
Abstract
The Post-acute Sequela of SARS-CoV-2 (PASC) syndrome, also known as Long-COVID, often presents with subjective symptoms such as brain fog and cognitive fatigue. Increased tinnitus, and decreased hearing in noise ability also occur with PASC, yet whether auditory manifestations of PASC are linked with the cognitive symptoms is not known. Electrophysiology, specifically the Auditory Brainstem Response (ABR), provides objective measures of auditory processing. We hypothesized that ABR findings would be linked to PASC and with subjective feelings of cognitive fatigue. Eighty-two individuals, 37 with PASC (mean age: 47.5, Female: 83%) and 45 healthy controls (mean age: 38.5, Female: 76%), were studied with an auditory test battery that included audiometry and ABR measures. Peripheral hearing thresholds did not differ between groups. The PASC group had a higher prevalence of tinnitus, anxiety, depression, and hearing handicap in addition to increased subjective cognitive fatigue. ABR latency findings showed a significantly greater increase in the wave V latency for PASC subjects when a fast (61.1 clicks/sec) compared to a slow click (21.1 clicks/sec) was used. The increase in latency correlated with cognitive fatigue scores and predicted PASC status. The ABR V/I amplitude ratio was examined as a measure of central gain. Although these ratios were not significantly elevated in the full PASC group, to minimize the cofounding effect of age, the cohort was median split on age. Elevated V/I amplitude ratios were significant predictors of both predicted PASC group classification and cognitive fatigue scores in the younger PASC subjects compared to age-matched controls providing evidence of elevated central gain in younger individuals with PASC. More frequent tinnitus also significantly predicted higher subjective cognitive fatigue scores. Our findings suggest that PASC may alter the central auditory pathway and lead to slower conduction and elevated auditory neurophysiology responses at the midbrain, a pattern associated with the typical aging process. This study marks a significant stride toward establishing an objective measure of subjective cognitive fatigue through assessment of the central auditory system.
Similar content being viewed by others

Introduction
Some individuals with SARS-CoV-2 infection develop a poorly understood post-viral syndrome (Post-Acute Sequelae of SARS-CoV-2 Infection - PASC) that persists for weeks, months, or even years1,2,3,4. Even those with no neurological signs during acute infection can develop “brain fog” often characterized by cognitive fatigue, difficulty concentrating, and problems with memory. These symptoms suggest that PASC may result from central nervous system (CNS) dysfunction from the virus5,6,7,8. Cognitive fatigue is the most common and persistent CNS concern in PASC1,5,9,10, but cognitive fatigue is subjective, difficult to quantify, and not specific to PASC.
CNS dysfunction may be detectable using the auditory system. Behavioral auditory symptoms such as difficulty with auditory discrimination, speech perception in background noise, presence of vertigo, and increases in tinnitus and hyperacusis (heightened sensitivity to sound) are often overlooked manifestations of PASC11,12,13,14,15. Using auditory brainstem responses (ABRs), an electrophysiologic technique, al, Gedik et al.16, found increased III-V interpeak latencies in those with history of COVID-19 infection (not PASC). Ozturk et al.17 found delays in the individual wave I, III and V peaks, among those with a history of COVID-19 but no significant difference in interpeak latencies. Dorobisz et al.18 found delayed latency (i.e., slower conduction time) of ABR waves III and V in those with PASC, as well as delayed I–III and I–V interpeak intervals. These articles focused on damage to the cochlea or peripheral hearing system as measured by the audiogram, OAEs, and the ABR (Wave I). Changes in ABR latencies and amplitudes, however, may also reflect damage to the central hearing system (i.e., the brainstem). Rather than examining only the latencies of individual peaks, effects on nerve function might be revealed better by using differences in Wave V latencies between slow and fast ABR click rates19,20,21. Latencies of ABR waves increase with faster click rates. Diseases that affect nerve transmission, such multiple sclerosis22,23 will lead to greater increases in latency with faster click rates compared to controls. Evidence shows that coronaviruses can be both neuroinvasive and neurovirulent. This could affect nerve conduction, which might be manifest in the differences in wave V latencies between slow and fast click rates.
Also, the ABR peaks, specifically the V/I amplitude ratio, may be useful for looking at changes in central gain24,25. Decreases in the primary inhibitory neurotransmitter, GABA, have been reported in those with PASC26,27,28. Given the link between GABA and central auditory gain, this sets up the possibility of heightened central gain in PASC and associated disruptions to auditory perception. Studies suggest tinnitus, the sensation of sound absent an external stimulus, can arise through abnormal neural gain mechanisms in the central auditory pathway29. Tinnitus, a frequenctly reported PASC symptom, is arguably one of the most prevelant, yet al.so one of the most complex, auditory conditions, often with an undetermined etiology or multifactorial cause30,31. Studies suggest it can arise from changes to the auditory nerve (e.g., microvascular compression or degeneration), and/or CNS dysfunction29,32,33. Gain escalation may emerge at multiple levels of the CNS in response to auditory trauma, hearing loss, or advanced age, leading to an over-application of sound-evoked neural activity in midbrain and cortex as well as disordered auditory percepts25,28,29. Auditory central gain can be quantified objectively and non-invasively using auditory brainstem responses (ABRs), by comparing electrical activity produced by the cochlear nerve (ABR wave I amplitude) to activity in midbrain (ABR wave V amplitude)34,35. Central gain models may explain other auditory disorders, including hyperacusis (i.e., loudness intolerance), which has also been reported with PASC29,36. The ABR profile of tinnitus has been extensively studied37. Several studies have demonstrated that individuals with tinnitus, despite having normal hearing sensitivity, exhibit significantly reduced amplitudes of ABR wave I and often display elevated or at least normal wave V amplitudes compared to control subjects, leading to abnormal V/I ratios indicative of increased central gain33,38,39,40. Central gain models are potentially wide reaching in their explanatory power. They may explain the spectrum of loudness and background noise tolerance observed in healthy young participants41 and age-related sound-evoked changes in midbrain and cortex from decreased central inhibition25.
To explore the link between PASC cognitive symptoms and both latencies and amplitudes on the ABR, we recorded ABRs on participants recruited from a PASC clinic. The focus was on using the increased stimulus repetition rate effects slow-fast wave V latency difference as a measure of diminished nerve function and the wave V/I ratio as a measure of central gain. Demographic information was collected, and hearing questionnaires and peripheral and central auditory tests were performed. The PASC group was compared to controls, who self-reported never having tested positive for COVID-19 or having what they believed to be COVID-19 symptoms. The goal was to examine the ABR for indications of delayed slow-fast latencies and elevated auditory central gain to determine whether the ABR could predict subjective cognitive symptoms in those with PASC.
