
Abstract
Purpose
To assess the relationship between age, corneal astigmatism, and ocular dimensions with reference to astigmatism correction during cataract surgery.
Methods
In this cross-sectional study of right eyes of 2247 consecutive patients attending cataract surgery preassessment, data on patient demographics, axial length (AL), anterior chamber depth (ACD), and keratometric astigmatism were collected. Astigmatism was further analyzed as against-the-rule (ATR: steepest meridian 180±30°), with-the-rule (WTR: 90±30°), and oblique (OB: 30–60°or 120–150°).
Results
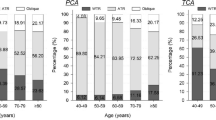
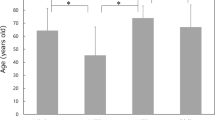
Mean age, AL, and ACD were 72.28±13.84 years, 23.99±1.85 mm and 3.08 ±0.52 mm, respectively. In all, 20.4% eyes had ≤0.50 diopters (D), 55.2% had 0.51–1.50 D, 7.9% had 2.01–3.00 D, and 3.7% eyes had >3.00 D of astigmatism. Overall, 44.2% of eyes had corneal astigmatism >1.00 D. Average astigmatism in age ranges 40–49, 50–59, 60–69, 70–79, 80–89, and 90+ years were 0.82, 1.04, 1.04, 1.02, 1.15 and 2.01 D, respectively. The magnitude of preoperative astigmatism positively correlated with age (P<0.0001), with increasing and decreasing prevalence of ATR and WTR astigmatism, respectively, with advancing age. The magnitude of ATR astigmatism inversely correlates to AL (P<0.0001). ATR astigmatism is more prevalent with increasing magnitude of astigmatism (P<0.0001).
Conclusions
A majority of patients for cataract surgery have astigmatism between 0.51 and 1.5 D. ATR astigmatism increases, whereas WTR decreases with age. ATR astigmatism inversely correlates to AL. With increasing age, the magnitude of astigmatism increases and ATR astigmatism becomes increasingly prevalent. The likelihood of a patient requiring astigmatic correction increases with age.
Similar content being viewed by others

Log in or create a free account to read this content
Gain free access to this article, as well as selected content from this journal and more on nature.com
or
References
Guan Z, Yuan F, Yuan YZ, Niu WR . Analysis of corneal astigmatism in cataract surgery candidates at a teaching hospital in Shanghai, China. J Cataract Refract Surg 2012; 38 (11): 1970–1977.
Budak K, Friedman NJ, Koch DD . Limbal relaxing incisions with cataract surgery. J Cataract Refract Surg 1998; 24 (4): 503–508.
Wang L, Misra M, Koch DD . Peripheral corneal relaxing incisions combined with cataract surgery. J Cataract Refract Surg 2003; 29 (4): 712–722.
Morlet N, Minassian D, Dart J . Astigmatism and the analysis of its surgical correction. Br J Ophthalmol 2001; 85 (9): 1127–1138.
Bayramlar H, Daglioglu MC, Borazan M . Limbal relaxing incisions for primary mixed astigmatism and mixed astigmatism after cataract surgery. J Cataract Refract Surg 2003; 29 (4): 723–728.
Amesbury EC, Miller KM . Correction of astigmatism at the time of cataract surgery. Curr Opin Ophthalmol 2009; 20 (1): 19–24.
Buckhurst PJ, Wolffsohn JS, Davies LN, Naroo SA . Surgical correction of astigmatism during cataract surgery. Clin Exp Optom 2010; 93 (6): 409–418.
Hasegawa Y, Okamoto F, Nakano S, Hiraoka T, Oshika T . Effect of preoperative corneal astigmatism orientation on results with a toric intraocular lens. J Cataract Refract Surg 2013; 39 (12): 1846–1851.
Chen W, Zuo C, Chen C, Su J, Luo L, Congdon N et al. Prevalence of corneal astigmatism before cataract surgery in Chinese patients. J Cataract Refract Surg 2013; 39 (2): 188–192.
Ferrer-Blasco T, Montes-Mico R, Peixoto-de-Matos SC, González-Méijome JM, Cerviño A . Prevalence of corneal astigmatism before cataract surgery. J Cataract Refract Surg 2009; 35 (1): 70–75.
Hoffmann PC, Hutz WW . Analysis of biometry and prevalence data for corneal astigmatism in 23,239 eyes. J Cataract Refract Surg 2010; 36 (9): 1479–1485.
