
Abstract
The relationship between the prognostic nutritional index (PNI) and mortality in patients with hypertension remains unclear. This study aimed to investigate the specific shape of the dose-response relationship and to identify a clinically meaningful risk threshold for PNI in this population. This retrospective cohort study included 6,165 adults with hypertension from the National Health and Nutrition Examination Survey (NHANES) 2003-2018. Weighted Cox proportional hazards models and restricted cubic splines were used to evaluate the associations between PNI and all-cause and cardiovascular disease (CVD) mortality. During a median follow-up of 7.9 years, 1,733 all-cause and 516 CVD deaths occurred. We identified a non-linear, L-shaped association between PNI and mortality. The risk of mortality was significantly lower with increasing PNI up to an inflection point of 51.55, beyond which the association plateaued. Each unit increase in PNI below this threshold was associated with a 9% reduction in all-cause mortality risk (Fully adjusted HR = 0.91, 95% CI: 0.87–0.95). The association was stronger in hypertensive individuals younger than 60 years and those with comorbid diabetes (P for interaction < 0.05). In a hypertensive population, PNI demonstrates an L-shaped association with all-cause and CVD mortality, with a distinct threshold at 51.55. This pattern suggests that PNI serves as a robust biomarker of immunonutritional status, and it ≥ 51.55 is associated with reduced mortality risk, supporting its utility as a prognostic biomarker for risk stratification in hypertensive patients.
Similar content being viewed by others

Introduction
Hypertension poses a significant global public health challenge. In 2010, 31.1% (1.39 billion) of the global adult population were affected by hypertension, accounting for approximately 10% of total global healthcare expenditure1. Hypertension is recognized as one of the major risk factors for cardiovascular disease and premature mortality worldwide, contributing to nearly half of all adverse cardiac, cerebrovascular, and renal events2,3. Accumulating evidence from both human and animal studies suggests that autoimmune inflammation may contribute to the development of hypertension4,5,6.
The prognostic nutritional index, derived from serum albumin and peripheral blood lymphocyte count, provides a comprehensive reflection of chronic inflammation, immune function, and nutritional status. Initially established in 1984 for assessing the prognosis of cancer7, recent studies have indicated the PNI as a marker of inflammation associated with increased risk of mortality and prognosis of cardiovascular disease8,9. Low-grade inflammation is considered to play a pivotal role in the initiation and perpetuation of elevated blood pressure. Even after effective control of blood pressure, residual cardiovascular risk persists in hypertensive patients, partly attributed to potential immune cell activation and chronic inflammation10. Existing research has demonstrated an independent association of PNI with resistant hypertension11. However, the relationship between PNI and long-term clinical outcomes in hypertensive patients, especially mortality rates, has not been thoroughly investigated.
In order to address the knowledge gap, our aim was to examine the association between PNI and all-cause mortality and cardiovascular mortality among a nationally representative sample of adults with hypertension in the United States (US).
Materials and methods
Study population
The National Health and Nutrition Examination Survey (NHANES) is a population-based survey aimed at collecting information on the health and nutrition of American households, However, for the purpose of this analysis, which involves follow-up for mortality outcomes, we employed a retrospective cohort design based on this survey data. The data are collected through structured interviews conducted at participants’ homes, physical examinations carried out at mobile examination centers, and laboratory tests. The survey employs a multi-stage probability sampling design. The NHANES protocol has been approved by the Ethics Review Committee of the National Center for Health Statistics (NCHS), and all participants provide written informed consent before participating in the survey.
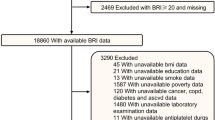
A total of 80,312 participants were included in the NHANES 2003–2018. Exclusion criteria were applied as follows (Fig. 1):1 individuals under the age of 18 years;2 participants without prognostic nutritional index data;3 participants without mortality rate data;4 participants without covariate data;5 individuals without hypertension. Ultimately, 6165 participants were included in the study. All data used in this research are publicly available (https://www.cdc.gov/nchs/nhanes/). To ensure the representativeness of the study results, subsequent data analysis was conducted with statistical weighting.