Materials and methods
Participants
Eighty-two individuals participated in this cross-sectional study, including 37 with PASC (mean age: 47.5, Female: 83%) and 45 healthy controls (mean age: 38.5, Female: 76%) (See Table 1). The age range for all subjects was 18–69 years. All subjects were required to have a documented COVID-19 vaccination before beginning testing. PASC subjects were recruited from local communities in New Hampshire and Vermont, and the dedicated PASC Clinic at Dartmouth-Hitchcock Medical Center. Control subjects were recruited from communities in New Hampshire, Vermont, and Connecticut. Participants recruited from Connecticut were tested at the University of Connecticut, while all other participants were tested at Dartmouth-Hitchcock Medical Center.
Control group eligibility criteria included no history or diagnosis of COVID-19. The PASC group was defined by persistent cognitive fatigue, as determined by a score of > 5.7 on the cognitive fatigue subscale from the Chalder Fatigue Scale, completed at least 2 months after a confirmed COVID-19 diagnosis via PCR (polymerase chain reaction). Exclusionary criteria for both groups were abnormal otoscopy or tympanograms (Type B or C), or a history of significant ear pathology, concussion, significant noise exposure, neurological disease, severe mental illness, or ototoxic antibiotics. The research protocol was approved by the Committee for the Protection of Human Subjects of Dartmouth-Hitchcock Medical Center, Dartmouth College, and the Institutional Review Board of the University of Connecticut and performed in accordance with the Declaration of Helsinki. All research was performed in accordance with relevant guidelines/regulations, and written informed consent was obtained from all participants.
Questionnaires
Subjects completed questionnaires on self-reported hearing ability and general health. Two questions about tinnitus from the National Health and Nutrition Examination Survey (NHANES) were included in the hearing ability questionnaire42. The first asked, “In the past 12 months have you been bothered by ringing, roaring, or buzzing in your ears or head that lasts for 5 minutes or more?” If they answered yes, they were asked how often the symptoms occurred. Self-reported auditory handicap was measured using the Amsterdam Inventory of Auditory Handicap (AIAH)43. Depression and anxiety were measured with the Beck Depression Inventory (BDI-II) and the Beck Anxiety Inventory (BAI), respectively44,45,46. Fatigue was measured using the Chalder Fatigue Scale (CFQ)47. This scale includes separate sub-scales for physical and mental/cognitive fatigue47,48. The CFQ includes items asking about symptoms suggestive of CNS dysfunction such as difficulty concentrating, trouble finding words, and problems with memory. The CFQ asked individuals to compare how they felt now to have they felt prior to contracting COVID-19, with responses measured on a Likert scale and summed. PASC group membership required CFQ scores one standard deviation or more above the mean on the cognitive fatigue subscale (i.e., > 5.7)49. The Neurobehavioral Symptom Inventory (NSI) was also given to assess PASC symptom severity50. In this study we specifically examined the NSI somatosensory (NSI-ss), cognitive (NSI-cog), and affective (NSI-a) factors based on the three-factor, 22-item NSI model described by Caplan, Ivins, Poole, Vanderploeg, Jaffee and Schwab51. For the subscales, somatosensory scores can range from 0 to 40, cognitive scores from 0 to 16, and affective scores from 0 to 28.
Peripheral auditory assessment
Otoscopy and tympanometry were performed on all subjects. Pure tone audiometry was completed with Creare LLC’s hearing test system with Sennheiser HD-200 headphones controlled through a laptop while in a sound booth. Air conduction thresholds were measured with a Békésy-like tracking procedure at octaves from 0.5 to 8 kHz plus the 6-kHz inter-octave. A pure tone average was calculated from 0.5 to 8.0 kHz for each ear.
Auditory brainstem response testing
The ABR was measured using the SmartEP system (Intelligent Hearing Systems). The ABR was collected using a 1-channel electrode array, with an electrode attached to the right earlobe as reference, a ground electrode at Fpz, and an electrode at the high forehead (Fz) as the noninverting electrode. The stimuli were 100-ms rarefaction clicks presented through insert earphones (ER-3As). As the ABR is sensitive to the effect of stimulus rate on neural synchrony, two rates, 21.1/s (slow) or 61.1/s (fast) at 80 dB SPL to the right ear were used to assess the increase in latency that occurs with a higher click rate. A grand mean waveform was also calculated by averaging the two click rates together. Two repetitions of each click rate were recorded and then averaged together (total, 4000 sweeps, 2000 sweeps per rate). Responses were online filtered from 0.1 to 1.5 kHz (second-order Butterworth). Online, recordings were epoched with a -5–12 ms window and averaged. The absolute latencies and amplitudes of waves I, III, and V were measured on the average waveform from the zero-microvolt line as well as from peak to subsequent trough. Rate differences on latency measures were also calculated. Central gain was assessed by measuring the amplitude ratio of wave V to wave I. Peaks to stabilize the V/I ratio were identified by two independent selectors blinded to group membership. A third highly experienced selector adjudicated any discrepancies between selectors.
While the V/I ratio is a common measurement approach in the ABR literature, there are statistical challenges to using ratios that are not often considered in the literature. When Wave I is significantly reduced (close to zero), this produces exceeding high ratios. To address this limitation and stabilize the ratio, a constant was added to the Wave I and Wave V amplitudes before calculating the ratio. Specifically, we added the cohort average amplitude for each peak (wave I – 0.183 mV and wave V – 0.311 mV).
Experimental design and statistical analysis
Efforts to match groups based on age, sex, and hearing ability during targeted recruitment were not fully successful. Consequently, two analysis approaches were used. First, group analysis using all subjects was employed. Second, participants were median divided into two age groups: a younger group aged 18–45 years, and an older group aged 45–69 years (See Table 2). In the younger age range, problems with auditory processing are rare and so any findings in this age group could be particularly noteworthy. A four-group cross-sectional design was used to assess differences in ABR measures between younger and older PASC subjects and their respective control groups. Demographic characteristics of the experimental groups were compared with t-tests for independent groups and a chi-square distribution test for sex and tinnitus prevalence. Primary analyses focused on the difference between ABR variables between PASC and control subjects and within age groups. Logistic and linear mixed effect models explored the relationship between ABR measures and PASC diagnosis as well as subjective cognitive fatigue scores on the Chalder and Neurobehavioral Symptom Inventory using MATLAB 2023b (MathWorks). Mixed-effects models were chosen for two reasons: (1) they can model correlated data, such as repeated measurements of the ABR, which leads to more accurate estimates of model parameters. (2) mixed effect models also require fewer assumptions about the underlying data distribution compared to ANOVA or traditional regression models. Due to the exploratory nature of this study and limited sample size, correction for multiple comparisons was not implemented. Implementing such corrections could potentially increase the risk of Type II errors, where true effects may be falsely dismissed as non-significant. Therefore, to maintain sensitivity and avoid excessive conservatism in our analysis, we have opted to interpret our results without correction for multiple comparisons, with the understanding this may increase the likelihood of Type I errors.
