participants (34.6%) for ioversol vs. 123 of 435 participants (28.3%) for iodixanol. The difference was statistically significant (P = 0.046, RR = 1.225). The risk of ADRs was 1.22 times greater in patients who received ioversol injections than in those who received iodixanol injections. The Kaplan‒Meier curves for the cumulative incidence of ADRs until 7 days after randomization are shown in Fig. 2. The incidence of ADRs in the ioversol group was significantly greater than that in the iodixanol group (log-rank P = 0.041). When we analysed the occurrence of ADRs according to timing, iodixanol was linked to a higher rate of delayed ADRs: 50 of 435 (11.5%) participants vs. 31 of 413 (7.5%) participants for ioversol (P = 0.048); however, ioversol had a higher rate of acute ADRs: 89 of 435 (20.5%) participants for iodixanol vs. 123 of 413 (29.8%) participants for ioversol (P = 0.002).

Time-to-ADRs by day 7. Kaplan-Meier curves for the cumulative incidence of ICM-related ADRs from randomization to day 7 after cerebrovascular interventional procedures.
When we analysed the occurrence of ADRs according to severity, iodixanol was associated with greater rates of moderate and severe ADRs: 25 of 435 (5.7%) participants for iodixanol vs. 10 of 413 (2.4%) participants for ioversol (P = 0.015); ioversol was associated with a greater rate of mild ADRs: 98 of 435 (22.5%) participants for iodixanol vs. 133 of 413 (32.2%) participants for ioversol (P = 0.002).
With respect to other symptoms of ioversol- and iodixanol-related ADRs, iodixanol was associated with a greater rate of cutaneous symptoms of ADRs: 24 of 435 (5.5%) participants for iodixanol vs. 7 of 413 (1.7%) participants for ioversol (P = 0.003). There was no significant difference in other clinical symptoms between the two groups.
Risk factors for the occurrence of ioversol- and iodixanol-related ADRs
Iodixanol
A history of allergic disease was identified as a significant risk factor for iodixanol-related ADRs. Among the participants who experienced ADRs, 13.8% had a history of allergic disease, whereas 6.1% did not (P = 0.008) (Table 3). Univariate logistic regression revealed that a history of allergic disease (OR: 2.5; 95% CI: 1.2–4.9; P = 0.010) was a risk factor for iodixanol-related ADRs. Even after adjusting for age, hypertension, and diabetes, multiple logistic regression confirmed a history of allergic disease (OR: 2.6; 95% CI: 1.3–5.1; P = 0.008) as a dependent risk factor for iodixanol-related ADRs (Fig. 3).

Multiple logistic regression analysis according to ioversol and iodixanol-related risk factors. aAllergic disease was defined as the presence of any of the following: bronchial asthma, allergic rhinitis, atopic dermatitis, urticaria, drug allergy (antibiotics, NSAID, sulfa, or pyrine), or food allergy.*P value < 0.05, CI = confidence interval, OR = odds ratio.
Ioversol
Age, female sex, intraoperative hypertension, and severe cerebral vascular stenosis were identified as candidate risk factors for ioversol-related ADRs: Age: participants who experienced ADRs (59.1 ± 14.1 years) vs. those who did not experience ADRs (63.0 ± 11.5 years) (P = 0.005); female sex: participants who experienced ADRs (13.8%) vs. those who did not experience ADRs (6.1%) (P = 0.008); and intraoperative hypertension: participants who experienced ADRs (65.0%) vs. those who did not experience ADRs (75.2%) (P = 0.029). Severe cerebral vascular stenosis: With ADRs (60.1%) vs. without ADRs (38.5%) (P = 0.001) (Table 3). Multiple logistic regression identified severe cerebral vascular stenosis (OR: 2.8; 95% CI: 1.8–4.4; P < 0.001), female sex (OR: 0.5; 95% CI: 0.3–0.8; P = 0.005), and a relatively young age (OR: 0.97; 95% CI: 0.95–0.99; P = 0.004) as dependent risk factors for ioversol-related ADRs (Fig. 3).
Discussion
The correlation between the type of contrast medium used (ioversol vs. iodixanol) and the onset of ICM-related ADRs in patients undergoing cerebrovascular interventional procedures remains unclear because of the lack of extensive randomized clinical trials. In our study, we found that ioversol had a greater propensity for CNS-related ADRs than did iodixanol in this procedural context. Specifically, acute ADRs were more prevalent in the ioversol group, whereas the iodixanol group experienced more delayed ADRs and skin reactions. Our study, which was a randomized control trial on this topic, revealed that the majority of ICM-related ADRs predominantly impact the CNS (142 of 266, 53.3%), a finding that is distinct from studies focused on intravenous and cardiac catheterization methods6,10,11. These discrepancies can be attributed to the direct injection of ICM into the carotid artery, which can notably increase areas of blood‒brain barrier (BBB) disruption20. This mechanism can explain the increased rate of CNS ADRs in patients undergoing cerebrovascular interventional procedures.