Flow diagram of the selection of eligible participants.
Definition of prognostic nutritional index
The Complete Blood Count (CBC) is a commonly employed laboratory test utilized to assess the impact of dietary intake and other factors on overall blood nutritional status and immune capability. The methodology for obtaining CBC parameters is based on the Beckman Coulter counting classification system12. Serum albumin levels are typically employed as an indicator of nutritional status, as determined using the Bromcresol Purple (BCP) method within the NHANES database. In this study, the prognostic nutritional index was calculated as: PNI = 5 * lymphocyte count (10^9/L) + serum albumin (g/L).
Outcomes assessment
Participants were followed up through December 31, 2015 unless dropping out or meeting the intended outcome. The mortality status of participants was authenticated by matching with the National Death Index. Referring to the International Classification of Disease, 10th Edition (ICD-10), Clinical Modification System codes, cardiovascular mortality was identified as deaths caused by CVD or cerebrovascular disease (ICD-10 codes I00 to I09, I11, I13, I20 to I51, and I60 to I69).
Assessment of covariates
We included various covariates that could potentially influence the results. Age, gender, race, smoking status, and medical conditions were collected through standardized questionnaires during home visits. Physical examinations, including measurement of body mass index (BMI), were conducted at the mobile examination center. Laboratory indicators used in the study included albumin, total protein, neutrophils, lymphocyte, white blood cell (WBC), hemoglobin, uric acid (UA), blood urea nitrogen (BUN), glycosylated hemoglobin (HbA1c), creatinine (Cr), alanine transaminase (ALT), aspartate transaminase (AST), total cholesterol (TC), triglycerides (TG), low-density lipoprotein cholesterol (LDL-C) and high-density lipoprotein cholesterol (HDL-C). Disease states were defined in detail. Individuals with an average systolic blood pressure (SBP) ≥140mmHg or an average diastolic blood pressure (DBP) ≥90mmHg, or those diagnosed with hypertension and receiving antihypertensive medication, were classified as having hypertension. Participants with a fasting plasma glucose level ≥ 7.0mmol/L or a HbA1c level ≥ 6.5%, as well as those with a diagnosed case of diabetes, were designated as having diabetes. The anemia was defined as a hemoglobin level < 130 g/L for male and < 120 g/L for female. The hypoalbuminemia was defined as serum albumin < 35 g/L.
Statistical analyses
In all of our analyses, we have considered sample weights to obtain national estimates. Additionally, a test for normality was conducted on the continuous variables. As the continuous variables did not conform to a normal distribution, they were represented using the median (interquartile range). Categorical variables were expressed as frequencies and percentages. A t-test was employed to compare the hypertensive population with the control group, while a one-way analysis of variance (ANOVA), Kruskal-Wallis H test, or chi-square test was used to assess differences among different quartile groups of PNI. Weighted Cox regression models were constructed to explore the association between PNI and mortality risk instead of traditional Cox regression, which was expressed as calculated hazard ratios (HRs) and 95% confidence interval (95% CIs). Crude analysis adjusted for no covariate, adjusted model adjusted for age, sex, race, education level, smoking status, BMI, SBP, DBP (model 1) and further adjust for ALT, TC, Cr, HbA1c, total protein, WBC (model 2), and fully adjusted model adjusted for age, sex, race, education level, smoking status, BMI, SBP, DBP, ALT, TC, Cr, HbA1c, total protein, WBC, CVD, Diabetes, anemia, hypoalbuminemia (model 3). The proportional hazards assumption was assessed using Schoenfeld residuals, the primary exposure variable (PNI) showed no evidence of violating the assumption in either all-cause or CVD mortality models. Kaplan-Meier survival analyses were applied to analyze the differences of survival rates according to PNI groups, and the differences were examined by log-rank test. To investigate the dose-response relationship between PNI and mortality, a restricted cubic spline (RCS) regression with the aforementioned multivariable adjustments was utilized. Non-linearity was examined using likelihood ratio tests. Stratified analyses were conducted based on gender (male, female), age ( > = 60 years, < 60 years), BMI (< 25, 25–30, > 30 kg/m2), diabetes (yes, no) and CVD (yes, no). Two-tailed p-values of < 0.05 were considered statistically significant.
