
Abstract
Background:
The proposed cadmium-induced oestrogen mimicking effects in reproductive tissues, suggest a role of this widespread food contaminant in the development of hormone-dependent malignancies.
Methods:
We prospectively evaluated the association between tertiles of dietary cadmium exposure and epithelial ovarian cancer in 60 889 women from the population-based Swedish Mammography Cohort. Dietary cadmium was estimated using a food-frequency questionnaire at baseline (1987–1990) and in 1997. Multivariable-adjusted rate ratios (RR) were evaluated using Cox proportional hazards models.
Results:
During a mean follow-up of 18.9 years (1 149 470 person-years), we identified 409 incident cases of epithelial ovarian cancer, including 215 serous, 27 mucinous, 62 endometrioid and 12 clear cell tumours. We found no association between dietary cadmium exposure and the risk of ovarian cancer. Compared with the lowest tertile of cadmium exposure, the multivariable-adjusted RR for the highest tertile was 0.90 (95% confidence interval (CI): 0.71–1.15) for total epithelial ovarian cancer. Likewise, no association was observed in subtypes modelled with continuous dietary cadmium exposure; multivariable RR for each 1 μg per day increment of cadmium: 0.97 (95% CI: 0.93–1.02) for serous tumours, 0.94 (95% CI: 0.82–1.07) for mucinous tumours and 1.00 (95% CI: 0.92–1.08) for endometrioid and clear cell tumours.
Conclusion:
Our study suggests that dietary cadmium exposure is not likely to have a substantial role in ovarian cancer development.
Similar content being viewed by others
Main
The food-pollutant cadmium has been widely dispersed into the environment even in industrially non-polluted areas. Farmland and thereby food, may become contaminated by atmospheric deposition and by the use of cadmium-containing fertilizers and sewage sludge (Jarup and Åkesson, 2009). Even though shellfish, offal products and certain seeds have the highest concentrations of cadmium, the main sources of dietary cadmium exposure (80%) in most Western populations are bread and other cereals, potatoes, root crops and vegetables due the comparatively high consumption of these products. In Asian populations, rice is the dominating source (Jarup and Åkesson, 2009). Mechanistically, cadmium may induce cancer in multiple ways. Possible non-oestrogen-mediated mechanisms of carcinogenicity are aberrant gene expression, oxidative stress, inhibition of DNA damage repair (Jin et al, 2003) and apoptosis (Joseph, 2009) or epigenetic alterations (Arita and Costa, 2009). Cadmium can also mimic the in vivo effects of oestrogen in reproductive tissues (Johnson et al, 2003). These oestrogen-mimicking effects may be mediated both via the oestrogen receptor (ER) (Byrne et al, 2009) and through alternative pathways in the absence of ERs (Filardo et al, 2008; Yu et al, 2010).
The aetiology of ovarian cancer is not fully understood. Results from experimental studies support a potential role of oestrogens to stimulate proliferation of ovarian surface epithelium cells (Syed et al, 2001; Spillman et al, 2010), but epidemiological evidence is more inconclusive. Whereas long-term use of any type of hormone replacement therapy seems to increase the risk of ovarian cancer (Lukanova and Kaaks, 2005), some studies observed a weaker association in users taking hormones containing oestrogen combined with progestin (Pearce et al, 2009). The observed favourable effect of progestins could explain these findings. Nevertheless, taken together, the results support the hypothesis of long-term elevated oestrogen concentrations as aetiologic important for this disease. Also in favour of the oestrogen hypothesis is the protective effect of oral contraceptive use, as it decreases ovarian oestrogen production (Lukanova and Kaaks, 2005). The oestrogen-mimicking properties of cadmium and the role of oestrogens in the aetiology of ovarian cancer may suggest a role of cadmium in this malignancy.
In a large population-based prospective cohort of Swedish women, we previously observed statistically significant positive association between dietary cadmium exposure and risk of endometrial cancer (Åkesson et al, 2008), a cancer form where oestrogen unopposed by progesterone is the main factor influencing risk (Akhmedkhanov et al, 2001). There are no studies on the association between cadmium exposure and ovarian cancer. This study aims to assess whether, in this same cohort, long-term dietary cadmium exposure is associated with the incidence of epithelial ovarian cancer.