Results
Demographic, hearing thresholds and questionnaire results
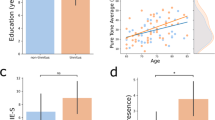
Overall, PASC and controls were matched on sex, education, and peripheral hearing ability (pure tone averages from 0.5 to 8.0 kHz), but showed a clear age difference (Table 1). PASC subjects had higher perceived hearing handicap, as well as higher anxiety, depression, and cognitive fatigue. The PASC subjects were significantly more likely to report tinnitus more than once a week or more frequently. The younger and older groups showed similar education and peripheral hearing ability within groups (Table 2). The older group showed similar sex distribution and age between PASC and controls, however, the younger PASC group showed slightly higher female percentage and older age compared to the younger controls. Compared to controls, younger PASC subjects were significantly more likely to report frequent tinnitus. While we did not directly ask about the difference in tinnitus symptoms before and after COVID-19 infection, multiple subjects spontaneously reported their tinnitus was more noticeable after diagnosis or the subjective perception began since diagnosis (14/37 all PASC subjects). No control subject reported constant tinnitus perception (i.e., “Always”), while 30% of the PASC subjects reported constant tinnitus (Supplemental Fig. 1). Within the age subgroups, the older PASC group had the largest percentage of constant tinnitus (Supplemental Fig. 2).
On mood measures, the PASC group had significantly higher levels of depression, anxiety, and negative affect compared to controls (all p < .001). Supplemental Figs. 3 and 4 shows box plots of questionnaire results for the entire cohort and subgroup analysis respectively. Somatosensory complaints (NSI-ss) were also higher in the PASC group (p < .001). Subjective cognitive fatigue (CFQ) and subjective cognitive functioning (NSI-cog) was also significantly higher in the PASC group compared to controls (all p < .001). In the subgroup analysis, all PASC groups showed higher levels of depression, anxiety, and negative affect compared to controls (all p < .002). While the CFQ was expected to be higher in those with PASC (i.e., part of inclusion criteria), the NSI further supported the presence of subjective cognitive concerns such as poor concentration, slowed thinking, forgetfulness, and difficultly with decision making. Notably, the PASC group also reported higher subjective hearing handicap (AIAH) as compared to controls in the overall cohort (p = .011) and the older subgroup analysis (p = .011), but not the younger group (p = .155).
ABR results—entire cohort
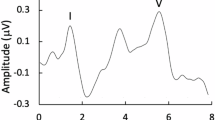
Grand mean waveforms and the fast and slow click rates for the overall cohort are plotted in Fig. 1. Two main findings revealed differences in wave I amplitude and wave V latency between PASC and controls. Although the data showed a trend toward amplitude differences between groups on multiple peaks, the PASC and controls groups differed only on wave I amplitude in the grand mean (p = .011) and using the fast click rate (p = .006) with controls having larger amplitudes (Supplementary Table 1). The V/I amplitude ratio was not different between PASC and controls (p = .144). While wave I amplitude differences were likely due to the age disparity between groups, a larger wave V latency difference between slow and fast click rate was observed for PASC subjects (p = .042).

ABR Grand Mean Waveforms for PASC and Control Subjects – The top panel shows the averaged grand mean waveforms for both PASC and control subjects. Control subjects are plotted with a black line while PASC patients are plotted in red. The bottom two panels show the slow click rate (right – 21.1 per second) and fast click rate (left – 61.1 per second). Shading represents +1 standard deviation. Waves I and V are outlined with dashed rectangles.
Figure 2 shows a plot of ABR V/I ratio across age collapsed across click rate. The controls show a gradual increase in V/I ratio with age; a second order polynomial using the least absolute residuals was determined as best fit for the control group. This best fit line was used as the basis for analyzing the PASC group. For the PASC subjects, we calculated how many subjects in each group were above and below the line of best fit. Although PASC subjects were more likely to be above the line (60%), Fisher’s Exact test showed no difference in V/I ratio across the age range (p = .144).

Age vs. ABR V/I Ratio. The solid black line is a second order polynomial fit using least absolute residuals to control subjects (blue dots). Dotted lines above and below the line of best fit represent the upper and lower bounds of the polynomial fit. PASC subjects (red dots) were then overlayed.
ABR results—age subgroup analysis
In the subgroup analysis, both cohorts showed clear morphology, but the younger adults displayed larger amplitude peaks (Fig. 3). Wave I amplitude and the V/I amplitude ratio were significantly larger in the grand mean waveforms in younger controls than younger PASC (p = .001 and p = .003, respectively - Supplementary Table 2). Wave III and I-V interpeak latencies were also significantly different, but the younger PASC group had earlier latencies compared to controls (p = .048 and 0.034, respectively – Supplementary Table 2). The older PASC and controls did not differ on any peak measure.

ABR Grand Mean Waveforms for Younger and Older Subgroups—The left panel shows the averaged grand mean waveforms (averaged across click rate) for younger PASC and control subjects and the left panel shows the older subjects. Control subjects are plotted with a black line while PASC patients are plotted in red. Shading represents +1 standard deviation. Waves I and V are outlined with dashed rectangles.
Figure 3, when divided by age subgroup, shows 80% (12/15) of the younger PASC group had V/I amplitude ratios above the fitted line compared to 48% (13/27) of the younger controls. However, using Fisher’s Exact test, we found that younger PASC subjects were not significantly (p = .056) more likely to have a larger V/I ratio (i.e., above the line) compared to young controls. While older PASC and control subjects had higher V/I ratios compared to younger subjects, there were no differences between V/I amplitude ratios between groups.
ABR relationship to group and cognitive fatigue
To assess how ABR measures related to group membership and reported cognitive fatigue on the CFQ and NSI, mixed effect models focused on using wave V latency difference in the entire cohort and V/I amplitude ratio in the subgroup analysis (Table 3). In the entire cohort wave V latency difference predicted PASC group membership (p = .036), CFQ (p = .004), and NSI (p = 004) cognitive fatigue. Tinnitus perception also predicted CFQ (p = .012), and NSI (p = .015), but not PASC group membership (p = .054).
In the age subgroups, higher ABR wave V/I amplitude significantly predicted PASC group membership (p = .018), and CFQ (p = .029), but its association with NSI scores (p = .132) was not significant for the young subgroup (Table 3). For the older group no association between cognitive fatigue or PASC group membership and V/I ratio was observed (all p > .364). Tinnitus perception was also a significant predictor of CFQ and NSI scores (p = .004 and p = .005, respectively) in the young subgroup. That is, frequent tinnitus perception predicted higher cognitive fatigue scores on two independent questionnaires in the entire cohort and the younger subgroup.
