
Abstract
Purpose: Mutations in the GJB2 gene are the most frequently found mutations in patients with nonsyndromic hearing impairment in populations studied to date. However, the prevalence of mutations varies among different ethnic groups. In most areas of China, genetic testing for nonsyndromic hearing impairment is currently not available because of the lack of information regarding the molecular cause of nonsyndromic hearing impairment. The purpose of this study is to determine the prevalence of a common GJB2 mutation, 235delC, in Chinese deaf children.
Methods: We collected DNA specimens from 3004 patients with nonsyndromic hearing impairment from 26 regions of China; 368 Han Chinese and 98 Uigur controls, and screened for the 235delC mutation. The coding exon of the GJB2 gene was polymerase chain reaction amplified, followed by restriction enzyme digestion with ApaI and analysis by agarose gel.
Results: Overall, 488 patients (16.3%) were determined to carry at least one 235delC mutant allele, with 233 (7.8%) homozygotes and 255 (8.5%) heterozygotes. Therefore, within the subpopulations examined, the frequency varies from 0% to 14.7% for 235delC homozygotes and from 1.7% to 16.1% for heterozygotes. On the basis of this survey of the patient cohort as stated, Chinese patients with nonsyndromic hearing impairment appear to have a relatively higher 235delC frequency than that of other Asian populations.
Conclusion: These results demonstrate that an easy and fast genetic testing method for this well-known GJB2 gene mutation can be made available for at least 2 million Chinese patients and family members with nonsyndromic hearing impairment. By screening for the common GJB2 235delC mutation, the molecular cause in as high as 15% of patients with nonsyndromic hearing impairment in certain regions of China can be identified. In addition, patients who are negative for the 235delC mutation would be candidates for further mutational analysis of GJB2 or other deafness-related genes.
Similar content being viewed by others

Main
Hearing impairment is the most common neurosensory disorder in humans with an incidence of approximately 1 in 1000 children.1 Approximately two thirds of cases have a genetic cause.1 Hereditary deafness is genetically heterogeneous. Nonsyndromic deafness accounts for 60% to 70% of inherited hearing impairment and involves more than 100 different genes demonstrating autosomal dominant (DFNA), autosomal recessive (DNFB), X-linked (DFN), and maternal inheritance.2 For many populations, the most common cause of nonsyndromic autosomal recessive hearing loss is mutations in Connexin 26, a gap junction protein encoded by the GJB2 gene.3–10 Approximately 30% to 40% of hereditary deafness is syndromic, presenting with other clinical features in addition to hearing impairment.
To date, more than 100 mutations, polymorphisms, and unclassified variants have been described in the GJB2 gene (http://davinci.crg.es/deafness). The mutation spectrum and prevalence of mutations vary significantly among different ethnic groups. Three mutations, 35delG, 167delT, and 235delC, are found to be the most frequent mutations in white, Ashkenazi Jewish, and Asian populations, respectively.3,4,6–15 A recent multicenter study reported that the 35delG mutation accounted for 72.4% of GJB2 mutant alleles in 1718 white patients with biallelic DFNB1 mutations, including delGJB6-D13S1830.16 In the Ashkenazi Jewish population, 35delG and 167delT accounted for 96% of the GJB2 mutant alleles.17 However, the 35delG mutation is rarely found in Asian patients. Instead, the 235delC mutation was the most prevalent in Japanese, Korean, and Taiwanese.7,8,11,18,19
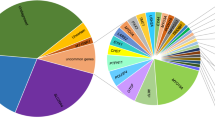
In China, it is estimated that 30,000 babies are born with congenital hearing impairment every year.20 Because of the lack of an established molecular cause in Chinese deaf children, genetic testing has not been offered in most areas of China. Recent reports demonstrated that 235delC is the most prevalent GJB2 mutation in Taiwanese, a subpopulation of Chinese. A large number of Han people from mainland China's coastal provinces of Fujian and Guangdong emigrated to Taiwan in the 16th century, and more recently in 1949, there was another influx of Chinese from mainland China during the retreat of Kuo-Ming-Dong army led by Chiang. Thus, approximately 98% of the Taiwanese population are Han Chinese (http://www.gio.gov.tw/taiwan-website/5-gp/yearbook/p028.html). China is a large country with more than 56 different subracial groups (e.g., Han, Man, Mon, Hui, Zang, Miao, Yi, Wa, Bai, Zhuang, Wei, Qiang, and NaXi) clustered in different parts of the country. The Han people make up 91.9% of the Chinese population of approximately 1.3 billion (http://education.yahoo.com/reference/factbook/ch/popula.html). Therefore, we hypothesize that the 235delC mutation is likely to be the most prevalent mutation in mainland China. Our first step toward a comprehensive genetic analysis of deaf children in different regions of China is to determine the frequency of the 235delC mutation in different regions of China and Chinese subpopulations. In this study, we report the results of screening the 235delC mutation in 3004 patients with nonsyndromic hearing impairment (NSHI) from 26 different regions of China (Fig. 1).