Materials and methods
Study population
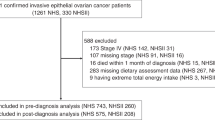
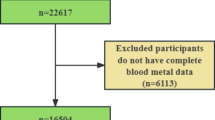
The Swedish Mammography Cohort was initiated in 1987–1990 when all women, born in 1914–48 and residing in Västmanland and Örebro counties of central Sweden, received a questionnaire including diet, lifestyle and reproductive factors, 74% responded (Åkesson et al, 2008). In 1997, data were updated; response rate was 70%. After exclusion of women with missing national registration number, implausible values for energy intake (mean ±3 s.d. value of loge-transformed energy intake), previous cancer diagnosis or bilateral oophorectomy, 60 889 women remained. The study was approved by the Regional Ethical Review Board in Stockholm, Sweden.
Dietary assessment
Dietary intake was assessed by a 67- and 96-item food frequency questionnaire (FFQ) at baseline and in 1997, respectively, where the women were asked how often, on average, they had consumed each food item. The National Food Administration provided data on the food-cadmium content. We estimated the average daily cadmium exposure by multiplying the frequency of consumption by age-specific portion sizes and the average cadmium content in each food item (Åkesson et al, 2008). The validity of the baseline questionnaire was previously assessed by comparing FFQ data with the average of four 1-week-weighted diet records among 129 randomly selected women of the cohort. Pearson correlation coefficients for the main cadmium-contributing food items ranged between 0.5–0.8.
Identification of ovarian cancer cases and follow-up of the cohort
Incident cases of invasive epithelial ovarian cancer were identified by linkage of the cohort to the National Cancer Registry, which is close to 100% complete (Mattsson and Wallgren, 1984). Ascertainment of deaths was obtained from the Swedish Death Registry and oophorectomies, and hysterectomies were obtained from the National Hospital Discharge Registry.
Statistical analysis
The estimated daily cadmium intake was adjusted for total energy intake of 1700 kcal (mean of the cohort) by using the residual method (Willett and Stampfer, 1986) and then categorized into tertiles. Follow-up was censored at the date of ovarian cancer diagnosis, death, bilateral oophorectomy or hysterectomy with unknown number of ovaries removed or 31 December 2009, whichever occurred first. Rate ratios (RR) and 95% confidence intervals (CIs) were estimated with Cox proportional hazards regression models with attained age as the timescale. In multivariable models, we adjusted for body mass index (BMI), post-secondary education, age at menarche, use of oral contraceptives, age at menopause, use of hormone replacement therapy, parity and age at first child birth. Linear trends across categories were tested using the median dietary cadmium intake values within categories as a continuous variable. All P-values were two-sided. Analyses on tumour subtypes were modelled with continuous cadmium exposure, due to the small number of cases. Statistical analyses were performed with STATA, version 11 (StataCorp., College Station, TX, USA).
Results
The characteristics of the study population are presented in Table 1. Women in the highest tertile of cadmium intake were more likely to have a post-secondary education and to be never-smokers compared with those in the lowest tertile.
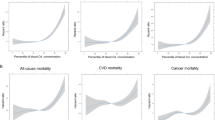
During a mean follow-up of 18.9 years (1 149 470 person-years) of 60 889 women, we identified 409 incident cases of epithelial ovarian cancer, including 215 serous, 27 mucinous, 62 endometrioid and 12 clear cell tumours. We found no association between dietary cadmium and risk of total epithelial ovarian cancer; neither after adjustment for age, nor in multivariable-adjusted analysis (Table 2). The lack of association remained also when starting follow-up in 1997 (multivariable-adjusted RR 1.03; 95% CI: 0.70–1.51 for all epithelial tumours) or in analysis comparing long-term consistently high intake of cadmium (> median) assessed twice (in 1987–1990 and 1997) (multivariable-adjusted RR 0.78; 95% CI: 0.55–1.10 for all epithelial tumours) with that of consistently low intake. Likewise, no association was observed for any subtype of ovarian cancer when modelled with continuous dietary cadmium exposure; multivariable RR for each 1 μg per day increment of cadmium: 0.97 (95% CI: 0.93–1.02) for serous tumours, 0.94 (95% CI: 0.82–1.07) for mucinous tumours and 1.00 (95% CI: 0.92–1.08) for endometrioid and clear cell tumours.