The overall incidence of ADRs in this study was 31.4% (266 of 848), which was similar to the results of previous studies (33.2–37%) of cerebral angiography21,22 and was significantly greater than that reported in previous intravenous and coronary angiography studies. In previous studies of ICM-related ADRs, investigators generally ignored transient neurological ADRs (headache, dizziness, etc.), although we still rigorously included these transient ICM-related ADRs in the statistical indicators of the study according to the criteria of the ACR Handbook of Contrast Agents (2020)19. Previous experiments have demonstrated that ICM has time- and concentration-dependent cytotoxic effects, with the degree of disruption to the BBB dependent on the osmolality of the ICM23,24. Compared with iodixanol, ioversol, an LOCM, is characterized mainly by high osmotic pressure (Osmoality at 37 °C; iodixanol vs. ioversol: 290mOsm/kg.H2O versus 710 mOsm/kg.H2O). Previous studies in animals have shown that intracarotid injection of ICM has the potential to disrupt the BBB, with subsequent leakage from the bloodstream into the brain parenchyma. The degree of disruption of the BBB has been shown to depend on the osmolality of the injected material25,26,27. We found that CNS ADRs were more common with the use of ioversol (iodixanol vs. ioversol: 55 of 435, 12.6% versus 87 of 413, 21.1%, P = 0.001), suggesting that its osmotoxicity might be responsible for the higher rate of CNS symptoms and acute ADRs in the given procedures. Past experiments have also indicated that iodixanol has a relatively mild effect on blood flow and headaches28, which aligns with our findings. The trial also mirrors European trials indicating that iodixanol tends to cause less injection-related pain29, and that iodixanol was associated with greater rates of blurred vision, which was in agreement with a previous study reporting a higher incidence of visual symptoms (such as flashing lights) induced by iodixanol than by ioxaglate in patients undergoing cerebral arteriography30. These results might be related to the increase in infiltrating inflammatory cells, vasodilation, and macrophage degranulation after iodixanol administration31. Furthermore, our findings align with the literature indicating a greater likelihood of delayed ADRs and skin reactions in patients receiving iodixanol10,11,32. However, the detection of risk factors for severe ICM-related ADRs and ICM-induced encephalopathy is of clinical importance. Nevertheless, in the present study, only 3 severe ADRs were reported; thus, we combined the data of moderate and severe ADRs for statistical analysis. The results revealed that patients with a history of allergic disease are especially vulnerable after iodixanol administration33, with many requiring intervention with hydrocortisone or antihistamines. For ioversol-related risk factors, our observations align with prior research pinpointing demographic factors, such as patinets who are younger and female, as vulnerable subgroups34. On the basis of previous studies that considered stroke4,15 as a risk factor, our results further demonstrated that severe cerebrovascular stenosis may be a potential risk factor.
Osmolality may be the primary determinant of CNS ADRs in patients undergoing cerebrovascular interventional procedures. Ioversol exacerbates BBB injury via osmotic cytotoxicity, whereas iodixanol’s lower osmolality reduces CNS risk but predisposes patients to immune-mediated delayed reactions. The distinct physicochemical properties of ioversol and iodixanol underlie their differential risk profiles. Ioversol-related ADRs were significantly associated with younger age, female sex, and severe cerebrovascular stenosis in this study. Conversely, iodixanol-related ADRs were predominantly linked to a history of allergic disease.
Our study’s strength lies in its pioneering nature—it isthe first of its kind to evaluate the effects of iodixanol and ioversol on CNS-related ADRs during cerebrovascular interventional procedures. However, this study is not without its limitations. The assessment of mild ADRs is primarily based on participants subjective experience of discomfort following the injection of ICM, for which there is a paucity of more objective evaluation indicators. Furthermore, being a single-centre study with a moderately sized sample precludes wide generalizations. Finally, the lack of immunological evaluations and skin biopsies curtails the understanding of the interplay between the immune system and ICM-related ADRs in this study.
Conclusions
Iodixanol appears to be safer for patients undergoing cerebrovascular interventional procedures, with a reduced risk of CNS ADRs compared with ioversol, but it causes were more delayed and cutaneous symptom ADRs. A younger age, female sex and severe cerebral vascular stenosis were significant risk factors for ioversol-related ADRs. A history of allergic disease was a significant risk factor for iodixanol-related ADRs. However, these observations necessitate validation in larger-scale, diverse, and multicentre randomized controlled trials.