Geographic distribution and proportion of patients carrying at least one 235delC mutant allele in each region studied.
MATERIALS AND METHODS
Patients and DNA samples
A total of 3004 unrelated students with NSHI from 26 different regions of China were included in this study. Parents were not included. Overall, the patients included in this study consisted of 1706 males and 1298 females from 2 to 30 years with an average age of 13.8 ± 4.5 (standard deviation) years. Although the majority of patients are Han Chinese, depending on the geographic location, the proportion of patients with minority ethnic backgrounds may be different. To broadly sample as many regions of China as possible, we included the remote northwestern provinces including Xinjiang (translates to New Territory), Tibet, and Qinghai, where minorities make up a significant part of the local population. We also included samples from the southwestern provinces of Yunnan and Guizhou, where the population is made up of a number of minorities originating from various native tribes. We included the approximate percentage of Han and minorities in the remote provinces in Table 1. In the eastern and southeast coastal provinces, the population consists of 90% to 98% Han Chinese.
The patients were identified through schools. Because the students attending the schools are from the same city or province in this study, they are reasonably representative of the general population in that region.
This study was performed according to a protocol approved by the ethics committee of the Chinese PLA General Hospital. Informed consent was obtained from parents of students aged less than 18 years or from adult patients themselves aged more than 18 years before blood sampling. The ethnic subgroup was categorized according to the information recorded in each individual's permanent residency documentation. Parents were interviewed to obtain family history information and a maternal pregnancy history in addition to the patients' age at diagnosis and clinical history, including infections, possible head or brain injuries, and exposure to aminoglycoside antibiotics. Only the patients with nonsyndromic hearing loss were included in this study. These patients showed moderate to profound bilateral sensorineural hearing impairment on audiograms. DNA specimens from all patients were analyzed by restriction fragment length polymorphism (RFLP) for the presence of the 235delC mutation in the GJB2 gene. In addition, we analyzed 368 control individuals with normal hearing, all Han Chinese from the capital, Beijing (Northern) and Jiangsu Province (Eastern), two densely populated regions, and 98 control individuals from Uigur of Xinjiang, the northwestern remote region of China. All DNA was extracted from peripheral blood leukocytes using a commercially available DNA extraction kit (Watson Biotechnologies Inc., Shanghai, China).
Mutational analysis
The 235delC mutation in GJB2 gene was analyzed by polymerase chain reaction (PCR) amplification using forward (5'-TTGGTGTTTGCTCAGGAAGA-3′) and reverse (5′-GGCCTACAGGGGTTTCAAAT-3′) primers located (115 base pair [bp] and 110 bp) upstream and downstream, respectively, of the single coding exon, followed by RFLP analysis. The 944-bp PCR product of a normal control DNA was digested with ApaI, producing two fragments with 585 bp and 359 bp. The 235delC mutation results in the loss of the ApaI site. A heterozygous mutation results in three DNA bands with 944, 585, and 359 bp, whereas the homozygous mutation produces a single 944-bp band (Fig. 2).

PCR/RFLP analysis of the 235delC mutation.. The DNA markers are 2000, 1000, 750, 500, 250, and 100 bp. Lane 1 is a homozygous 235delC control, lanes 2 and 3 are normal controls, lanes 5, 13, and 15 are heterozygous for 235delC, lane 21 is homozygous for 235delC, and other lanes are normal cases. The heterozygous 235delC mutation produces three bands; 944, 585, and 359 bp.