Results
Baseline characteristics of study participants
A total of 15,817 NHANES participants were included in this study. The baseline features of all the eligible participants are presented in Table 1. Among them, the median age was 52 years, the male accounted for 49%, and the weighted prevalence of hypertension was 34%. The median value of PNI was 52.0, and the individuals with hypertension tended to have lower PNI relative to those without hypertension. We also identified higher BMI, SBP, DBP, WBC, ALT, AST, UA, serum creatinine, HbA1c, glucose, triglyceride, LDL, and lower HDL in hypertension individuals, while there was no material difference in cholesterol level. The overall prevalence rates of CVD, diabetes mellitus, anemia and hypoalbuminemia were 8.6%, 13.0%, 6.0%, and 1.8% respectively, and individuals with hypertension had a higher prevalence of these conditions. During a median follow-up of 7.9 person-years (4.3–11.5 years), the all-cause and CVD mortality were 7.9% and 2.2%, and hypertension individuals had a higher mortality than those without hypertension. Then, we divided the hypertension groups according to the PNI quartiles and compared the differences of the above indicators among the groups. The results are shown in Supplementary Table 1. Participants with higher PNI levels were more likely to be male, never smoker and White; and those had higher WBC, ALT, AST, TC, TG and lower HDL (all p < 0.05).
Correlations between PNI and clinical characteristics
The results of partial correlation analysis evaluating the correlations of PNI with clinical characteristics demonstrated that PNI was negatively correlated with BMI (r=-0.053 (-0.099, -0.030), p < 0.001), WC (r=-0.049 (-0.089, -0.029), p < 0.001), monocyte to lymphocyte ratio (MLR) (r=-0.255 (-0.359, -0.209), p < 0.001), neutrophil to lymphocyte ratio (NLR) (r=-0.237 (-0.345, -0.184), p < 0.001), Creatinine (r=-0.05 (-0.100, -0.024), p < 0.001), but positively correlated with TG (r = 0.063 (0.035, 0.116), p < 0.001), TC (r = 0.069 (0.042, 0.117), p < 0.001), total protein (r = 0.124 (0.072, 0.236), p < 0.001), hemoglobin (r = 0.097 (0.039, 0.203), p < 0.001). The positive correlation between PNI and total cholesterol (r = 0.069 (0.042, 0.117), p < 0.001), likely reflects their shared dependence on hepatic synthetic function, as albumin and cholesterol are both synthesized in the liver and serve as markers of nutritional status and metabolic health (Table 2).
Associations between PNI and mortality
As shown in Table 3, Higher PNI was associated with a decreased risk of all-cause mortality (HR = 0.95, 95%CI = 0.91–0.99) in the crude model. After multivariable adjustment, a consistent inverse association trend was observed. The hazard ratios and their precise statistical significance were as follows: Unadjusted model (HR = 0.95, 95%CI = 0.91–0.99, p = 0.014), model 1 (HR = 0.97, 95%CI = 0.94–1.02, p = 0.200), model 2 (HR = 0.97, 95%CI = 0.94-1.00, p = 0.042), and model 3 (HR = 0.98, 95%CI = 0.96-1.00, p = 0.016). Compared to the first quartile of PNI, multivariate-adjusted HRs for patients in the fourth quartile tend to be lower, with model 1 (HR = 0.61, 95%CI = 0.50–0.74, p for trend < 0.001), model 2 (HR = 0.54, 95%CI = 0.43–0.67, p for trend < 0.001), model 3 (HR = 0.60, 95%CI = 0.48–0.76, p for trend < 0.001). This statistically significant association was consistent for CVD mortality. The Kaplan–Meier survival curve for all-cause and CVD mortality in the hypertension participants stratified by PNI groups was presented in Fig. 2. We observed the mortality was lower in individuals with a higher PNI than in those with a lower PNI, which was consistent with Cox regression analysis (log-rank p < 0.001).