Further, no association was present across strata of BMI, post-menopausal hormone use, oral contraceptive use or smoking, neither in age-adjusted (data not shown), nor in multivariable-adjusted models (Table 2).
Discussion
In this prospective cohort of Swedish women, we observed no association between dietary cadmium exposure and the incidence of epithelial ovarian cancer. The lack of association persisted when starting follow-up later (1997), in the assessment of long-term consistent intake of cadmium and across strata of BMI, use of hormone replacement therapy, oral contraceptive use or smoking. To our knowledge, there are no other studies to date exploring the association between dietary cadmium exposure and ovarian cancer.
A possible reason for the lack of association in the present study, in contrary to that observed between dietary cadmium and endometrial cancer (Åkesson et al, 2008), is that oestrogen may not be the most important aetiologic factor for ovarian cancer (Risch, 1998). Indeed, a strong direct association was observed between circulating levels of oestrogen and endometrial cancer (Lukanova et al, 2004), but not ovarian cancer (Lukanova et al, 2003). Furthermore, even if obesity is associated with increased levels of circulating oestrogens, obesity seems to have a relatively weak adverse effect on ovarian cancer risk, if any (Renehan et al, 2010). Although cadmium may induce cancer also through non-oestrogen-mediated mechanisms (Jin et al, 2003; Arita and Costa, 2009; Joseph, 2009), the lack of an association in the present study does not support an important role of cadmium in the aetiology of ovarian cancer.
Our study has several strengths, including the prospective, population-based design, a relatively large number of cases and the nearly complete follow-up through linkage to population-based registers. We cannot exclude measurement error due to self-reported dietary intake, which could have influence on the lack of observed association. Additionally, due to a suggested ovarian cancer latency of 25–30 years (Risch, 1998), we may not have captured the relevant exposure time for ovarian carcinogenesis. In this study, we had the power (>80%) to detect increased relative risks of 1.4.
In conclusion, the present prospective study found no association between dietary cadmium exposure and risk of epithelial ovarian cancer. It suggests that dietary cadmium exposure is not likely to have a substantial role in ovarian cancer development.
Change history
29 March 2012
This paper was modified 12 months after initial publication to switch to Creative Commons licence terms, as noted at publication
References
Åkesson A, Julin B, Wolk A (2008) Long-term dietary cadmium intake and postmenopausal endometrial cancer incidence: a population-based prospective cohort study. Cancer Res 68 (15): 6435–6441
Akhmedkhanov A, Zeleniuch-Jacquotte A, Toniolo P (2001) Role of exogenous and endogenous hormones in endometrial cancer: review of the evidence and research perspectives. Ann N Y Acad Sci 943: 296–315
Arita A, Costa M (2009) Epigenetics in metal carcinogenesis: nickel, arsenic, chromium and cadmium. Metallomics 1 (3): 222–228
Byrne C, Divekar SD, Storchan GB, Parodi DA, Martin MB (2009) Cadmium--a metallohormone? Toxicol Appl Pharmacol 238 (3): 266–271
Filardo EJ, Quinn JA, Sabo E (2008) Association of the membrane oestrogen receptor, GPR30, with breast tumour metastasis and transactivation of the epidermal growth factor receptor. Steroids 73 (9–10): 870–873
Jarup L, Åkesson A (2009) Current status of cadmium as an environmental health problem. Toxicol Appl Pharmacol 238 (3): 201–208
Jin YH, Clark AB, Slebos RJ, Al-Refai H, Taylor JA, Kunkel TA, Resnick MA, Gordenin DA (2003) Cadmium is a mutagen that acts by inhibiting mismatch repair. Nat genet 34 (3): 326–329
Johnson MD, Kenney N, Stoica A, Hilakivi-Clarke L, Singh B, Chepko G, Clarke R, Sholler PF, Lirio AA, Foss C, Reiter R, Trock B, Paik S, Martin MB (2003) Cadmium mimics the in vivo effects of oestrogen in the uterus and mammary gland. Nat Med 9 (8): 1081–1084