To understand which ABR components were driving the V/I amplitude ratio effects, wave I and V amplitude were plotted separately across age (Fig. 4). Using a linear fit to the data, wave I showed similar decreasing trajectory of amplitude with increased age for both PASC and controls in the entire cohort. The wave V fit, however, shows a greater slope for the PASC group with higher wave V amplitudes for younger ages. This finding was contrary to results of the individual peak measures that showed significant differences in wave I and no differences between wave V in the overall cohort and in the younger subgroup. Therefore, an analysis was conducted to assess the difference between PASC and controls on waves I and V in the two subgroups. While the older subgroup showed complex trajectories, the younger subgroup displayed lower wave I and higher wave V amplitudes. Interestingly, the younger PASC subjects who experienced tinnitus most frequently were observed to have the lower wave I amplitudes. Linear mixed effect models were then conducted to assess the effect of age, tinnitus, and PASC group membership on waves I and V amplitude. The overall model showed that the PASC group had higher wave V amplitudes, and age reduced wave I in all subjects, but the interaction between age and PASC group showed no significant effect even on wave V (p = .051). Individual subgroup analysis showed younger PASC subjects had smaller wave I amplitude (p = .044) and those with higher perceived tinnitus had smaller wave V amplitude (p = .008). In the older subgroup, age was a strong predictor of wave I amplitude (p = .009), but no other significant effects were found for wave V. Taken together, this is consistent with smaller wave I amplitude in younger PASC and an undefined effect of PASC and tinnitus on wave V.

Amplitude of Waves I and V for Entire Cohort and Age Subgroups. The top panel shows amplitude of wave I (top left panel) and wave V (top right panel) for PASC (red) and Controls (blue). A linear fit is also plot for both groups. The size of the individual datapoints represents the perceived tinnitus of the subject. Larger dots equate to more frequently perceived tinnitus. The bottom four panels show waves I and V for the younger and older group respectively.
Discussion
This study investigated the link between PASC cognitive symptoms and objective auditory electrophysiology in patients with and without PASC. Compared to controls, PASC subjects showed an increased prevalence of tinnitus and more perceived hearing handicaps despite matched peripheral hearing ability, in addition to increased cognitive fatigue, anxiety, and depression. ABR wave V latency differences between the slow and fast click rate revealed larger differences in the PASC group, similar to previous work in MS23. Increased stimulus repetition rate effects on wave V latency also predicted PASC membership and subjective cognitive fatigue on both the CFQ and NSI. When divided into younger and older ages, tinnitus prevalence was increased in younger PASC subjects, while older PASC subjects had more perceived hearing handicap compared to age-matched controls. ABR showed reduced wave I amplitude and heightened ABR wave V/I ratios in younger PASC subjects. While older adults showed an overall increase in the V/I amplitude ratio due to age, no differences were found between PASC and controls. Moreover, tinnitus perception and V/I amplitude ratio, a measure of central gain, predicted younger PASC group membership, degree of subjective cognitive fatigue on the CFQ, with greater gain associated with greater fatigue.
To date, biological indices of subjective fatigue have been elusive. Interesting findings to emerge from this study were that ABR slow-fast latency rate differences predicted subjective cognitive fatigue and younger PASC subjects show signs of elevated central gain, similar to what was observed in older adults. The reduction of wave I amplitude in the younger group could potentially suggest a subclinical dysfunction to the cochlea or auditory nerve. Together, young adults may be more susceptible than older adults to adverse effects of COVID-19 on central auditory processing, or that the changes may be more difficult to detect with aging52.
This study and others suggest that COVID-19 may have long-lasting effects on the CNS. Our study aligns with other’s showing significant effects on wave latencies compared to controls, indicating potential brainstem dysfunction16,17,53. This supports the hypothesis that persistent brainstem dysfunction may contribute to PASC, given the brainstem’s vulnerability to SARS-CoV-2 infection and its role in regulating various physiological processes54. Subtle delays in neural transmission within the brainstem could have severe downstream consequences. Some COVID-19 cases exhibit demyelinating features, with symptoms resembling acute disseminated encephalomyelitis55. As neurons do not readily regenerate, neural transmission dysfunction in the brainstem dysfunction may be long-lasting and has been implicated in other similar disorders, such as chronic pain, migraine and chronic fatigue syndrome56,57. Our latency results also match rate-based effects seen in those with MS, another population that is affected by cognitive fatigue58,59. Robinson and Rudge60 were the first to report ABR wave V latency and amplitude changes in MS with increasing click rate. Since then, studies have found that increasing ABR stimulus rates can improve the detection of abnormalities in MS patients23. Interestingly, the results of our study were not evident in the faster rate (61.1), but in the difference between the rates, indicating earlier slow rate latencies and delayed faster rate latencies. This effect was independent of age, which is consistent with the literature showing remarkably similar rate effects in young and older adults when peripheral hearing ability is normal in both age groups19. Importantly, this latency result predicted cognitive fatigue on two independent measures in PASC patients. While the exact mechanisms of PASC neurotropism and neuropathogenesis are still under investigation, the potential for both acute and long-term neurological consequences is a growing concern. Objective auditory electrophysiological evidence of CNS dysfunction linked to cognitive fatigue could serve as a valuable marker for PASC and other populations experiencing cognitive fatigue though further research is needed to confirm and expand on these findings.
Previous work has also shown that gain enhancement may emerge concurrently at multiple levels of the CNS in response to auditory dysfunction or trauma, leading to increased sound-evoked neural activity in midbrain and cortex and disordered auditory perceptions, such as tinnitus29. In studies of patients with tinnitus, elevated amplitudes, specifically the wave V/I ratio, have been thought to reflect overactivity in the central pathway extending from ventral cochlear nucleus to inferior colliculus38, this overactivity being associated with cochlear neural degeneration in many, but not all, reports61. In the case of our PASC subjects, heightened central gain may be a consequence of disruptions to the cochlea or cochlear nerve, as wave I amplitude was significantly smaller in PASC subjects, particularly those younger then 45 years. Also, wave V could be contributing to larger V/I ratios in PASC, suggesting increased sound-evoked activity in inferior colliculus. Nonetheless, wave V amplitude independently predicted group membership in the overall cohort, while wave I amplitude was predictive in the younger PASC subgroup. However, neither wave amplitude was predictive of PASC in the older subgroup. Notably, the younger and older groups did not differ on other dimensions of the ABR, including peak and inter-peak latencies, suggesting that heightened gain is not comorbid with deficient synaptic transmission.