Statistical analysis
The statistical analysis was performed using SAS 9.1.3 software (SAS Inc., Cary, NC). Because there is a statistically significant difference in the whole comparison of 235delC mutant allele frequency of all subethnic groups in this study, the comparison of each two subethnic groups must use a corrected significance level: α' ≈ 0.00227 {α' = α/[0.5k(k − 1) + 1] = 0.05/[0.5 × 7 × (7 − 1) + 1] = 0.00227, k is the number of group, α = 0.05}. All comparisons between two subgroups in this study used this P value for the significance level.
RESULTS
Geographic distribution of patients
In China, approximately 94% (http://www.gxu.edu.cn/administration/gxdxjsb/zzcl/rkfb.htm) of the population is concentrated in the Southern (e.g., Guangdoung and Fujian provinces) and the Eastern (e.g., Beijing, Shanghai, Nanjing) parts of the country. The western half of the country is mostly sparsely populated desert (e.g., Xinjiang) and elevated plateau (e.g., Tibet). We studied patients from 26 regions, including the northwestern province, Xinjiang, the middle-west province Qinghai, and the northeastern province, Heilongjiang, as shown in Fig. 1. The population of each area studied is given in the second column of Table 1 (http://www.xzqh.org/quhua/index.htm). The number of patients studied from each region ranges from 31 (Shanghai) to 202 (Ningxia), with a total of 3004.
Frequency of homozygous and heterozygous 235delC GJB2 mutation in different regions of China
PCR/RFLP analysis (Fig. 2) of all 3004 patients for the presence of the 235delC mutation revealed a broad distribution of homozygote, heterozygote, and allele frequencies in different regions of China (Table 1). Among the 3004 patients, 233 (7.8%) were homozygous and 255 (8.5%) were determined to be heterozygous for the 235delC mutation. The frequency of homozygous 235delC varied from 0% in Lhasa, Tibet, to 14.7% in Beijing. Heterozygosity for 235delC varied from 1.7% in Lhasa, Tibet, to 16.1% in Shanghai. The total number of patients with NSHI carrying at least one 235delC mutant allele was 488 (16.3%), with a frequency as high as 26.5% in Nantong City, Jiangsu, and as low as 1.7% in Lhasa, Tibet. The 235delC mutant allele frequency varied with regions from 0.9% to 19.5%, yielding a nationwide average frequency of 12.0% based on the populations studied. Variability of distribution of 235delC homozygote, heterozygote, and mutant allele frequency among different regions of China was therefore evident. Six of seven cities where the 235delC frequency was more than 20% (20.2%–26.5%) were located in the eastern provinces (Fig. 1). In most regions, the proportion of 235delC homozygotes and heterozygotes was approximately equal. However in Beijing, Jilin, Korla (Xinjiang), and Guiyang, the number of 235delC homozygotes was approximately twice that of the heterozygotes, whereas, in Yuncheng, Fuyang, and Lanzhou, it was half that of the heterozygotes. In Xi'an, Liuzhou, Xining, and Lincang, the number of homozygotes represented only approximately 20% that of the number of heterozygotes. These regions also have the lowest 235delC allele frequency. These observations suggest that mutations other than 235delC in the GJB2 gene or other genes are responsible for NSHI in these patients.
We attribute part of the high variability of the frequency of the 235delC mutation in different regions to the makeup ofthe general population in the regions studied. To examine whether the difference in the frequency of the 235delC mutation among different subethnic populations is statistically significant, we performed a statistical comparison between two subethnic groups. The total populations of Han, Tibetan, Hui, Man, Mon, minorities in Xinjiang, and minorities in Southwestern China are 1137.4 million, 5.4 million, 9.8 million, 10.7 million, 5.8 million, 10.8 million, and 57.1 million, respectively (http://www.cnmuseum.com/intro/renkou_intro.asp, http://www.xzqh.org/quhua/index.htm). The 235delC frequency of Man, Mon, Han, and Hui minorities in Xinjiang and minorities in southwestern China and Tibet is 23.7%, 18.3%, 13.0%, 10.1%, 5.1%, 4.1%, and 0.8%, respectively (Table 2). When the 235delC allele frequency among different Chinese ethnic groups was compared, there was a statistically significant difference in the comparison of the whole subethnic groups, so we used a corrected P value of approximately .00227 for the cutoff of significance in the paired comparison. The Tibetan subethnic group has the lowest 235 delC mutant allele frequency (0.8%), which is statistically significant when compared with other subethnic groups, Han, Man, Mon, and Hui. The Man subethnic group has the highest (23.7%) 235delC mutant allele frequency, which is statistically significant when compared with Tibetan and minorities in Xinjiang and the Southwest. As shown in Table 2, the distribution of the 235delC mutant allele among different Chinese ethnic groups is variable. The 235delC mutation occurs at a much lower frequency in the minorities in the southwest and the northwest regions than in the majorities Han and Man. These results suggest that sequencing of the entire GJB2 gene is necessary to establish the mutation spectrum and mutation frequency within the Chinese subpopulations.
