
Abstract
Purpose: To examine the feasibility of offering genetic susceptibility testing for lung cancer (GSTM1) via the Internet to smokers who were blood relatives of patients with lung cancer. Outcomes include proportion who logged on to the study website to consider testing, made informed decisions to log on and to be tested.
Methods: Baseline measures were assessed via telephone survey. Participants could choose to log on to the study website; those who did were offered testing. Informed decisions to log on and to be tested were indicated by concordance between the decision outcome and test-related attitudes and knowledge.
Results: Three hundred four relatives completed baseline interviews. One hundred sixteen eligible relatives expressed further interest in receiving information via the web. Fifty-eight logged on and 44 tested. Those logging on expressed greater quit motivation, awareness of cancer genetic testing, and were more likely to be daily Internet users than those who did not log on. Approximately half of the sample made informed decisions to log on and to be tested.
Conclusion: Interest in a web-based protocol for genetic susceptibility testing was high. Internet-delivered decision support was as likely as other modalities to yield informed decisions. Some subgroups may need additional support to improve their decision outcomes.
Similar content being viewed by others

Main
Availability of genetic susceptibility testing for common diseases is likely to increase as the evidence supporting gene-disease associations continues to grow.1 There is a good deal of optimism that such testing might be beneficial for motivating individuals to adopt healthy lifestyles.2 Genetic susceptibility testing for lung cancer has been suggested as a means to motivate smoking cessation.3 However, a challenge for integrating such testing into smoking cessation or other behavior change interventions is that most of these interventions are self-directed, low intensity, and obliged to be low in cost to maximize dissemination.4 Before any such integration, the feasibility of offering genetic susceptibility testing and conveying risk feedback, via alternate, user-friendly, self-directed delivery models, such as the Internet, must be assessed.5
To our knowledge, no studies to date have offered genetic susceptibility testing using solely a web-based format. This is despite the fact that 75% of Americans use the Internet on a regular basis, and the impact of Internet applications on physician–patient communication and health care delivery continues to expand.6–8 Though no studies have examined delivery of genetic test results via the Internet, research to date supports the examination of alternate delivery models in some settings. For example, one trial delivered genetic susceptibility testing for alpha-1 antitrypsin deficiency, a smoking-linked form of emphysema, via the mail to unaffected individuals with some success.9,10 Results of another trial, in which a computer-based decision-aid enhanced the knowledge of low-risk women with personal or family histories of breast cancer seeking BRCA1/2 susceptibility testing, suggest that such methods could potentially reduce the burden on genetic counselors who are limited in number in the United States and abroad.11 The Internet may be another promising means to deliver genetic susceptibility testing information and services, though the authors of the above trials rightly caution that research on alternate delivery models is nascent. For example, little is known about using such delivery models, such as predictors of accessing a web-based protocol, projected uptake rates, whether those who would otherwise be inclined toward testing based on their positive attitudes pursue testing using this modality, and whether individuals can use these tools to make informed decisions about genetic testing in the absence of a trained professional. Therefore, in the current study, we examine these outcomes to evaluate the feasibility of this approach.
GSTM1, a gene in the family of glutathione S-transferases, is one of a growing number of common genetic variants with an evidence base to support its use as a genetic susceptibility test that could be offered via the web. GSTM1 is one of several genes involved in the metabolism of nicotine and detoxification of carcinogens in cigarette smoke.12,13 DNA damage, as a result of tobacco smoke-related carcinogens, is higher among smokers with the GSTM1-null–null genotype than those with the non-null genotype. The overall relation between GSTM1 and lung cancer risk ranges from 1.13 to 1.20.14,15 Previous research has conveyed information about the mechanisms underlying GSTM1 and susceptibility to lung cancer via graphical images that lend themselves readily to communication via the web.16,17 A web-based format enables individuals to review information at their own pace and take time to consider whether they want to be tested. Individuals who want to be tested can collect their own DNA samples via noninvasive techniques such as mouthwash swishing that also reduce the cost and inconvenience of being tested. Accompanying educational messages can be conveyed to a broad literacy group, though there is conflicting evidence as to whether individuals can understand relatively low levels of risk.16–19
Numerous studies underscore the importance of a family history of lung cancer at any age in the complex prediction of lung cancer risk.20,21 Accordingly, it has been suggested that a lung cancer diagnosis in a close family member may be a prime opportunity or “teachable moment” to encourage smoking cessation by reinforcing the associated risks to family members who smoke.22,23 In this context, genetic susceptibility testing may be particularly appropriate for these family members to consider. Once again, a web-based genetic testing program would have the benefit of increasing access to information, testing, and self-directed cessation interventions to extended families that are likely to be geographically distant from each other and the patient with lung cancer.