What might then be the mechanistic underpinning of heightened central gain in younger PASC patients? Although not directly measured in the current study, decreased GABA could be a driving force behind the wave V/I ratio results. GABA, the primary inhibitory neurotransmitter in the central auditory system, maintains the balance of neural excitation and inhibition62. Relevant to the COVID-19 virus, GABA also plays a role in modulating inflammatory autoimmune responses63. Decreased GABA has been associated with a panoply of physiological and pathophysiological neurological conditions and has been reported in PASC64,65. Insufficient inhibition due to lower GABA concentrations, altered GABA distribution within the auditory system, or altered receptor density or GABA affinity could explain, and potentially link, the tinnitus and ABR findings in this population66. Altered GABA is not necessarily specific to the auditory system in PASC; altered GABA could be more systemic and even potentially underlie depressive and anxiety symptoms67, which were also elevated in the PASC group.
In this study, results from the ABR, an obligatory electrophysiological measure that does not require attention to the stimulus, were related to subjective cognitive fatigue on the Chalder Fatigue Scale. These results suggest central auditory involvement in PASC and highlight that ABRs could offer an objective correlate of cognitive fatigue. This symptom currently can only be assessed using subjective measures. Auditory tests are particularly relevant in assessing cognitive fatigue because sound engages cognitive processes related to perception, attention, and memory68,69. Studies of patients with chronic fatigue syndrome70,71 have shown increased neural resource allocation when processing complex auditory information compared to demographically similar healthy adults72. The same may be true in PASC. Delayed neural conduction time and increased central gain in the midbrain could give rise to functional cortical processing disparities in PASC. Therefore, ABRs could serve as an objective indicator of upstream cortical dysfunction73,74,75. Future research should study later auditory evoked potentials and fMRI, and simulate real-world communication environments, to further clarify these findings within this population.
While latency results were found in the entire cohort, a wide age range (18–69) prompted additional analysis on age subgroups. ABR V/I amplitude ratio clearly showed an increasing trend with advanced age. Age-related changes in the auditory midbrain and cortex from decreased central inhibition are well-described literature25,76 and are evident in our dataset as well, where we see a decrease in wave I with age and corresponding trend for increasing V/I amplitude with age (regardless of group). Thus, with the aging process, there is a natural deterioration of cochlear output with age (i.e., presbycusis) that leads to a hypothesized increase in central gain25,28. The observed increased latency of wave V due to a rapid click rate is likely not attributable to an age-related effect19, opening a new avenue for further investigation. Nonetheless, the V/I ratio increase in the PASC groups, particularly the younger subjects, potentially exceeds central changes that are expected to occur with natural aging. Indeed, in the PASC group, the younger subjects patterned similarly to the older subjects for wave V/I ratio and in wave I reduction. In alignment with this, the relationship between the V/I ratio and Chalder score was reduced with increasing age. This could suggest a form of accelerated central auditory aging in COVID-19 77,78; future longitudinal studies need to assess the progression of central gain with biological aging in patients who develop PASC at younger vs. older ages.
Interestingly, frequent tinnitus significantly predicted CFQ scores, and tinnitus also independently predicted cognitive scores from a subset of the NSI in the entire cohort. However, the younger PASC group seemed to drive this effect (i.e., no tinnitus result in the older subgroup) with more frequent tinnitus related to heightened central gain but simultaneously related to smaller ABR wave V amplitude. This supports the hypothesized link between central gain and tinnitus, although in this cross-sectional study it is not possible to know how the wave V/I ratio might have changed with COVID in a given individual and whether this change was related to tinnitus severity or development. An intuitive explanation for the causation of tinnitus is that a reduction in auditory input, typically due to hearing loss or cochlear damage, leads to increased gain in the central auditory pathways79,80,81. In other words, auditory neurons that receive reduced input at lower levels compensate by amplifying their response to maintain their baseline activity level at higher level. Like our younger subgroup, several studies have demonstrated that subjects with tinnitus and normal hearing sensitivity show significantly reduced ABR wave I amplitudes and elevated or at least normal wave V amplitudes compared with control subjects, suggesting increased central auditory gain38,40. Indeed, studies have shown possible cochlear neural degeneration in normal-hearing individuals with tinnitus with reduced wave I amplitudes and smaller action potential amplitudes using electrocochleography33,40,82. Vasilkov et al. showed tinnitus status was a significant predictor of ABR wave I, even after controlling for factors such as sex, auditory thresholds, and concussion history. But there are mixed findings in the literature on ABRs and the V/I ratio in those with tinnitus24,25,79,80,81,83. Tinnitus symptoms are also known to vary as a function of mental health84 and environmental conditions85,86. Thus, it could be that increased fatigue leads to increased social isolation, greater time in quiet environments, and an unmasking of tinnitus symptoms previously unobserved by the person. The degree to which some of the reported group differences predate PASC is unknown as data on tinnitus, depression, anxiety, hearing handicap, and hearing thresholds prior to contracting PASC in our sample were not available. Additionally, the tinnitus questionnaire used in this study lacked the depth and specificity of other validated measures, such as the Tinnitus Handicap Inventory (THI)87. As a result, the subjective perceptions reported in this study may not fully capture or accurately reflect a true tinnitus percept or how tinnitus impacts someone’s social emotional well-being. Another limitation is the lack of extended high-frequency thresholds. Studies have clearly demonstrated that extended high-frequency hearing loss is prevalent among individuals with tinnitus88,89 and could be contributing to PASC group results. The small sample size and not adjusting for multiple comparisons also hinder generalizability and increases the likelihood of falsely identifying significant effects. Another limitation is that our healthy controls were also defined from self-report of cognitive fatigue and absent symptoms of COVID-19 infection. Controls could have had asymptomatic infections; also, as subjects were required to be vaccinated to participate in the study, it was not possible to use PCR to confirm that controls had never had COVID-19. Increased tinnitus perception following the SARS-CoV-2 vaccine90 cannot be ruled out. Data collection took place in 2021–2022 at a point in the pandemic when it became increasingly difficult to find individuals who had never had COVID-19; thus, we cannot rule out that the individuals in the control group have other characteristics that differentiate them from those who contracted the illness.
Conclusions
Compared to controls, PASC subjects showed an increased prevalence of tinnitus, more perceived hearing handicap, and increased slow-fast wave V latency difference for the two stimulus rates. When separated into younger and older age ranges, increased ABR wave V/I ratios were found in only the younger PASC subjects. Increased stimulus repetition rate effects on wave V latency and wave V/I amplitude ratio predicted PASC group membership and subjective cognitive fatigue on the Chalder Fatigue Scale. These findings indicate abnormal central auditory processing in individuals with PASC, particularly notable in those under 45 years old, where such effects are typically unexpected. These results also suggest central auditory involvement determined using auditory electrophysiology in PASC could offer an objective correlate of subjective cognitive fatigue, but additional testing is needed to confirm the use of this methodology.
Data availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
References
Moghimi, N. et al. The neurological manifestations of post-acute sequelae of SARS-CoV-2 infection. Curr. Neurol. Neurosci. Rep. 21, 1–17 (2021).
