
Summary:
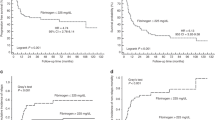
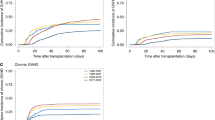
We have previously described a scoring system for patients undergoing hemopoietic stem cell transplantation (HSCT) based on day +7 blood urea nitrogen (BUN) and serum bilirubin levels. We have revised that scoring system using a formal multivariate approach based on a training phase (305 patients) and a validation phase (217 patients). Day +7 BUN, serum cholinesterase (CHE), total proteins (TP), gamma glutamyl transferase (γGT), donor type and cell dose at transplant were included in the new score. The score distribution identified three groups of patients in the training set (<25, 25-75, >75 percentile of the score) which were classified as low, intermediate and high risk. Their actuarial risk of transplant-related mortality (TRM) at 6 years was, respectively, 12, 38 and 60%. In the validation set the 6 year actuarial TRM was, respectively, 15, 40 and 69%. High risk patients had more graft-versus-host disease (GvHD) (P<0.0001) and lower platelet counts (P<0.0001). This study confirms that GvHD and TRM can be predicted on day +7 after HSCT: pre-emptive GvHD therapy may be one option for high-risk patients and is being tested in a prospective randomized trial. The score for single patients can be calculated on the web site http://213.26.110.20/lrm/day_seven_score.html.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$259.00 per year
only $21.58 per issue
Buy this article
- Purchase on SpringerLink
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout



Similar content being viewed by others

References
Frassoni F, Labopin M, Gluckman E et al. Results of allogeneic bone marrow transplantation for acute leukemia have improved in Europe with time – a report of the Acute Leukemia Working Party of the European Group for Blood and Marrow Transplantation (EBMT). Bone Marrow Transplant 1996; 17: 13.
Weiner RS, Bortin MM, Gale RP et al. Interstitial pneumonitis after bone marrow transplantation. Assessment of risk factors. Ann Intern Med 1986; 104: 168.
Gale RP, Bortin MM, van Bekkum DW et al. Risk factors for acute graft-vs-host disease. Br J Haematol 1987; 67: 397.
Weisdorf D, Hakke R, Blazar B et al. Risk factors for acute graft-versus-host disease in histocompatible donor bone marrow transplantation. Transplantation 1991; 51: 1197.
Storb R, Prentice RL, Thomas ED et al. Factors associated with graft rejection after HLA-identical marrow transplantation for aplastic anaemia. Br J Haematol 1983; 55: 573.
Bearman SI, Anderson GL, Mori M et al. Venoocclusive disease of the liver: development of a model for predicting fatal outcome after marrow transplantation. J Clin Oncol 1993; 11: 1729.
Bacigalupo A, Oneto R, Bruno B et al. Early predictors of transplant-related mortality (TRM) after allogeneic bone marrow transplants (BMT): blood urea nitrogen (BUN) and bilirubin. Bone Marrow Transplant 1999; 24: 653–659.
Lamparelli T, van Lint MT, Gualandi F et al. Bone marrow transplantation for chronic myeloid leukemia (CML) from unrelated and sibling donors: single center experience. Bone Marrow Transplant 1997; 20: 1057.
Bacigalupo A, Oneto R, Bruno B et al. Serum cholinesterase is an early marker of graft versus host disease (GvHD) and transplant related mortality (TRM). Bone Marrow Transplant 2001; 28: 1093–1096.
Locasciulli A, Testa M, Valsecchi MG et al. On behalf of the Infectious Diseases-Working Party of the European Blood and Marrow Transplantation Group. The role of hepatitis C and B virus infections as risk factors for severe liver complications following allogeneic BMT: a prospective study by the infectious disease Working Party of the European Blood and Marrow Transplantation Group. Transplantation 1999; 68: 1486–1491.
Adler M, Verset D, Bouhdid H, Bourgeois N et al. Prognostic evaluation of patients with parenchymal cirrhosis : proposal of a new simple score. J Hepatol 1997; 26: 642.
Garello E, Battista S, Bar F et al. Evaluation of hepatic function in liver cirrosis: clinical utility of galactose elimination capacity, hepatic clearance of D-sorbitol and laboratory investigations. Dig Dis Sci 1999; 44: 782.
Fink JC, Cooper MA, Burkahrt KM et al. Marked enzymuria after bone marrow transplantation: a correlate of veno occlusive disease induced hepatorenal syndrome. J Am Soc Nephrology 1995; 6: 1655.
Cooke KR, Krenger W, Hill G et al. Host reactive donor T cells are associated with lung injury after experimental allogeneic bone marrow transplantation. Blood 1998; 92: 2571–2580.
Panoskaltsis-Mortari A, Strieter RM, Hermanson JR et al. Induction of monocyte and T-cell attracting chemokines in the lung during the generation of idiopathic pneumonia syndrome following allogeneic murine bone marrow transplantation. Blood 2000; 96: 834–839.
Ramsay NKC, Kersey JH, Robinson LL et al. A randomized study of the prevention of acute graft versus host disease. N Engl J Med 1982; 306: 392–397.
Bacigalupo A, Oneto R, Lamparelli T et al. Pre-emptive therapy of acute graft versus host disease: a pilot study with anti-thymocyte globulin (ATG). Bone Marrow Transplant 2001; 28: 1093–1096.
Acknowledgements
This work was supported by Associazione Italiana Ricerca contro il Cancro (AIRC) Milano grant to AB and Associazione Ricerca Trapianto Midollo Osseo (ARITMO) Genova. The great work of our nursing staff is gratefully acknowledged. The BMT transplant group from Hospital Gaslini, Genova, Italy is also gratefully aknowledged.
Author information
Authors and Affiliations
Appendix : Prediction of risk of TRM
Appendix : Prediction of risk of TRM
In order to predict the risk of TRM for a new patient undergoing HSCT using the predictive model built on the training set and validated on the validation set, the following procedure can be followed. First, the score for that patient can be calculated using the formula:

where CHE, TP, BUN and γGT assume the values 0, 1 or 2 according to the following criteria: (See Table A)
CHE=IU/dl; TP=gr/dl; BUN= mg/dl; γGT=IU/dl; donor type is 0 if it is an HLA-identical sibling and 1 if otherwise.
Second, the probability of TRM for the patient with a score=x, can be calculated by:

where Sx is calculated applying the formula reported in the Methods:

In our sample S0 (survival for a patient with all variables set as their mean values) is=0.66 and β=0.83.
Let us imagine a patient grafted from an HLA-identical sibling (donor type=0) who received 2.1 × 108 cells/kg, with day +7 CHE=4599, BUN=17, TP=5.4, γGT=78: from the table, we transform these values as CHE=2, BUN=0, TP=0, γGT=1, donor type=0. Using these transformed values, we calculate the score for that patient:

And the TRM at day 2500 is

This patients, with a probability of TRM at day 2500=23% is considered as low-risk patient.
Alternatively, one can log in to the web site http://213.26.110.20/lrm/day_seven_score.html and fill in the fields as indicated (cell dose × 108/kg, type of donor, day +7 value for CHE. TP, γGT, BUN: the program will calculate the score for that patient and indicate if he is low- intermediate- or high risk).
Rights and permissions
About this article
Cite this article
Sormani, M., Oneto, R., Bruno, B. et al. A revised day +7 predictive score for transplant-related mortality: serum cholinesterase, total protein, blood urea nitrogen, γ glutamyl transferase, donor type and cell dose. Bone Marrow Transplant 32, 205–211 (2003). https://doi.org/10.1038/sj.bmt.1704085
Received:
Accepted:
Published:
Issue date:
DOI: https://doi.org/10.1038/sj.bmt.1704085
Keywords
This article is cited by
-
Galectin-3 predicts acute GvHD and overall mortality post reduced intensity allo-HCT: a BMT-CTN biorepository study
Bone Marrow Transplantation (2024)
-
Net reclassification improvement with serial biomarkers and bed-sided spirometry to early predict the need of organ support during the early post-transplantation in-hospital stay in allogeneic HCT recipients
Bone Marrow Transplantation (2019)
-
New Directions for Rabbit Antithymocyte Globulin (Thymoglobulin®) in Solid Organ Transplants, Stem Cell Transplants and Autoimmunity
Drugs (2014)
-
Serum albumin level predicts survival of patients with gastrointestinal acute graft-versus-host disease after allogeneic stem cell transplantation
Annals of Hematology (2014)
-
IL15 levels on day 7 after hematopoietic cell transplantation predict chronic GVHD
Bone Marrow Transplantation (2013)