Examining the feasibility of providing genetic susceptibility testing via a web-based protocol should include the assessment of several key constructs. First, it is unclear what the uptake rates and predictors of uptake for a web-based protocol are. Previous, nonweb-based, studies incorporating GSTM1 feedback have had moderate (48%) to high (83%) rates of willingness to be tested.17–19 Offers for genetic testing made via the mail for alpha-1 antitrypsin deficiency, a smoking-linked form of emphysema, reported an uptake rate of 33%.9,10 This rate is slightly lower than that found in the GSTM1 studies, but may be a useful comparison for the current study.
Several variables may impact uptake of a web-based protocol. Cognitive and emotional factors, such as worry and perceived risk24,25 related to lung cancer may influence engagement in learning about personal cancer risk, as might demographic variables.26 Previous findings related to interest in smoking cessation suggest that uptake rates may be higher among those who smoke more cigarettes per day and express greater quit motivation.27,28 Indeed, uptake rates may reflect quit motivation.29 Finally, although Internet use among Americans has reached 75%,30 issues of frequency of access and comfort with the Internet may also modify engagement.31
Second, it is vital to assess whether individuals can make informed decisions using a web-based approach. An informed decision is defined as “one that is based on relevant knowledge, consistent with the decision-maker's values and behaviorally implemented.”32 In other words, the decisions to log on to the website and to be tested should be related to one's attitudes toward testing. Further, the web-based content should provide an adequate knowledge base and result in a choice that is concordant with an individual's attitudes. Concordance would be defined as a match between one's attitude and the behavioral outcome (positive attitudes/logged on/tested and negative attitudes/did not log on/not tested).33 Decisions that reflect either poor knowledge and/or reflect discordance between attitudes and behavior would be less informed.33. Informed decision outcomes present a very important hurdle, as a trained professional is not present to counsel the individual unless proactively sought. Thus, the extent to which those who consider testing via a web-based modality can make informed decisions during this process would be one indicator of the potential feasibility of this approach.
Based on all the aforementioned considerations, we offered access to a web-based protocol that provided information regarding lung cancer susceptibility and offered GSTM1 testing to blood relatives of patients with late-stage lung cancer. This design allowed for the incorporation of the emotional and motivational salience of a family member's diagnosis with a method that could counter the challenge of geographic distance that could deter involvement of family members from receiving smoking cessation or genetic services. We examined rates and predictors of accessing the web-based protocol and the extent to which those who were offered the opportunity to log on to this web-based protocol arrived at informed decisions related to testing. The purpose of this study is to assess the overall feasibility of this web-based modality.
MATERIALS AND METHODS
Eligibility
Participants were recruited for this study in tandem with a larger multi-site smoking cessation trial. Participants were patients with stage IIIB/IV lung cancer who were receiving care in the Thoracic Oncology Clinic at the H. Lee Moffitt Cancer Center and Research Institute and their adult blood relatives aged 18 to 55 who were smokers (relative-smokers). Relative-smokers were first- or second-degree blood relatives. Other eligibility criteria for relative-smokers included the following: smoking at least seven cigarettes in the past week and at least 100 in their lifetime, no current or previous diagnosis of cancer, access to and previous use of the Internet, a score lower than 14 on the Centers for Epidemiological Survey of Depression, and English speaking. These stringent criteria were selected to maximize the salience of the setting and the test offered, while also protecting participants. Specifically, the eligibility cutoff for the level of depressive symptoms was set low because of the stressful context of recruitment and the minimal nature of the genetic counseling offered in the intervention.