Comparison of the prevalence of 235delC in Asian populations
Previous reports have suggested that the prevalence of GJB2 common mutations among different ethnic groups varies.3,4,6–15 The 235delC is the most common GJB2 mutation in Asian populations, and its frequency also varies among intra-Asian ethnic groups and subpopulations. Overall, Chinese patients with NSHI as a group appear to carry the highest 235delC mutant allele frequency compared with Korean and Japanese patients with NSHI (Table 3). Thus the frequency of 235delC seems to decline from China (12.0%) to Korea (9.3%) to Japan (3.9%) (Table 3). It should be noted that this comparison is based on the limited reports on studies of particular regions in the countries.
DISCUSSION
This study represents the largest study of the common GJB2 mutation, 235delC, in patients with NSHI. Accordingly, we analyzed a total of 6008 GJB2 alleles for the presence of a 235delC mutation. Our results demonstrate that the 235delC mutation in the GJB2 gene accounts for a significant portion of Chinese patients with NSHI. An estimated 2 million in the Chinese population has NSHI.20 By assuming that the 235delC mutation is present in approximately 16% of the Chinese population with NSHI, then approximately 320,000 Chinese patients would be expected to test positive for this mutation. The PCR/RFLP diagnostic method is relatively straightforward, rapid, and inexpensive, enabling this genetic service to be readily available to Chinese patients with NSHI and their family members. For the sake of comparison, we would estimate that the average cost of GJB2 235delC genotyping per sample by PCR/RFLP is 18.3 Ren-Min-Bi (RMB), equal to approximately 2.5 U.S. dollars, which is approximately half of the cost of the Universal Newborn Hearing Screening in China. Most general hospitals in China have laboratories and equipment necessary for this testing. The GJB2 gene is small with a high mutation rate. If the 235delC mutation is detected in a heterozygous form, it should prompt analysis of the GJB2 gene for the second mutant allele. We screened 368 normal controls from Beijing and Jiangsu areas and identified five individuals with the heterozygous 235delC mutation; meanwhile, we screened 98 normal Uigur controls and identified no individuals with the heterozygous 235delC mutation. Thus, the carrier frequency of the 235delC mutation in the Han population from Beijing and Jiangsu is approximately 1.4%. This carrier frequency in the general population is similar to that reported for the Asian carrier rate.21 Because the carrier frequency of the 235delC mutation may be different in different subethnic groups, it is necessary to analyze controls from various regions and populations of China to determine the accurate carrier frequencies in overall and subethnic groups.
Previous reports3,4,6–15 suggested that the most frequent GJB2 mutation in whites, 35delG, represents a hot spot mutation. However, the prevalence of specific GJB2 mutations depends on the ethnic origin and founder effect: 167delT in Ashkenazi Jews6,17, R143W (c.427C>T) in a restricted village in Africa,22 and 235delC in Asian populations.7,18,23 These European, Jewish, and African common mutations have not been reported in Asian populations. Our results demonstrate that 235delC also occurs at a high frequency in the Chinese population with NSHI. Whether mutations other than 235delC in the region of the GJB2 gene are responsible for the Chinese patients with NSHI in regions where the frequency of the 235delC mutation is low is currently under investigation. Our preliminary results reveal that other GJB2 mutations account for an additional 6.1% of patients with NSHI from Xining, where the frequency of the 235delC mutation is only 3.7%. Nevertheless, sequencing analysis of the entire coding region of GJB2 gene in patients from Liuzhou, where the frequency of the 235delC mutation is 3.4%, reveals no additional mutations. These results have two important implications: the GJB2 gene needs to be sequenced in its entirety, and mutations in genes other than GJB2 responsible for NSHI should be looked for in patients who harbor one or no mutations in the GJB2 gene.