Kaplan-Meier survival curve for mortality by PNI quartiles in hypertensive individuals. Kaplan-Meier curve of all-cause mortality (A) and cardiovascular mortality (B) among participants with hypertension. In the Kaplan-Meier curves, the population is stratified into four groups (Q1, Q2, Q3, Q4) based on the quartiles of PNI, and statistical analysis is conducted using the log-rank test. PNI, prognostic nutritional index; Q1, Quantile 1; Q2, Quantile 2; Q3, Quantile 3; Q4, Quantile 4.
Dose-response relationship between PNI and mortality
Estimated association between PNI and mortality outcomes in hypertension population was shown from restricted cubic spline. As demonstrated in Fig. 3, after adjusting for multiple potential confounders, we observed an ‘L-shaped’ association between PNI and the risk of all-cause and CVD death in hypertensive patients: the risk declined sharply as PNI increased to the inflection point of 51.55, with no further meaningful change beyond this threshold, the nonlinear associations between PNI and all-cause mortality or CVD mortality were statistically significant (p < 0.05). In addition, a clear threshold effect was observed. Indeed, when PNI is below 51.55, there is a significant reduction in the risk of mortality as PNI increases. This suggests that maintaining a higher PNI level may be beneficial in reducing mortality risk in individuals with hypertension.

Restricted cubic spline analysis of the association between PNI and mortality. The nonlinear association of PNI levels with the all-cause (A) and cardiovascular (B) mortality.
Subgroup analyses
As shown in Fig. 4, subgroup analyses were conducted to determine whether demographic characteristics and comorbidities could account for the association between PNI and mortality. Consistent results were observed when analyses were stratified by gender, age, BMI, diabetes and CVD subgroups both for all-cause and CVD mortality. The associations were generally consistent with those of the whole population. The interaction tests revealed no statistically significant interactions between PNI and any demographic or clinical subgroup for all-cause mortality (all p for interaction > 0.05) These findings indicate that the inverse association of PNI with mortality was stable across subgroups. It is worth noting that there was a 9% decreased risk of mortality per one-unit increment in PNI in hypertensive patients younger than 60 years old and a 7% decrease in patients with diabetes, consistent with the overall inverse association observed in the entire cohort. The prognostic value of PNI appears consistent across various patient subgroups, supporting its potential as a universal risk predictor in hypertensive populations.

Forest plot of subgroup analyses for the association between PNI and mortality. Hazard ratios (HRs) were calculated using multivariate Cox regression models adjusted for the variables listed in the fully adjusted model except for the variable used for stratification. Association of PNI levels with the all-cause (A) and cardiovascular (B) mortality.
Discussion
In this US nationally representative retrospective cohort study, we uncover a non-linear, L-shaped relationship between PNI and both all-cause and CVD mortality in hypertensive individuals, pinpointing 51.55 as a critical risk stratification threshold. This pattern reveals a biologically meaningful phenomenon: while PNI values below 51.55 were associated with a steep reduction in mortality risk (HR = 0.91 per unit increase), this association plateaued beyond this threshold. Our findings show associations that are biologically plausible when considered alongside existing literature on nutrition, immunity, and cardiovascular outcomes.
The immune-metabolic axis represents a potential conceptual framework that may help contextualize the observed association between PNI and mortality. Hypertension is characterized by chronic low-grade inflammation that disrupts metabolic homeostasis, creating a vicious cycle of vascular injury and end-organ damage. PNI, as a composite of immune (lymphocyte) and nutritional/metabolic (albumin) markers, directly reflects the integrity of this axis. Low lymphocyte counts indicate impaired adaptive immunity and reduced capacity to resolve vascular inflammation, while hypoalbuminemia disrupts metabolic buffering and exacerbates insulin resistance13,14. Thus, PNI below 51.55 may reflect compromised immune and metabolic status. Notably, PNI remained an independent predictor of mortality in our fully adjusted models after accounting for serum albumin and white blood cell count, and prior head-to-head comparison studies have confirmed PNI outperforms its single components in prognostic value for mortality15,16. This plateau effect reflects a ceiling effect of immunonutritional reserve in hypertensive individuals: once PNI exceeds 51.55 (indicating adequate nutritional status and intact immune function), further elevations in serum albumin or lymphocyte count fail to confer additional survival benefit, as the immunometabolic homeostasis is sufficiently maintained to counteract hypertension-related chronic inflammation and vascular injury. The steeper association between PNI and mortality at lower values could potentially indicate that more substantial physiological deficits exist at these levels. The plateau observed at higher PNI values suggests that once certain thresholds of nutritional and immune status are reached, additional improvements may have limited incremental benefit on mortality outcomes.