Joseph P (2009) Mechanisms of cadmium carcinogenesis. Toxicol Appl Pharmacol 238 (3): 272–279
Lukanova A, Kaaks R (2005) Endogenous hormones and ovarian cancer: epidemiology and current hypotheses. Cancer Epidemiol Biomarkers Prev 14 (1): 98–107
Lukanova A, Lundin E, Akhmedkhanov A, Micheli A, Rinaldi S, Zeleniuch-Jacquotte A, Lenner P, Muti P, Biessy C, Krogh V, Berrino F, Hallmans G, Riboli E, Kaaks R, Toniolo P (2003) Circulating levels of sex steroid hormones and risk of ovarian cancer. Int J Cancer 104 (5): 636–642
Lukanova A, Lundin E, Micheli A, Arslan A, Ferrari P, Rinaldi S, Krogh V, Lenner P, Shore RE, Biessy C, Muti P, Riboli E, Koenig KL, Levitz M, Stattin P, Berrino F, Hallmans G, Kaaks R, Toniolo P, Zeleniuch-Jacquotte A (2004) Circulating levels of sex steroid hormones and risk of endometrial cancer in postmenopausal women. Int J Cancer 108 (3): 425–432
Mattsson B, Wallgren A (1984) Completeness of the Swedish Cancer Register. Non-notified cancer cases recorded on death certificates in 1978. Acta Radiol Oncol 23: 305–313
Pearce CL, Chung K, Pike MC, Wu AH (2009) Increased ovarian cancer risk associated with menopausal oestrogen therapy is reduced by adding a progestin. Cancer 115 (3): 531–539
Renehan AG, Soerjomataram I, Leitzmann MF (2010) Interpreting the epidemiological evidence linking obesity and cancer: A framework for population-attributable risk estimations in Europe. Eur J Cancer 46 (14): 2581–2592
Risch HA (1998) Hormonal aetiology of epithelial ovarian cancer, with a hypothesis concerning the role of androgens and progesterone. J Natl Cancer Inst 90 (23): 1774–1786
Spillman MA, Manning NG, Dye WW, Sartorius CA, Post MD, Harrell JC, Jacobsen BM, Horwitz KB (2010) Tissue-specific pathways for oestrogen regulation of ovarian cancer growth and metastasis. Cancer Res 70 (21): 8927–8936
Syed V, Ulinski G, Mok SC, Yiu GK, Ho SM (2001) Expression of gonadotropin receptor and growth responses to key reproductive hormones in normal and malignant human ovarian surface epithelial cells. Cancer Res 61 (18): 6768–6776
Willett W, Stampfer MJ (1986) Total energy intake: implications for epidemiologic analyses. Am J Epidemiol 124 (1): 17–27
Yu X, Filardo EJ, Shaikh ZA (2010) The membrane oestrogen receptor GPR30 mediates cadmium-induced proliferation of breast cancer cells. Toxicol Appl Pharmacol 245 (1): 83–90
Acknowledgements
This work was supported by The Swedish Cancer Society, the Swedish Research Council for Environment, Agricultural Sciences and Spatial Planning, and the Swedish Research Council/Research Infrastructures.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
From twelve months after its original publication, this work is licensed under the Creative Commons Attribution-NonCommercial-Share Alike 3.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-sa/3.0/
About this article
Cite this article
Julin, B., Wolk, A. & Åkesson, A. Dietary cadmium exposure and risk of epithelial ovarian cancer in a prospective cohort of Swedish women. Br J Cancer 105, 441–444 (2011). https://doi.org/10.1038/bjc.2011.238
Received:
Revised:
Accepted:
Published:
Issue date:
DOI: https://doi.org/10.1038/bjc.2011.238
Keywords
This article is cited by
-
Human papillomavirus infection, cervical cancer and the less explored role of trace elements
Biological Trace Element Research (2023)
-
Association between dietary intake and risk of ovarian cancer: a systematic review and meta-analysis
European Journal of Nutrition (2021)
-
Urinary cadmium and estimated dietary cadmium in the Women’s Health Initiative
Journal of Exposure Science & Environmental Epidemiology (2016)
-
Dietary cadmium exposure and prostate cancer incidence: a population-based prospective cohort study
British Journal of Cancer (2012)
-
Dietary cadmium and risk of invasive postmenopausal breast cancer in the VITAL cohort
Cancer Causes & Control (2012)
