
Abstract
Aims
There have been significant changes in the management of out of hours services in ophthalmology recently. The European Working Time Directive (EWTD) and economic measures have anecdotally reduced the availability of staff and facilities outside normal working hours, and there have been various responses to the provision of emergency surgical care. There are disparate attitudes to the optimum management of the emergency surgical case. We sought to establish a nationwide picture of the management of out of hours surgery.
Methods
A questionnaire was distributed to every consultant ophthalmologist working in the NHS and registered with the Royal College of Ophthalmologists (n=947). Information was requested regarding departmental and personal policies, local facilities, and personal beliefs regarding emergency surgery.
Results
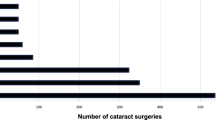
A total of 440 (46.5%) questionnaires were returned from 155 units; 18.7% of the units had no out of hours services or no operating facilities. Sixty-three percent of units reported a local policy regarding a time after which patients should not be taken to theatre. For 57%, this time began between 2100 hours and midnight. The most common reasons for not operating after a certain time were ‘belief that delay does not significantly affect the outcome’ (41.6%), ‘delayed access to theatre due to competition with other surgical specialities’ (40%), and ‘no specialist ophthalmic-theatre nursing input’ (32.7%).
Conclusion
We report the first nationwide study on out of hours ophthalmological surgical working practices. This demonstrates variation in work patterns. It is significant to patients and ophthalmologists that there should be units in United Kingdom without full local facilities and staff.
Similar content being viewed by others

Log in or create a free account to read this content
Gain free access to this article, as well as selected content from this journal and more on nature.com
or
References
Cullinane M, Gray AJG, Hargreaves CMK, Lansdown M, Martin IC, Schuber M et al The Report of the National Confidential Enquiry into Perioperative Deaths 2003.
Briggs M . Emergency eye care. The Royal College of Ophthalmologists Ophthalmic Services Guidance 2009 www.rcophth.ac.uk.
Lowry J, Cripps J . Results of the online EWTD trainee survey. Ann R Coll Surg Engl 2005; 87 (Suppl): 86–87.
Blanch RJ, Bindra MS, Jack AS, Scott RAH . Ophthalmic injuries in British armed forces in Iraq and Afghanistan. Eye 2011; 25: 218–223.
The Ocular Trauma Classification Group. A system for classifying mechanical injuries of the eye (globe). Am J Ophthalmol 1997; 123 (6): 820–831.
Colyer MH, Weber ED, Weichel ED, Dick JS, Bower KS, Ward TP et al. Delayed intraocular foreign body removal without endophthalmitis during operations Iraqi Freedom and Enduring Freedom. Ophthalmology 2007; 114 (8): 1439–1447.
Colyer MH, Chun DQ, Bower KS, Dick JS, Weichel ED . Perforating globe injuries during operation Iraqi Freedom. Ophthalmology 2008; 115 (11): 2087–2093.
Jaques H . Moving towards consultant delivered care. BMJ Careers. http://careers.bmj.com/careers/advice/view-article.html?id=20005242. Accessed on November 2011.
Acknowledgements
We thank Mrs Tracy Sparey for her help with the administration of this survey.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Additional information
Presented as a poster at the Oxford Ophthalmological Congress, July 2011.
Rights and permissions
About this article
Cite this article
O'Colmain, U., Wright, M., Bennett, H. et al. Out of hours ophthalmic surgery: a UK national survey. Eye 27, 363–366 (2013). https://doi.org/10.1038/eye.2012.280
Received:
Accepted:
Published:
Issue date:
DOI: https://doi.org/10.1038/eye.2012.280