Some previous research has suggested potential links between gut microbiota, nutrition, and inflammation, though these relationships were not directly assessed in our study. Diet and nutritional status significantly influence gut microbiota composition, which in turn regulates systemic inflammation and metabolic health17. Dysbiosis in hypertension impairs the synthesis of short-chain fatty acids and vitamins critical for lymphocyte proliferation and albumin synthesis, while increased intestinal permeability allows LPS entry, activating inflammatory pathways that suppress lymphocyte function and reduce albumin synthesis. Hypothetically, if PNI reflects underlying gut-immune-nutritional interactions, the observed association with mortality might be partially explained by these pathways. However, our observational data cannot establish whether changes in PNI directly influence these biological processes or mortality outcomes17,18.
Several additional mechanisms reinforce the L-shaped association observed in our study. First, metabolic dysfunction and insulin resistance, as reflected by indices such as the triglyceride-glucose index, show similar nonlinear associations with mortality in hypertensive populations. The steeper slope at lower PNI values may correspond to periods of greater physiological vulnerability, while the plateau at higher values might indicate a threshold beyond which additional improvements in these parameters show attenuated associations with mortality19,20. Second, body composition alterations play a crucial role—low PNI often coincides with either sarcopenia or excess adiposity, both of which increase mortality risk through chronic inflammation, oxidative stress, and metabolic disturbances. Once healthier body composition is achieved, further improvements have diminishing effects on mortality.
Notably, the identified threshold of 51.55 aligns with biologically plausible values for its components and demonstrates consistency with established biological thresholds across multiple chronic conditions. This threshold value is consistent with values reported in other populations, suggesting it may have clinical relevance, though further validation is needed to determine its biological significance.
Our subgroup analysis demonstrated that the inverse association between PNI and mortality was consistent across demographic and clinical subgroups. This consistency strengthens the robustness of PNI as a mortality predictor in hypertensive populations and suggests its universal applicability regardless of age or diabetes status. The consistent inverse association observed across all subgroups indicates that immunonutritional status, as reflected by PNI, serves as a fundamental determinant of mortality risk in hypertension, transcending the influence of specific demographic characteristics or comorbidities. This uniformity enhances the clinical utility of PNI as a broadly applicable risk stratification tool rather than one limited to specific patient subpopulations.
The clinical implications of our findings are substantial and immediate. The 51.55 threshold provides a concrete, readily applicable tool for risk stratification in hypertension management. Clinicians may perform appropriate rounding (e.g., to 51 or 52) based on laboratory detection accuracy and individual patient conditions. Patients with PNI below this cutoff represent a high-risk subgroup that may warrant targeted nutritional assessment and anti-inflammatory monitoring, and specific interventions targeting the two core components of PNI are recommended:1 For improving serum albumin: individualized supplementation with high-quality dietary protein (e.g., lean meat, fish, eggs, dairy products) and oral nutritional support for patients with mild hypoalbuminemia (30–35 g/L) to correct nutritional insufficiency;2 For enhancing lymphocyte count: adoption of an anti-inflammatory diet rich in fruits, vegetables, whole grains and polyunsaturated fatty acids to alleviate chronic low-grade inflammation, regular monitoring of peripheral blood lymphocyte count for persistent lymphopenia, and avoidance of unnecessary long-term immunosuppressive agents. The consistent association of PNI with mortality across diverse patient subgroups suggests that this risk stratification approach is broadly applicable to hypertensive patients of all ages and diabetes statuses. The L-shaped relationship further suggests that interventional strategies should focus on bringing patients above this critical threshold rather than pursuing maximal possible PNI elevation.