Recruitment and study procedures
Procedures were approved by the National Human Genome Research Institute (NHGRI) and the Moffitt and Duke Institutional Review Boards. Patients with lung cancer were identified through their providers and approached by a recruiter during their clinic visits to Moffitt's Thoracic Oncology Clinic. Patients were asked if they were willing to be contacted for a brief telephone survey about their general well-being and their relatives who smoke. Patients who agreed signed a consent form indicating their willingness to have their personal health information forwarded to Duke University. Within 1 week, a trained interviewer called the patient to complete a brief survey. Some patients' interviews were completed by a proxy who was either designated at the clinic before the call or when the patient was contacted for the telephone interview. As part of the survey, the patient or his/her proxy enumerated relatives who were current smokers, their names, current mailing addresses and telephone numbers, and were asked for permission to use this information to contact these relative-smokers.
Relative-smokers were sent a letter to inform them of the study, and they were provided a toll-free number to call to decline participation. Relatives who did not decline were contacted by a survey interviewer employed by Battelle Survey Research Associates and were asked to complete a 30-minute telephone survey. Relative-smokers who agreed and were deemed eligible were asked if they would be willing to participate in a study designed to learn about the beliefs and attitudes that relatives may have related to lung cancer risks, genetics, and genetic testing and how these might influence their desire to quit. Their participation would involve reviewing web-based information, and genetic testing would be offered free of charge, as would smoking cessation materials. Multiple members of the same family could participate.
Within 2 weeks, relative-smokers who agreed received a packet of information including a user ID and password, and were instructed to log onto the website to begin their participation. A study team at the NHGRI's Social and Behavioral Research Branch monitored web-based data collection of relative-smokers' information and provided genetic counseling services as needed.
Relative-smokers who logged onto the website were guided through a series of structured steps identified as Session 1. This included additional consenting information and an overview of study procedures. A click box was provided for the individual to indicate willingness to begin Session 1. To start, relative-smokers completed a brief pretest survey and were then guided through 21 consecutive pages of graphically displayed information about the role of smoking and genetics in the development of lung cancer. Topics covered included (in order presented): “How does lung cancer develop?” “What is harmful about cigarette smoke?” “How does genetics affect your risk of lung cancer?” “Pros to consider in deciding about genetic testing”; “Cons to consider in deciding about genetic testing”; “How can you lower your risk for lung cancer?” Pros to consider included the following: the result that gives you information about one of the ways your body may handle the chemicals in cigarette smoke that cause lung cancer; the results could motivate you to quit smoking; the test is simple and painless. The cons included the following: if you are found to be at higher genetic risk, the news could be distressing; the result may not motivate you to quit smoking; the result can only tell you whether your risk is higher or lower than average, not whether or not you will get lung cancer; the result will not tell you about your genetic risk for other diseases of smoking. The development and structure of web content was guided by theoretical models,34–37 clinical models of genetic services delivery, and the conceptualization that participants may be experiencing a “teachable moment” in the context of the patients' lung cancer diagnoses.38
Individuals could move back and forth within the presentation of information. After reviewing the information, the relative-smoker began a survey component of the Session and was not able to move back into the information section. As part of the survey section, participants were offered testing for the GSTM1 genotype. They could decide to accept, decline, or delay taking the free test. Those who agreed to be tested were sent a kit, a consent form, and instructions for collecting a buccal sample and were provided with postage-paid mailing. Two reminders (e-mail or mail) were sent to those who had not logged on for Session 1, timed to occur 1 and 3 weeks after their first notification to log on to the website. About 3 weeks after Session 1, relative-smokers were e-mailed and asked to return for Session 2 to receive their results. Participants would receive $50 each for completing measures at Sessions 1 and 2, regardless of whether they were tested.
Predictors: baseline telephone survey
Demographics
Participants provided demographic information at baseline, including age, race, gender, education, marital, and employment status.
Smoking characteristics
Participants were asked how much they wanted to quit smoking in the next 6 months, rated on a scale of 1 (not at all) to 7 (very much). They also provided information regarding their smoking behavior, including how many cigarettes they smoked in a typical day and how long after waking they waited to smoke their first cigarette. These items are used commonly to assess the level of nicotine addiction.39
Patient-related characteristics
Two items were used to assess the patient's overall health from the relative-smoker's perspective: How would you rate your relative's health right now? and How would you describe your relatives overall quality of life right now? Each was scored on a 1 to 5 scale (1 = excellent, 2 = good, 3 = fair, 4 = poor, 5 = deceased).