Parker, A. M. et al. Addressing the post-acute sequelae of SARS-CoV-2 infection: A multidisciplinary model of care. Lancet Respiratory Med. 9 (11), 1328–1341 (2021).
Vehar, S., Boushra, M., Ntiamoah, P. & Biehl, M. Post-acute sequelae of SARS-CoV-2 infection: Caring for the ‘long-haulers’. Cleve Clin. J. Med. 88 (5), 267–272 (2021).
Sudre, C. H. et al. Attributes and predictors of long COVID. Nat. Med. 27 (4), 626–631 (2021).
Carfì, A., Bernabei, R. & Landi, F. Persistent symptoms in patients after acute COVID-19. Jama 324 (6), 603–605 (2020).
Islam, M. F., Cotler, J. & Jason, L. A. Post-viral fatigue and COVID-19: Lessons from past epidemics. Fatigue Biomed. Health Behav. 8 (2), 61–69. https://doi.org/10.1080/21641846.2020.1778227 (2020).
Wu, Y. et al. Nervous system involvement after infection with COVID-19 and other coronaviruses. Brain. Behav. Immun. 87, 18–22 (2020).
Khateb, M., Bosak, N. & Muqary, M. Coronaviruses and central nervous system manifestations. Front. Neurol. 11doi https://doi.org/10.3389/fneur.2020.00715 (2020).
Haider, H. F. & Szczepek, A. J. Neurotological consequences of long COVID. Front. Neurol. 13, 1087896 (2022).
Junior, G. Z. et al. Neurologic and neuropsychiatric symptoms in long-COVID 19 syndrome: A systematic review (Research Square Platform LLC, 2022).
Wu, Y. et al. Nervous system involvement after infection with COVID-19 and other coronaviruses. Brain Behav. Immun.. 87, 18–22. https://doi.org/10.1016/j.bbi.2020.03.031 (2020).
Alves de Sousa, F., Costa, R., Xará, S., Pinto, A. & Almeida, E. S. SARS-CoV-2 and hearing: An audiometric analysis of COVID-19 hospitalized patients. J. Otol.(2021).
Verma, H., Shah, J., Akhilesh, K. & Shukla, B. Patients’ perspective about speech, swallowing and hearing status post-SARS-CoV-2 (COVID-19) recovery: E-survey. Eur. Arch. Otorhinolaryngol. 279 (5), 2523–2532. https://doi.org/10.1007/s00405-021-07217-2 (2022).
Almishaal, A. A. & Alrushaidan, A. A. Short- and long-term self-reported audiovestibular symptoms of SARS-CoV-2 infection in hospitalized and nonhospitalized patients. Audiol. Neurotol. 1–15. (2022).
De Luca, P. et al. Long COVID, audiovestibular symptoms and persistent chemosensory dysfunction: A systematic review of the current evidence. Acta Otorhinolaryngol. Ital. 42, S87–S93 (2022).
Gedik, Ö., Hüsam, H., Başöz, M., Tas, N. & Aksoy, F. The effect of coronavirus disease 2019 on the hearing system. J. Laryngol. Otol. 135 (9), 810–814. https://doi.org/10.1017/s0022215121001961 (2021).
Öztürk, B., Kavruk, H. & Aykul, A. Audiological findings in individuals diagnosed with COVID-19. Am. J. Otolaryngol. 43 (3), 103428 (2022).
Dorobisz, K., Pazdro-Zastawny, K., Misiak, P., Kruk-Krzemień, A. & Zatoński, T. Sensorineural hearing loss in patients with Long-COVID-19: Objective and behavioral audiometric findings. Infect. Drug Resist. 16, 1931–1939 (2023).
Burkard, R. F. & Sims, D. The human auditory brainstem response to high click rates. (2001).
Don, M., Allen, A. R. & Starr, A. Effect of click rate on the latency of auditory brain stem responses in humans. Ann. Otol. Rhinol. Laryngol. 86 (2), 186–195 (1977).
Yagi, T. & Kaga, K. The effect of the click repetition rate on the latency of the auditory evoked brain stem response and its clinical use for a neurological diagnosis. Arch. Oto-Rhino-Laryngol. 222 (2), 91–97. https://doi.org/10.1007/bf00469746 (1979).
Paludetti, G., Maurizi, M. & Ottaviani, F. Effects of stimulus repetition rate on the auditory brain stem responses (ABR). Otol. Neurotol. 4 (3), 226–234 (1983).
Jacobson, J. T., Murray, T. & Deppe, U. The effects of ABR stimulus repetition rate in multiple sclerosis. Ear Hear. 8 (2), 115–120 (1987).
Johannesen, P. T. & Lopez-Poveda, E. A. Age-related central gain compensation for reduced auditory nerve output for people with normal audiograms, with and without tinnitus. Iscience 24(6) (2021).
Rumschlag, J. A. et al., Age-related central gain with degraded neural synchrony in the auditory brainstem of mice and humans. Neurobiol. Aging. 115, 50–59. https://doi.org/10.1016/j.neurobiolaging.2022.03.014 (2022).
White, K. R., Forsman, I., Eichwald, J. & Munoz, K. Apr. The evolution of early hearing detection and intervention programs in the United States. Seminars Perinatol. 34 (2), 170–179 (2010). https://doi.org/10.1053/j.semperi.2009.12.009
Caspary, D. M., Milbrandt, J. C. & Helfert, R. H. Central auditory aging: GABA changes in the inferior colliculus. Exp. Gerontol. 30 (3–4), 349–360 (1995).
Harris, K. C. et al. Afferent loss, GABA, and central gain in older adults: Associations with speech recognition in noise. J. Neurosci. 42 (38), 7201–7212. https://doi.org/10.1523/jneurosci.0242-22.2022 (2022).
Auerbach, B. D., Rodrigues, P. V. & Salvi, R. J. Central gain control in tinnitus and hyperacusis. Rev. Front. Neurol.. 24 (206) (2014). https://doi.org/10.3389/fneur.2014.00206 (2014).
Roberts, L. E. & Salvi, R. Overview Hearing Loss, Tinnitus, Hyperacusis, and the Role of Central Gain, p. 1–7 (Elsevier, 2019).
Baguley, D., McFerran, D., Hall, D. & Tinnitus Lancet 382 (9904), 1600–1607 (2013).
Shulman, A., Goldstein, B. & Strashun, A. M. Central nervous system neurodegeneration and tinnitus: A clinical experience. Int. Tinnitus J. 13, 118–131 (2007).
Vasilkov, V. et al. Evidence of cochlear neural degeneration in normal-hearing subjects with tinnitus. Sci. Rep. 13 (1). https://doi.org/10.1038/s41598-023-46741-5 (2023).