It is important to acknowledge several limitations of this study. Firstly, the observational nature of this retrospective study makes it susceptible to recall bias. Additionally, the patient data was sourced from a single center, which may limit generalizability. Secondly, this study assessed the association between PNI and mortality, our study lacked complete data on certain lifestyle factors (e.g., alcohol consumption, detailed physical activity) and specific medication use. While we adjusted for smoking status and key comorbidities and biomarkers that are closely linked to these unmeasured factors, we cannot fully rule out residual confounding. Third, we lacked detailed data on dietary habits, such as total caloric or protein intake. Although we adjusted for BMI and serum total protein as proxies for nutritional status, and the PNI itself incorporates albumin (a nutritional marker), we cannot completely rule out residual confounding by unmeasured dietary factors. Fourth, our study was unable to directly compare the predictive performance of PNI against other inflammatory biomarkers such as CRP using formal reclassification metrics (e.g., Net Reclassification Index) due to the incomplete availability of CRP measurements across the multiple NHANES cycles included in our analysis. This represents an important limitation when interpreting the relative prognostic value of PNI compared to established biomarkers. Finally, a significant methodological consideration in our study is the potential for reverse causality, where low PNI may reflect unmeasured disease severity or subclinical illness rather than directly influencing mortality risk. Although we adjusted for multiple markers of organ function and inflammation in our multivariable models, and observed consistent associations across participants with and without baseline cardiovascular disease, we cannot eliminate this possibility entirely as an observational study. Future prospective studies with repeated PNI measurements and interventional designs are needed to establish whether PNI improvement directly contributes to mortality reduction in hypertensive populations.
Conclusion
In summary, we provided evidence that higher PNI were significantly associated with a lower risk of all-cause and CVD mortality. The L-shaped associations of PNI and risks of mortalities were observed and the threshold was 51.55. The results were robust in subgroup analyses and PNI may exhibit heightened prognostic potential and clinical significance in hypertensive individuals with comorbid diabetes and younger than 60 years.
Data availability
All data used in this research are publicly available (https://www.cdc.gov/nchs/nhanes/).
References
Mills, K. T., Stefanescu, A. & He, J. The global epidemiology of hypertension. Nat. Rev. Nephrol. 16 (4), 223–237. https://doi.org/10.1038/s41581-019-0244-2 (2020).
Yano, Y. et al. Isolated diastolic hypertension and risk of cardiovascular disease: controversies in hypertension - pro side of the argument. Hypertension 79 (8), 1563–1570. https://doi.org/10.1161/hypertensionaha.122.18459 (2022).
Rapsomaniki, E. et al. Blood pressure and incidence of twelve cardiovascular diseases: lifetime risks, healthy life-years lost, and age-specific associations in 1·25 million people. Lancet 383 (9932), 1899–1911. https://doi.org/10.1016/s0140-6736(14)60685-1 (2014).
Harrison, D. G., Coffman, T. M. & Wilcox, C. S. Pathophysiology of hypertension: the mosaic theory and beyond. Circ. Res. 128 (7), 847–863. https://doi.org/10.1161/circresaha.121.318082 (2021).
Guzik, T. J. et al. Immune and inflammatory mechanisms in hypertension. Nat. Rev. Cardiol. 21 (6), 396–416. https://doi.org/10.1038/s41569-023-00964-1 (2024).
Wolf, V. L. & Ryan, M. J. Autoimmune disease-associated hypertension. Curr. Hypertens. Rep. 21 (1), 10. https://doi.org/10.1007/s11906-019-0914-2 (2019).
Onodera, T., Goseki, N. & Kosaki, G. [Prognostic nutritional index in gastrointestinal surgery of malnourished cancer patients]. Nihon Geka Gakkai Zasshi. 85 (9), 1001–1005 (1984).
Aktas, G. Association between the prognostic nutritional index and chronic microvascular complications in patients with type 2 diabetes mellitus. J. Clin. Med. 12 (18). https://doi.org/10.3390/jcm12185952 (2023).