China today is a melting pot of Chinese people from more than 56 different ethnic backgrounds. The Han Chinese originating from the middle and eastern parts of China make up the majority of the population in China. Today the Man population from the northeastern part, the Zang and the Hui from the western part, the Mon from Mongolia, and the many aborigines from the southwestern part are admixing with Hans. Consequently the frequency of homozygotes can be expected to transiently decline according to Wahlund's principles.24,25 It is not clear whether the 235delC is a founder mutation. Several studies investigating the possible founder effect of 235delC in Asian populations have been reported.7,26,27 However, a definite conclusion was never reached because of the small size of samples. Further studies are necessary to determine whether the common mutation 235delC in China is a founder effect or a mutation hot spot.
The results of this study will facilitate the establishment of DNA diagnostic testing for the common GJB2 mutation in Chinese patients with NSHI. The variability in the prevalence of the 235delC mutation among different Asian populations suggests that other mutations in the GJB2 gene may be responsible for patients with NSHI from regions where the occurrence rate of the 235delC mutation is low. It is also possible that other genes, such as GJB6 or SLC26A4, may play a role. Since the molecular cause in the majority of the patients with NSHI in China remains unidentified, many patients will require sequencing of the entire coding region of the GJB2 gene or evaluation for mutations in other genes such as connexin 30, 31, 32, and SLC26A4.
References
Cohen MM, Gorlin RJ . Epidemiology, etiology and genetic patterns. Hereditary Hearing Loss and Its Syndromes. In: Gorlin RJ, Toriello HV, Cohen MM, (Eds.). Oxford: Oxford University Press, 1995; 9–21.
Bitner-Glindzicz M . Hereditary deafness and phenotyping in humans. Br Med Bull 2002; 63: 73–94.
Estivill X, Fortina P, Surrey S, Rabionet R, et al. Connexin-26 mutations in sporadic and inherited sensorineural deafness. Lancet 1998; 351: 394–398.
Gabriel H, Kupsch P, Sudendey J, Winterhager E, et al. Mutations in the connexin26/GJB2 gene are the most common event in non-syndromic hearing loss among the German population. Hum Mutat 2001; 17: 521–522.
Lench N, Houseman M, Newton V, Van Camp G, et al. Connexin-26 mutations in sporadic non-syndromal sensorineural deafness. Lancet 1998; 351: 415.
Morell RJ, Kim HJ, Hood LJ, Goforth L, et al. Mutations in the connexin 26 gene (GJB2) among Ashkenazi Jews with nonsyndromic recessive deafness. N Engl J Med 1998; 339: 1500–1505.
Ohtsuka A, Yuge I, Kimura S, Namba A, et al. GJB2 deafness gene shows a specific spectrum of mutations in Japan, including a frequent founder mutation. Hum Genet 2003; 112: 329–333.
Park HJ, Hahn SH, Chun YM, Park K, et al. Connexin26 mutations associated with nonsyndromic hearing loss. Laryngoscope 2000; 110: 1535–1538.
Rabionet R, Zelante L, Lopez-Bigas N, D'Agruma L, et al. Molecular basis of childhood deafness resulting from mutations in the GJB2 (connexin 26) gene. Hum Genet 2000; 106: 40–44.
Wilcox SA, Saunders K, Osborn AH, Arnold A, et al. High frequency hearing loss correlated with mutations in the GJB2 gene. Hum Genet 2000; 106: 399–405.
Abe S, Usami S, Shinkawa H, Kelley PM, et al. Prevalent connexin 26 gene (GJB2) mutations in Japanese. J Med Genet 2000; 37: 41–43.
Ballana E, Ventayol M, Rabionet R, Gasparini P, et al. Connexins and deafness. Available at: http://dawinci.crq.es/deafness. Accessed January 8, 2007.
Kelsell DP, Dunlop J, Stevens HP, Lench NJ, et al. Connexin 26 mutations in hereditary non-syndromic sensorineural deafness. Nature 1997; 387: 80–83.
Roux AF, Pallares-Ruiz N, Vielle A, Faugere V, et al. Molecular epidemiology of DFNB1 deafness in France. BMC Med Genet 2004; 5: 5.