Auerbach, B. D., Radziwon, K. & Salvi, R. Testing the central gain model: Loudness growth correlates with central auditory gain enhancement in a rodent model of hyperacusis. Neurosci. 21, 407:93–107. https://doi.org/10.1016/j.neuroscience.2018.09.036 (2019).
Valderrama, J. T. et al. Effects of lifetime noise exposure on the middle-age human auditory brainstem response, tinnitus and speech-in-noise intelligibility. Hear. Res. 365, 36–48. https://doi.org/10.1016/j.heares.2018.06.003 (2018). 2018/08/01/.
Gu, J. W., Halpin, C. F., Nam, E-C., Levine, R. A. & Melcher, J. R. Tinnitus, diminished sound-level tolerance, and elevated auditory activity in humans with clinically normal hearing sensitivity. J. Neurophysiol. (2010).
Milloy, V., Fournier, P., Benoit, D., Noreña, A. & Koravand, A. Auditory brainstem responses in tinnitus: A review of who, how, and what? Front. Aging Neurosci. 9, 237 (2017).
Gu, J. W., Herrmann, B. S., Levine, R. A. & Melcher, J. R. Brainstem auditory evoked potentials suggest a role for the ventral cochlear nucleus in tinnitus. J. Assoc. Res. Otolaryngol. 13 (6), 819–833. https://doi.org/10.1007/s10162-012-0344-1 (2012).
Bramhall, N. F., Konrad-Martin, D. & McMillan, G. P. Tinnitus and auditory perception after a history of noise exposure: Relationship to auditory brainstem response measures. Ear Hear. 39 (5), 881–894. https://doi.org/10.1097/aud.0000000000000544 (2018).
Schaette, R. & McAlpine, D. Tinnitus with a normal audiogram: Physiological evidence for hidden hearing loss and computational model. J. Neurosci. Off. J. Soc. Neurosci. 21 (38), 13452–13457. https://doi.org/10.1523/jneurosci.2156-11.2011 (2011).
Tampas, J. W. & Harkrider, A. W. Auditory evoked potentials in females with high and low acceptance of background noise when listening to speech. J. Acoust. Soc. Am. 119 (3), 1548–1561 (2006).
Shargorodsky, J., Curhan, G. C. & Farwell, W. R. Prevalence and characteristics of tinnitus among US adults. Am. J. Med. 123 (8), 711–718 (2010).
Kramer, S. E., Kapteyn, T. S., Festen, J. M. & Tobi, H. Factors in subjective hearing disability. Audiol.. 34 (6), 311–320 (1995).
Beck, A. T., Steer, R. A. & Brown, G. K. Beck depression inventory. San Antonio TX (1987).
Beck, A. T., Epstein, N., Brown, G. & Steer, R. Beck anxiety inventory. J. Consult. Clin. Psychol. (1993).
Beck, A. T., Steer, R. A. & Brown, G. K. BDI-II, Beck Depression Inventory 2nd edn vi (Psychological Corp, 1996).
Chalder, T. et al. Development of a fatigue scale. J. Psychosom. Res. 37 (2), 147–153. https://doi.org/10.1016/0022-3999(93)90081-p (1993).
Cella, M. & Chalder, T. Measuring fatigue in clinical and community settings. J. Psychosom. Res. 69 (1), 17–22. https://doi.org/10.1016/j.jpsychores.2009.10.007 (2010).
Loge, J. H., Ekeberg, O. & Kaasa, S. Fatigue in the general Norwegian population: Normative data and associations. J. Psychosom. Res. 45 (1), 53–65. https://doi.org/10.1016/s0022-3999(97)00291-2 (1998).
Cicerone, K. D. & Kalmar, K. Persistent postconcussion syndrome: The structure of subjective complaints after mild traumatic brain injury. J. Head Trauma Rehabil. 10 (3), 1–17 (1995).
Caplan, L. J. et al. The structure of postconcussive symptoms in 3 US military samples. J. Head Trauma Rehabil. 25 (6), 447–458 (2010).
Liberman, M. C. & Kujawa, S. G. Cochlear synaptopathy in acquired sensorineural hearing loss: Manifestations and mechanisms. Hear. Res. Jun. 349, 138–147. https://doi.org/10.1016/j.heares.2017.01.003 (2017).
Hamdy, M. M., Hosny, N. A., Farag, R. G. & Elbohy, Z. M. Y. Assessment of cortical evoked potential (P300) and auditory brainstem response (ABR) in post-COVID-19 patients. Egypt. J. Otolaryngol. 40 (1). https://doi.org/10.1186/s43163-024-00612-6 (2024).
Yong, S. J. Persistent brainstem dysfunction in Long-COVID: A hypothesis. ACS Chem. Neurosci.. 17 (4), 573–580. https://doi.org/10.1021/acschemneuro.0c00793 (2021).
Reichard, R. R. et al. Neuropathology of COVID-19: A spectrum of vascular and acute disseminated encephalomyelitis (ADEM)-like pathology. Acta Neuropathol. 140, 1–6 (2020).
Yong, S. J. Persistent brainstem dysfunction in long-COVID: A hypothesis. ACS Chem. Neurosci. 12 (4), 573–580 (2021).
Yong, S. J. Long COVID or post-COVID-19 syndrome: Putative pathophysiology, risk factors, and treatments. Infect. Dis. 53 (10), 737–754 (2021).
DeLuca, J., Genova, H. M., Hillary, F. G. & Wylie, G. Neural correlates of cognitive fatigue in multiple sclerosis using functional MRI. J. Neurol. Sci. 270 (1–2), 28–39 (2008).
Krupp, L. B. & Elkins, L. E. Fatigue and declines in cognitive functioning in multiple sclerosis. Neurology 55 (7), 934–939 (2000).
Robinson, K. & Rudge, P. The stability of the auditory evoked potentials in normal man and patients with multiple sclerosis. J. Neurol. Sci. 36 (1), 147–156 (1978).
Vasilkov, V. et al. Evidence of cochlear neural degeneration in normal-hearing subjects with tinnitus. Sci. Rep. 13 (1), 19870 (2023).
Kaltenbach, J. A. Tinnitus: models and mechanisms. Hear. Res. 276 (1–2), 52–60 (2011).
Bhat, R. et al. Inhibitory role for GABA in autoimmune inflammation. Proc. Natl. Acad. Sci. 107 (6), 2580–2585 (2010).
Versace, V. et al. Intracortical GABAergic dysfunction in patients with fatigue and dysexecutive syndrome after COVID-19. Clin. Neurophysiol. 132 (5), 1138–1143 (2021).
Marinkovic, K. et al. Cortical GABA levels are reduced in post-Acute COVID-19 syndrome. Brain Sci. 13 (12), 1666 (2023).