The mean of six items from the FACES II40 was used to assess the relative-smoker's perceptions of family cohesiveness in relation to the patient (e.g., You feel the patient and you have/had a relationship closer than most; the patient accepts/accepted you just as you are) scored on a 1 (strongly disagree) to 4 (strongly agree) scale. Internal consistency in the present study was high (Cronbach's α = 0.81).
Cognitive and emotional variables
Participants were asked two questions: “What do you think your risk of getting lung cancer is if you continue to smoke at your present level, ” with 1 = certain not to happen and 7 = certain to happen, and “How worried are you about getting lung cancer in your lifetime, ” with 1 = not at all worried and 5 = very worried.
Internet-related variables
Participants were asked one item to assess frequency of Internet use: How often do you access the Internet, with 1 = daily, 2 = weekly, 3 = monthly and 4 = never. Participants responding never were excluded from the study. Overall comfort was assessed using one item: In general, how comfortable do you feel using the Internet? scored on a 1 to 5 scale (1 = very comfortable, 5 = very uncomfortable). Two items assessed experience with Internet modalities: Have you sent and received email messages? Have you sent and received email attachments?
Cancer genetic testing awareness
We assessed awareness with the item before today, have you ever heard about genetic tests for cancer risks? with 1 = yes or 2 = no.
Outcomes
Logging on to the study website
Participants were considered to have logged on if they completed the Session 1 end-of-session online surveys.
General knowledge about genetics
In the baseline telephone survey, we assessed general knowledge about genetics using five true/false items: once a genetic marker for a disorder is found in a person the disorder can be prevented or cured; if a person has a genetic marker for a disorder, the person will always get the disorder; only mothers can pass on genetic disorders; people who have a genetic marker for a disease are unhealthy; and a person's health habits can influence whether or not their genes cause disease. Responses were summed to create an overall knowledge scale with high internal consistency (Cronbach's α = 0.82).
Knowledge about GSTM1
Immediately after receiving the information presented in the web-based module of Session 1, we assessed knowledge specific to GSTM1 testing using four true/false items: the GSTM1 enzyme acts by cleaning up chemicals in cigarette smoke; whether a person has the GSTM1 enzyme that cannot be changed because it is genetic; about 50% of people are missing the GSTM1 enzyme; and a GSTM1 test result can tell you about your risk for many cancers. Responses were summed to create an overall knowledge scale with high internal consistency (Cronbach's α = 0.71).
Attitudes about genetic testing
Overall attitudes about testing were assessed in the baseline survey using eight items: you would be too worried that you might carry a gene that would increase your chance of getting lung cancer; if you were at greater risk, you could make changes to lower your risk; you believe that being tested would help you get motivated to do things like quit smoking; you would just want to know; you are afraid you would be too upset if you had the gene that increased your chance of lung cancer; if you found out you had a gene that increased your chance of lung cancer, you would feel singled out; you are not sure if the test would be accurate; it's hard to believe that finding our your genetic test result would have any benefit to you, accompanied by a five-point scale labeled strongly disagree to strongly agree. Responses were summed to create an overall attitude scale with high internal consistency (Cronbach's α = 0.73). Knowledge and attitudes at baseline were uncorrelated (r = 0.10, P = 0.27).
Attitudes toward GSTM1 testing
In Session 1, attitudes about testing were measured using 13 items that assessed reasons that they would or would not be tested: The test is painless and simple, the result might motivate me to stop smoking if I find out I am at greater risk, I just want to know the result, I want to know what my chances are of getting lung cancer, there is no proof that missing the GSTM1 enzyme causes lung cancer, the results won't tell me about my risk for other diseases, I'm concerned the results might upset me, I do not want to get my test result online, I'm not sure the test would be accurate, I see no benefit in being tested, now is not a good time, I don't think the result would be helpful, if I find out I'm at high risk I would feel singled out, accompanied by a seven-point scale labeled not at all important to very important. Responses were summed to create an overall attitude scale with high internal consistency (Cronbach's α = 0.87). Again, knowledge and attitudes in Session 1 were uncorrelated (r = 0.09, P = 0.48).