Yu, J. H., Chen, Y. & Yin, M. G. Association between the prognostic nutritional index (PNI) and all-cause mortality in patients with chronic kidney disease. Ren. Fail. 45 (2), 2264393. https://doi.org/10.1080/0886022x.2023.2264393 (2023).
Caillon, A. & Schiffrin, E. L. Role of inflammation and immunity in hypertension: Recent epidemiological, laboratory, and clinical Evidence. Curr. Hypertens. Rep. 18 (3), 21. https://doi.org/10.1007/s11906-016-0628-7 (2016).
Yılmaz, F., Keleş, M. & Bora, F. Relationship between the prognostic nutritional index and resistant hypertension in patients with essential hypertension. Clin. Exp. Hypertens. 44 (4), 326–333. https://doi.org/10.1080/10641963.2022.2036995 (2022).
Hsieh, M. M. et al. Prevalence of neutropenia in the U.S. population: age, sex, smoking status, and ethnic differences. Ann. Intern. Med. 146 (7), 486–492. https://doi.org/10.7326/0003-4819-146-7-200704030-00004 (2007).
Wu, T. T. et al. Association between extremely high prognostic nutritional index and all-cause mortality in patients with coronary artery disease: Secondary analysis of a prospective cohort study in China. BMJ Open. 14 (6), e079954. https://doi.org/10.1136/bmjopen-2023-079954 (2024).
Cheng, Y. L. et al. Prognostic nutritional index and the risk of mortality in patients with acute heart failure. J. Am. Heart Assoc. 6 (6). https://doi.org/10.1161/jaha.116.004876 (2017).
Wang, J. & Pan, W. Albumin-related nutritional indices and all-cause and cause-specific mortality in older adults with severe dysphagia receiving artificial feeding. Front. Nutr. 12, 1756087. https://doi.org/10.3389/fnut.2025.1756087 (2025).
Wu, W. J. et al. Comparison of the prognostic value of different inflammation-based scores in patients with hepatocellular carcinoma after Lenvatinib therapy. World J. Gastroenterol. 31 (47), 113776. https://doi.org/10.3748/wjg.v31.i47.113776 (2025).
Chen, Z. et al. Association of an antioxidant-rich diet with all-cause and cardiovascular mortality in hypertensive patients: A prospective study. Med. (Baltim). 104 (29), e43443. https://doi.org/10.1097/md.0000000000043443 (2025).
Youqi, Z. et al. Sex-specific associations of the Dietary Inflammatory Index with cardiovascular and non-cardiovascular mortality in hypertensive adults: A cohort study. BMC Public. Health. 25 (1), 2055. https://doi.org/10.1186/s12889-025-23232-y (2025).
Li, C. et al. The triglyceride-glucose index and its obesity-related derivatives as predictors of all-cause and cardiovascular mortality in hypertensive patients: Insights from NHANES data with machine learning analysis. Cardiovasc. Diabetol. 24 (1), 47. https://doi.org/10.1186/s12933-025-02591-1 (2025).
Huang, Y. et al. Inflammatory markers link triglyceride-glucose index and obesity indicators with adverse cardiovascular events in patients with hypertension: Insights from three cohorts. Cardiovasc. Diabetol. 24 (1), 11. https://doi.org/10.1186/s12933-024-02571-x (2025).
Acknowledgements
This research was funded by the Key Research and Development Plan of Hunan Province (2020SK2081).
Funding
This research was funded by the Key Research and Development Plan of Hunan Province (2020SK2081).
Author information
Authors and Affiliations
Contributions
W.L. designed the research. C.C., Y.L., and X.G. collected and analyzed the data. W.L. and S.W. wrote the main manuscript text. D.P. provided critical revisions. All authors reviewed and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Liu, W., Liu, Y., Guo, X. et al. Association of prognostic nutritional index with all-cause and CVD mortality in hypertensive individuals. Sci Rep 16, 14981 (2026). https://doi.org/10.1038/s41598-026-45144-6
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-026-45144-6