Scott DA, Kraft ML, Carmi R, Ramesh A, et al. Identification of mutations in the connexin 26 gene that cause autosomal recessive nonsyndromic hearing loss. Hum Mutat 1998; 11: 387–394.
Snoeckx RL, Huygen PL, Feldmann D, Marlin S, et al. GJB2 mutations and degree of hearing loss: a multicenter study. Am J Hum Genet 2005; 77: 945–957.
Sobe T, Vreugde S, Shahin H, Berlin M, et al. The prevalence and expression of inherited connexin 26 mutations associated with nonsyndromic hearing loss in the Israeli population. Hum Genet 2000; 106: 50–57.
Hwa HL, Ko TM, Hsu CJ, Huang CH, et al. Mutation spectrum of the connexin 26 (GJB2) gene in Taiwanese patients with prelingual deafness. Genet Med 2003; 5: 161–165.
Wang YC, Kung CY, Su MC, Su CC, et al. Mutations of Cx26 gene (GJB2) for prelingual deafness in Taiwan. Eur J Hum Genet 2002; 10: 495–498.
Dai P, Liu X, Yu F, Zhu Q, et al. Molecular etiology of patients with nonsyndromic hearing loss from deaf-mute schools in 18 provinces of China. Chin J Otol 2006; 4: 1–5.
Tang HY, Fang P, Ward PA, Schmitt E, et al. DNA sequence analysis of GJB2, encoding connexin 26: observations from a population of hearing impaired cases and variable carrier rates, complex genotypes, and ethnic stratification of alleles among controls. Am J Med Genet 2006; 140: 2401–2415.
Brobby GW, Muller-Myhsok B, Horstmann RD . Connexin 26 R143W mutation associated with recessive nonsyndromic sensorineural deafness in Africa. N Engl J Med 1998; 338: 548–549.
Park HJ, Shaukat S, Liu XZ, Hahn SH, et al. Origins and frequencies of SLC26A4 (PDS) mutations in east and south Asians: global implications for the epidemiology of deafness. J Med Genet 2003; 40: 242–248.
Wahlund S . Zuzammensetzung von Populationen und Korrelationser-scheinungen vom Standpunkt der Vererbungslehre aus betrachtet. Hereditas 1928; 11: 65–106.
Ding Y-C, Wooding S, Harpending HC, Chi HC, et al. Population structure and history in East Asia, PNAS 2000; 97: 14003–14006.
Kudo T, Ikeda K, Kure S . Novel mutations in the connexin26 gene (GJB2) responsible for childhood deafness in the Japanese population. Am J Med Genet 2000; 17: 141–145.
Liu XZ, Xia XJ, Ke XM, Ouyang XM, et al. The prevalence of connexin 26 (GJB2) mutations in the Chinese population. Hum Genet 2002; 111: 394–397.
Acknowledgements
This work was supported by the Chinese National Nature Science Foundation Research Grant 30572015, Beijing Nature Science Foundation Research Grant 7062062 to Pu Dai and Chinese Capital Medical Development Scientific Funding 2005-1032 to Dongyi Han. The authors would like to thank Dr. Raye Alford and Dr. Dennis Johnson for their valuable suggestions.
Author information
Authors and Affiliations
Additional information
The authors declare no conflict of interest.
Rights and permissions
About this article
Cite this article
Dai, P., Yu, F., Han, B. et al. The prevalence of the 235delC GJB2 mutation in a Chinese deaf population. Genet Med 9, 283–289 (2007). https://doi.org/10.1097/GIM.0b013e31804d2371
Received:
Accepted:
Issue date:
DOI: https://doi.org/10.1097/GIM.0b013e31804d2371
Keywords
This article is cited by
-
A novel method for detecting nine hotspot mutations of deafness genes in one tube
Scientific Reports (2024)
-
A multiplex PCR amplicon sequencing assay to screen genetic hearing loss variants in newborns
BMC Medical Genomics (2021)
-
Genetic mutations of GJB2 and mitochondrial 12S rRNA in nonsyndromic hearing loss in Jiangsu Province of China
Journal of Translational Medicine (2013)
-
Estimation of carrier frequencies of six autosomal-recessive Mendelian disorders in the Korean population
Journal of Human Genetics (2012)
-
Genetic mutations in non-syndromic deafness patients of uyghur and han chinese ethnicities in xinjiang, China: a comparative study
Journal of Translational Medicine (2011)