Informed decision-making
We assessed the informed decision-making process in two stages using a process similar to that of Marteau and collegues.33,41 The first step was to examine primarily whether an individual's decision to seek more information via the web (i.e., log on) was concordant with his/her attitudes toward testing, and whether he/she had a basic level of understanding about genetics. The second step was to assess the rates of informed decisions about testing among those who viewed the web-based protocol.
Our informed decision-making construct has three components: knowledge (general, GSTM1-specific), attitude (general, GSTM1-specific), and decision outcomes (logging on, being tested). Similar to the categorizations described by Michie et al.,41 adequate knowledge was defined as providing correct answers to more than half of the items provided, and positive attitudes toward testing was indicated by an attitude scale score at or above the midpoint of the scale. Participants' responses to knowledge and attitude items along with decision outcomes were dichotomized as follows: adequate knowledge (1 => half correct, 0 = other), attitude positive (1 = midpoint or >, 0 = other), decision to log on (1 = yes, 0 = no), and decision to be tested (1 = yes, 0 = no). Concordance was defined as a fit between participants' attitude and decision (1,1 or 0,0). Cross-categorizing these three components in a process similar to that used by Marteau and colleagues yielded eight categories of informed decision-making.33,41 An informed decision is defined as either adequate knowledge/positive attitude/tested or adequate knowledge/negative attitude/not tested; all other categories are considered less informed.
Data analysis
We generated descriptive statistics to characterize the participants' sociodemographics. We conducted bivariate analyses to determine the relationships between our predictors and our outcome of logging on to the study website. Because multiple relative-smokers from the same family participated, leading to intercorrelated data, multivariate analyses accounted for aggregation of data by family membership by using multiple logistic regression with generalized estimating equations to identify independent predictors of test uptake.
RESULTS
Participants and response rate
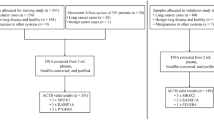
Recruitment for patients started in January 2005 at H. Lee Moffitt Cancer Center, Tampa Florida and ended in July 2006. As described in the study flowchart (see Fig. 1), 482 patients with late stage (IIIB/IV) lung cancer provided written consent to complete the patient survey. Nine patients were excluded due to being too ill or because they died before being contacted for the patient survey. Thirty-four refused to complete the survey at the time of contact, 44 were unable to be reached within the call window for the survey and four started but did not complete the survey. A total of 336 patients and 55 proxies completed the patient survey and gave permission to contact 539 of relative-smokers. Nine relative-smokers opted out of contact by calling the toll-free number. Telephone contact was attempted for 530 relative-smokers. Of these, we were unable to contact 165 by phone and 47 actively refused the baseline survey. A total of 304 (57.4%) completed the baseline survey; 180 were ineligible. Individuals who were ineligible were less likely to be employed (χ2 = 12.78, P < 0.001), expressed more negative attitudes about testing (t = 2.00, P < 0.05), and smoked significantly more cigarettes (t = 2.32, P < 0.05) than those who were eligible.

Participation flowchart.
Of the 124 eligible relative-smokers, 116 agreed to receive information about genetic testing that included log-in information. These 116 participants were from 95 unique families; 78 families included one relative-smoker, 13 families included two relative-smokers, and four families included three relative-smokers. Most of these participants were white (96%), married or living as married (66%), and employed full-time (72%); mean age was 38 years (range, 20–54). Fifty-three percent of the sample was female. On average, participants reported high quit motivation (mean = 6.0 on a 1–7 scale), high perceived risk (mean = 5.35 on a 1–7 scale), and worry (mean = 3.7 on a 1–5 scale) related to lung cancer regardless of whether they chose to log on to the study website; they rated the patient's health and quality of life to be fair and reported moderate family cohesion (mean = 3.4 on a scale of 1–5). Fifty-eight of the 116 (50%) logged on to the website and completed Session 1.