Isler, B. et al. Lower glutamate and GABA levels in auditory cortex of tinnitus patients: A 2D-JPRESS MR spectroscopy study. Sci. Rep. 12 (1). https://doi.org/10.1038/s41598-022-07835-8 (2022).
Petty, F. GABA and mood disorders: A brief review and hypothesis. J. Affect. Disord. 34 (4), 275–281 (1995).
Baldwin, C. L. Auditory Cognition and Human Performance: Research and Applications (CRC, 2012).
Pichora-Fuller, M. K. et al. Hearing impairment and cognitive energy: The framework for Understanding effortful listening (FUEL). Ear Hear. 37 (1), 5S–27S. https://doi.org/10.1097/aud.0000000000000312 (2016).
Chaudhuri, A. & Behan, P. O. Fatigue and basal ganglia. J. Neurol. Sci. 179 (1–2), 34–42 (2000).
Chaudhuri, A. & Behan, P. O. Fatigue in neurological disorders. Lancet 363 (9413), 978–988 (2004).
Lange, G. et al. Objective evidence of cognitive complaints in chronic fatigue syndrome: A BOLD fMRI study of verbal working memory. NeuroImage 26, 513–524 (2005).
Stockard, J. J. & Rossiter, V. S. Clinical and pathologic correlates of brain stem auditory response abnormalities. Neurology 27 (4), 316–316 (1977).
Kamerer, A. M. et al. The role of cognition in common measures of peripheral synaptopathy and hidden hearing loss. Am. J. Audiol. 28 (4), 843–856 (2019).
Allen, P. & Allan, C. Auditory processing disorders: Relationship to cognitive processes and underlying auditory neural integrity. Int. J. Pediatr. Otorhinolaryngol. 78 (2), 198–208 (2014).
Caspary, D. M., Ling, L., Turner, J. G. & Hughes, L. F. Inhibitory neurotransmission, plasticity and aging in the mammalian central auditory system. J. Exp. Biol. 211 (11), 1781–1791 (2008).
Sivagurunathan, N. & Calivarathan, L. SARS-CoV-2 infection to premature neuronal aging and neurodegenerative diseases: Is there any connection with hypoxia? CNS Neurol. Disord Drug Targets. 23 (4), 431–448. https://doi.org/10.2174/1871527322666230418114446 (2024).
Petersen, M. et al., Brain imaging and neuropsychological assessment of individuals recovered from a mild to moderate SARS-CoV-2 infection. Proc. Natl. Acad. Sci. 120 (22)https://doi.org/10.1073/pnas.2217232120 (2023).
Auerbach, B. D., Rodrigues, P. V. & Salvi, R. J. Central gain control in tinnitus and hyperacusis. Front. Neurol. 5. https://doi.org/10.3389/fneur.2014.00206 (2014).
Noreña, A. J. An integrative model of tinnitus based on a central gain controlling neural sensitivity. Neurosci. Biobehav. Rev. 35 (5), 1089–1109 (2011).
Sedley, W. Tinnitus: Does gain explain? Neuroscience 407, 213–228 (2019).
Ting, K-C., Chang, C-C., Huang, C-Y., Chen, Y-F. & Cheng, Y-F. Are electrocochleographic changes an early sign of cochlear synaptopathy? A prospective study in tinnitus patients with normal hearing. Diagnostics 12 (4), 802. https://doi.org/10.3390/diagnostics12040802 (2022).
Shim, H. J., An, Y. H., Kim, D. H., Yoon, J. E. & Yoon, J. H. Comparisons of auditory brainstem response and sound level tolerance in tinnitus ears and non-tinnitus ears in unilateral tinnitus patients with normal audiograms. PLoS ONE. 12 (12), e0189157. https://doi.org/10.1371/journal.pone.0189157 (2017).
Hackenberg, B. et al. Tinnitus and its relation to depression, anxiety, and stress—a population-based cohort study. J. Clin. Med. 12 (3), 1169 (2023).
Searchfield, G. D. Tinnitus what and where: An ecological framework. Front. Neurol. 5, 122255 (2014).
Colagrosso, E. M., Fournier, P., Fitzpatrick, E. M. & Hébert, S. A qualitative study on factors modulating tinnitus experience. Ear Hear. 40 (3), 636–644 (2019).
Newman, C. W., Jacobson, G. P. & Spitzer, J. B. Development of the tinnitus handicap inventory. Arch. Otolaryngol.–Head Neck Surg. 122 (2), 143–148 (1996).
Song, Z. et al. Tinnitus is associated with extended high-frequency hearing loss and hidden high-frequency damage in young patients. Otol. Neurotol. 42 (3), 377–383 (2021).
Jafari, Z., Baguley, D., Kolb, B. E. & Mohajerani, M. H. A systematic review and meta-analysis of extended high-frequency hearing thresholds in tinnitus with a normal audiogram. Ear Hear. 43 (6), 1643–1652 (2022).
Ahmed, S. H. et al. SARS-CoV-2 vaccine-associated-tinnitus: A review. Ann. Med. Surg. 75, 103293 (2022).
Acknowledgements
We thank Megan Dotzenrod and Annalise Kieley for their assistance with data collection and identification of peaks on Auditory Brainstem Responses at the University of Connecticut. We also very much appreciate the work of Abigail Fellows during the conception and planning of this project.
Funding
This research was funded by Hitchcock Foundation to C.N., the Munck-Pfefferkorn Novel and Interactive Grant program to, J.B., and the Connecticut Institute for the Brain and Cognitive Sciences to E.S.
Author information
Authors and Affiliations
Contributions
C.N. - Study design lead; funding; enrollment; data collection, analysis, and interpretation; manuscript preparation.E.S. - Study design; funding; data analysis and interpretation; manuscript preparation.S.L. -Enrollment, data analysis and interpretation; manuscript preparation. L. Z. - Enrollment; data collection; manuscript preparation.M. D. - Enrollment; data collection; manuscript preparation. A. K. - Enrollment; data collection; manuscript preparation. S. S. - Enrollment; data collection; manuscript preparation.J. P. - Enrollment; data collection, analysis, and interpretation; manuscript preparation. C. M. - Enrollment; data collection, analysis, and interpretation; manuscript preparation.C. E. - Enrollment; data collection, manuscript preparation.O. C. - Study design; data collection; manuscript preparation.J. G. - Statistical analysis, and interpretation; manuscript preparation. A. W. - Enrollment; data analysis, and interpretation. R. R. - Study design; enrollment; data collection, interpretation; manuscript preparation.J. B. - Study design; funding; analysis, and interpretation; manuscript preparation.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Niemczak, C., Skoe, E., Leigh, S. et al. Altered auditory brainstem responses are post-acute sequela of SARS-CoV-2 (PASC). Sci Rep 15, 9387 (2025). https://doi.org/10.1038/s41598-025-93664-4
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-93664-4