Khan MI, Muhtaseb M . Prevalence of corneal astigmatism in patients having routine cataract surgery at a teaching hospital in the United Kingdom. J Cataract Refract Surg 2011; 37 (10): 1751–1755.
Hayashi K, Hayashi H, Hayashi F . Topographic analysis of the changes in corneal shape due to aging. Cornea 1995; 14 (5): 527–532.
Ho JD, Liou SW, Tsai RJ, Tsai CY . Effects of aging on anterior and posterior corneal astigmatism. Cornea 2010; 29 (6): 632–637.
Riley AF, Grupcheva CN, Malik TY, Craig JP, McGhee CN . The Auckland Cataract Study: demographic, corneal topographic and ocular biometric parameters. Clin Experiment Ophthalmol 2001; 29 (6): 381–386.
Ueno Y, Hiraoka T, Miyazaki M, Ito M, Oshika T . Corneal thickness profile and posterior corneal astigmatism in normal corneas. Ophthalmology 2015; 122 (6): 1072–1078.
Hashemi H, Khabazkhoob M, Yekta A, Jafarzadehpur E, Emamian MH, Shariati M . High prevalence of astigmatism in the 40- to 64-year-old population of Shahroud, Iran. Clin Experiment Ophthalmol 2012; 40 (3): 247–254.
Grosvenor T . Etiology of astigmatism. Am J Optom Physiol Opt 1978; 55 (3): 214–218.
Vihlen FS, Wilson G . The relation between eyelid tension, corneal toricity, and age. Invest Ophthalmol Vis Sci 1983; 24 (10): 1367–1373.
Howland HC, Sayles N . Photokeratometric and photorefractive measurements of astigmatism in infants and young children. Vision Res 1985; 25 (1): 73–81.
Nanavaty MA, Vasavada AR, Patel AS, Raj SM, Desai TH . Analysis of patients with good uncorrected distance and near vision after monofocal intraocular lens implantation. J Cataract Refract Surg 2006; 32 (7): 1091–1097.
Mallen EA, Gammoh Y, Al-Bdour M, Sayegh FN . Refractive error and ocular biometry in Jordanian adults. Ophthalmic Physiol Opt 2005; 25 (4): 302–309.
Pineda R, Denevich S, Lee WC, Waycaster C, Pashos C . Economic evaluation of toric intraocular lens: a short- and long-term decision analytic model. Arch Ophthalmol 2010; 128 (7): 834–840.
Nemeth G, Szalai E, Berta A, Modis L Jr . Astigmatism prevalence and biometric analysis in normal population. Eur J Ophthalmol 2013; 23 (6): 779–783.
Leighton DA, Tomlinson A . Changes in axial length and other dimensions of the eyeball with increasing age. Acta Ophthalmol (Copenh) 1972; 50 (6): 815–826.
Olsen T, Arnarsson A, Sasaki H, Sasaki K, Jonasson F . On the ocular refractive components: the Reykjavik Eye Study. Acta Ophthalmol Scand 2007; 85 (4): 361–366.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Additional information
A brief version of this paper has been presented at the Annual Meeting of the British Society of Refractive Surgery, Birmingham, UK, March 2015, as well as at the Annual Meeting of Students' Independent Research Project Conference, Brighton, UK.
Author contributions
OCW: Data collection, analysis, manuscript drafting, statistical analysis and interpretation. RA: Data collection, analysis, manuscript drafting. MAN: Concept and design, analysis, manuscript editing, drafting, and critical review.
Rights and permissions
About this article

Cite this article
Collier Wakefield, O., Annoh, R. & Nanavaty, M. Relationship between age, corneal astigmatism, and ocular dimensions with reference to astigmatism in eyes undergoing routine cataract surgery. Eye 30, 562–569 (2016). https://doi.org/10.1038/eye.2015.274
Received:
Accepted:
Published:
Issue date:
DOI: https://doi.org/10.1038/eye.2015.274
This article is cited by
-
Evaluation of an intraoperative marking technique using the body axis as a reference
Spektrum der Augenheilkunde (2022)
-
Central and mid-peripheral corneal astigmatism in an elderly population: a retrospective analysis of Scheimpflug topography results
Scientific Reports (2021)
-
Relationship between central and peripheral corneal astigmatism in elderly patients
Optical Review (2018)
-
Qualitative and quantitative evaluation of acute angle-closure mechanisms
BMC Ophthalmology (2017)