Characteristics associated with logging on
Table 1 depicts the characteristics of the 116 eligible participants who received login information, comparing those who logged on and those who did not log on. Those who logged on were significantly younger than those who did not (t = 2.10, P < 0.05). The only smoking-related variable to differentiate those who logged on from those who did not was quit motivation; those who logged on were significantly more likely than those who did not to state that they were motivated to quit in the next 6 months (t = 2.93, P < 0.01). The only Internet-related variable to differentiate these groups was daily Internet use; those who logged on were more likely to be daily Internet users (χ2 = 8.64, P < 0.05) than those who did not log on. Those who logged on also were more likely to have greater awareness of genetic tests for cancer risk (χ2 = 5.54, P < 0.05) than those who did not log on. There were no other group differences on demographic, cognitive, emotional, or patient-related variables. Variables that were significant at the bivariate level were entered into a logistic regression model using generalized estimating equations, accounting for the intraclass correlation related to including multiple members of the same family in the analysis. With the exception of age, which was not significant and was dropped from the final model, these same variables were significant in the final logistic model to predict logging on (see Table 2).
Informed decision outcome: logging on
The 116 participants were categorized into eight groups as to whether or not they made informed decisions to log on to the web-based protocol.33,41 As seen in Table 3, 48% (n = 55) of participants made an informed decision, with 25 making an informed decision to log on and 30 making an informed decision not to log on. The remaining 52% (n = 61) of the sample made less-informed decisions. The largest of these groups, and the largest group overall, consisted of participants inclined toward testing given adequate knowledge and positive attitudes, but who did not log on to consider testing (n = 36), followed by those who logged on having adequate knowledge, but whose negative attitudes toward testing would suggest that they should be disinclined to log on (n = 14).
We conducted post hoc tests examining which variables differentiated those who made more or less informed decisions to log on. Overall, participants whose decision to log on was concordant with attitudes and knowledge were younger than those whose decision was less concordant (F = 4.62, P < 0.05). Among participants whose knowledge and attitudes suggested that they would be interested in learning more about the genetic test, those who did not log on reported a significantly closer relationship to the patient compared with those who logged on (F = 5.59, P < 0.05). Among those whose knowledge and attitudes suggested that they should not be interested in genetic testing (i.e., had high knowledge but negative attitudes), those who logged on despite their negative attitudes toward testing were older (F = 7.12, P < 0.05) and more motivated to quit smoking (F = 5.05, P < 0.05) than those who expressed negative attitudes toward testing and did not log on.
Informed decision outcome: being tested
Additionally, the 58 participants who completed Session 1 of the web-based module were categorized into eight groups as to whether or not they made informed decisions to be tested, again with two categories grouped as “informed” (adequate knowledge/positive attitude/tested; adequate knowledge/negative attitude/not tested).32,33 The distribution of informed decision-making is presented in Table 4. Forty-eight percent (n = 28) of participants made an informed decision, with 21 making an informed decision to be tested and 7 making an informed decision not to be tested. The remaining 52% (n = 28) of the sample made less-informed decisions, including participants who were tested and had adequate knowledge, but whose negative attitudes toward testing were not concordant with their decision to be tested (n = 20), followed by those inclined toward testing given adequate knowledge and positive attitudes, but who were not tested (n = 4). Post hoc tests did not reveal any differences between those who made more or less informed decisions.
CONCLUSION
The vast majority of relatives of patients with late-stage lung cancer who were eligible to participate in the current study indicated interest in receiving web-based information about genetic testing. As a group, this sample expressed high motivation to quit smoking and reported Internet use patterns that are similar to those seen in the US population. However, only half of the smokers—all of whom had Internet access, comfort with the Internet, and had been offered an incentive—logged on to consider genetic susceptibility testing. Smokers who logged on expressed greater motivation to quit smoking, higher rates of daily Internet use, and greater awareness of cancer genetic testing. Although there was no evidence in the overall analysis that emotional factors inhibited engagement with the website, it is certainly possible that this context was not appropriate timing for these smokers.
Our finding that daily Internet use was a strong predictor of logging on was not surprising, though there may be a number of reasons that explain this finding. Frequency of use may be related to other important, unmeasured variables, such as comfort in conveying private information over the Internet. Many people are guarded about sharing genetic information, even with their relatives.42 Discomfort in having such private information conveyed over the web could be a deterrent for some and may be an issue for web-based modalities that should be considered more thoroughly in future research.