Data availability
Prior to the start of the study, we registered on the Chinese Clinical Trial Registry and received a trial number (www.chictr.org.cn, ChiCTR1900024679). All data generated or analysed during this study are included in this published article and its supplementary information files.
Change history
10 October 2025
The original online version of this Article was revised: The Funding section in the original version of this Article was omitted. The Funding section now reads: “This research was funded by Key Public Relations Project of the Health and Family Planning Commission of Gansu Province (GSSZD2024-06); Key Talent Project of Gansu Province (2025RCXM068); Major Research Projects of the Gansu Provincial Center Hospital (ZDGG-2023-002).” The original article has been corrected.
References
Cha, M. J. et al. Hypersensitivity reactions to iodinated contrast media: A multicenter study of 196 081 patients. Radiology 293 (1), 117–124 (2019).
Wang, L. D. et al. Chinese journal of cerebrovascular diseases (in chinese). Chin. J. Cerebrovasc. Disases. 19 (2), 136–144 (2022).
Harada, Y. et al. Pearls & Oy-sters: Contrast-induced encephalopathy following coronary angiography: A rare stroke mimic. Neurology 94 (23), e2491–e4 (2020).
Chu, Y. T. et al. Contrast-Induced encephalopathy after endovascular thrombectomy for acute ischemic stroke. Stroke 51 (12), 3756–3759 (2020).
Meijer, F. J. A., Steens, S. C. A., Tuladhar, A. M., van Dijk, E. D. & Boogaarts, H. D. Contrast-induced encephalopathy-neuroimaging findings and clinical relevance. Neuroradiology 64 (6), 1265–1268 (2022).
An, J. et al. Differences in adverse reactions among iodinated contrast media: analysis of the KAERS database. J. Allergy Clin. Immunol. Pract. 7 (7), 2205–2211 (2019).
Vogl, T. J., Wessling, J. & Buerke, B. An observational study to evaluate the efficiency and safety of Ioversol pre-filled syringes compared with Ioversol bottles in contrast-enhanced examinations. Acta Radiol. 53 (8), 914–920 (2012).
Chen, Q. L. et al. Retrospective analysis of non-laboratory-based adverse drug reactions induced by intravenous Radiocontrast agents in a joint commission International-accredited academic medical center hospital in China. Ther. Clin. Risk Manag. 13, 565–573 (2017).
van der Molen, A. J., Dekkers, I. A., Bedioune, I. & Darmon-Kern, E. A systematic review of the incidence of hypersensitivity reactions and post-contrast acute kidney injury after Ioversol in more than 57,000 patients: part 1-intravenous administration. Eur. Radiol. 32 (8), 5532–5545 (2022).
Sutton, A. G. et al. Early and late reactions after the use of iopamidol 340, ioxaglate 320, and Iodixanol 320 in cardiac catheterization. Am. Heart J. 141 (4), 677–683 (2001).
Sohn, K. H. et al. Immediate and delayed hypersensitivity after intra-arterial injection of iodinated contrast media: a prospective study in patients with coronary angiography. Eur. Radiol. 29 (10), 5314–5321 (2019).
He, L. B. Z. et al. Incidence and clinical risk factors of contrast⁃induced encephalopathy after percutaneous coronaryintervention (in chinese). Chin. Circ. J. 35 (7), 655–659 (2020).
Li, F. O. Z. J. et al. An initial study on contrastinduced encephalopathy after percutaneous coronary intervention (in chinese). Clin. Cardiol. (China). 33 (6), 518–521 (2017).
Niimi, Y., Kupersmith, M. J., Ahmad, S., Song, J. & Berenstein, A. Cortical blindness, transient and otherwise, associated with detachable coil embolization of intracranial aneurysms. AJNR Am. J. Neuroradiol. 29 (3), 603–607 (2008).
Zhang, G. et al. Contrast-Induced encephalopathy resulting from use of Ioversol and iopromide. Clin. Neuropharmacol. 43 (1), 15–19 (2020).
Zhao, W. et al. Irreversible fatal contrast-induced encephalopathy: a case report. BMC Neurol. 19 (1), 46 (2019).
Muller, F. H. Post-marketing surveillance of the safety profile of Iodixanol in the outpatient CT setting: a prospective, multicenter, observational study of patient risk factors, adverse reactions and preventive measures in 9953 patients. Rofo 186 (11), 1028–1034 (2014).
B SH, A. D. M., C, K. F. S. & E PCG, D. V. M. CONSORT 2010 explanation and elaboration: updated guidelines for reporting parallel group randomised trials. Int. J. Surg. 10 (1), 28–55 (2012).
Media & ACoDaC ACR Manual on Contrast Media (2020).
Whisson, C. C., Wilson, A. J., Evill, C. A. & Sage, M. R. The effect of intracarotid nonionic contrast media on the blood-brain barrier in acute hypertension. AJNR Am. J. Neuroradiol. 15 (1), 95–100 (1994).
Poirier, V. C., Newberry, P. D., Hecht, S. T. & Nemzek, W. R. Phase III clinical trial comparing Iodixanol and Iohexol in cerebral angiography. Acad. Radiol. 3 (Suppl 3), S495–S499 (1996).
Heo, Y. J. et al. Safety and tolerability of Iobitridol in cerebral angiography: a prospective, multicenter study. Acta Radiol. 61 (3), 331–337 (2020).
Wu, T. et al. Cytotoxic effects of nonionic iodinated contrast agent on human Adipose-Derived mesenchymal stem cells. PM R S1934-1482(18), 30294-6. (2018).
Uchiyama, Y. et al. Factors contributing to blood-brain barrier disruption following intracarotid injection of nonionic iodinated contrast medium for cerebral angiography: experimental study in rabbits. Radiat. Med. 24 (5), 321–326 (2006).
Rapoport, S. I., Thompson, H. K. & Bidinger, J. M. Equi-osmolal opening of the blood-brain barrier in the rabbit by different contrast media. Acta Radiol. Diagnosis. 15 (1), 21 (1974).
Jeppsson, P. G. & Olin, T. Neurotoxicity of Roentgen contrast media. Study of the blood-brain barrier in the rabbit following selective injection of contrast media into the internal carotid artery. Acta Radiol. 10 (1), 17–34 (1970).
Rapoport, S. I., Hori, M. & Klatzo, I. Testing of a hypothesis for osmotic opening of the blood-brain barrier. Am. J. Physiol. 223 (2), 323–331 (1972).
Almen, T. Effects of iodixanol, iopentol, Iohexol and Metrizoate on femoral blood flow after injection into the femoral artery of the dog. Acta Radiol. Suppl. 370, 69–72 (1987).
Grynne, B. H., Nossen, J. O., Bolstad, B. & Borch, K. W. Main results of the first comparative clinical studies on Visipaque. Acta Radiol. Suppl. 399, 265–270 (1995).
Palmers, Y., De Greef, D., Grynne, B. H., Smits, J. & Put, E. A double-blind study comparing safety, tolerability and efficacy of Iodixanol 320 mgi/ml and ioxaglate 320 mgi/ml in cerebral arteriography. Eur. J. Radiol. 17 (3), 203–209 (1993).
Zou, W. et al. Iodixanol activation of mast cells: implications in the pathogenesis of iodixanol-induced delayed cutaneous adverse reactions. Toxicology 465, 153034 (2022).
Gharekhanloo, F. & Torabian, S. Comparison of allergic adverse effects and contrast enhancement between Iodixanol and iopromide. Iran. J. Radiol. 9 (2), 63–66 (2012).
Haussler, M. D. Safety and patient comfort with iodixanol: a postmarketing surveillance study in 9515 patients undergoing diagnostic CT examinations. Acta Radiol. 51 (8), 924–933 (2010).
Kopp, A. F. et al. Prevalence of acute reactions to iopromide: postmarketing surveillance study of 74,717 patients. Acta Radiol. 49 (8), 902–911 (2008).
Funding
This research was funded by Key Public Relations Project of the Health and Family Planning Commission of Gansu Province (GSSZD2024-06); Key Talent Project of Gansu Province (2025RCXM068); Major Research Projects of the Gansu Provincial Center Hospital (ZDGG-2023-002).
Author information
Authors and Affiliations
Contributions
The study design was accomplished by Rong Yin and Huisheng Chen.The data collection was accomplished by Aibin Guo, Bin Zhao, Yuanming Li, Yaxuan Wei, Shaoju Shao and Guozhen Zhang.The data analysis was accomplished by Aibin Guo and Zhiqi Yang. The writing the paper was accomplished by Aibin Guo and Zhiqi Yang.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Guo, Ab., Yang, Zq., Zhao, B. et al. Comparison of ioversol and iodixanol related adverse drug reactions in cerebrovascular interventional procedures. Sci Rep 15, 26986 (2025). https://doi.org/10.1038/s41598-025-12048-w
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-12048-w