Motivation to quit smoking also emerged as a strong predictor of logging on, even in this motivated sample. This supports a previous suggestion that smokers who seek genetic tests are “self-selected.” Some may take genetic tests with specific intentions of using their result as a “motivational tool,” possibly regardless of the result itself.43 Alternatively, others may refuse uptake due to anticipated negative affect.44 A strong tendency for people to self-select themselves in or out of testing on the basis of their beliefs about their anticipated response to the test result has been observed in the clinical literature.45,46 The suggestion also is supported by some psychological theories, particularly those based on subjective expected utility theory,47,48 which argue that outcome expectancies—defined as an individual's expectations about the outcomes or consequences of the behavior—are among the strongest predictors of intentions to engage in specific behaviors. Although this seems intuitively obvious, the possibility of self-selection is mentioned infrequently in current debates about genetic testing for common diseases or gene variants and may play an important role as genetic tests move into the broader public sphere.
For assessing the quality of the decisions achieved with the web modality, we used Michie and Marteau's conception of informed decisions as a metric.33,41 About half of the participants in this study made informed choices both to log on and to be tested. Although this is lower than would be desirable, proportionately it does not differ from decisions made in the presence of a trained health professional.33 However, our results do suggest potential directions for future refinement of web-based modalities. The largest proportion of those whose attitudes and knowledge would have suggested they would have logged on but did not were emotionally closer to the lung cancer patient than those who had positive attitudes and did log on. This group's concerns, motives, and anticipated reactions to testing may mean they would have benefited from additional decision support via contact with a counselor or health care provider or different timing of the intervention as they may have been involved in the care of their relative.49,50 One of the potential advantages of a web-based protocol would be to offer services to those whose schedules (including their care-giving duties) do not enable them to attend group meetings or other programs. To this end, a web-based testing program could be used to triage individuals based on preference for testing and other behavioral assessments as a means for managing the limited resource of genetics-trained health professionals. These professionals could then focus their efforts on those who would most benefit from their services.
The other sizable group of the less-informed deciders included those who were disinclined toward testing based on attitudes and knowledge but logged on anyway. These individuals were older and more motivated to quit when compared with those who had negative attitudes and did not log on. It may be that older, more motivated smokers have turned to the current study as yet another attempt to find a magic bullet to motivate their cessation efforts.51 This is despite the fact that the study was not framed as a cessation intervention and participants were told that they would not be expected to quit smoking if they participated. Thus, the novelty of genetic susceptibility testing may have drawn these individuals to the web to consider testing.
There were no significant differences distinguishing those who made more or less informed decisions about testing, though 20 participants who expressed negative attitudes toward testing were tested and this discordance might have downstream implications for how individuals respond to testing.
Study limitations
The study had several limitations. Our results must be interpreted while considering some caveats related to our recruitment methods. Our stringent and conservative eligibility criteria excluded those who were older and experiencing greater levels of depressive symptomatology. Those excluded due to their depressive symptoms (n = 98) accounted for almost half of ineligible participants. Our exclusion of these individuals limits our ability to generalize the findings to smokers in general, many of whom express heightened depressive symptoms.52,53 However, it was prudent to exclude these individuals given our study's setting. With that said, levels of depressive symptoms among those who completed the baseline survey, including eligible and ineligible participants, were comparable with those found in many previous studies17,19 but lower than that found in others.54,55 Our study also does not provide a control or comparison group; we cannot know what rates of uptake or informed decision-making would have been had the participants been offered testing through a trained genetic counselor.
Our sample was similar to those of previous studies of lung cancer susceptibility feedback with regard to age, gender, and smoking status16–19,54,55 though as a group, they were slightly younger and more motivated to quit when compared with results found in previous studies.16–18,54,55 Our age cutoff of 55, significantly lower than the cutoff of 75 used in many of these studies, limited the mean age of the sample. Our rate of participation among racial or ethnic minority groups was lower than that found in previous studies. This is due to the demographics of those receiving care at our recruitment site, and not the web-based methodology, and as a result we cannot generalize to more diverse samples. We also are unable to address whether unmeasured variables, such as comfort in transmitting private information on the Internet or curiosity about the methodology, may have impacted log on rates. Finally, given the exploratory nature of the study, we were underpowered to detect some differences. Our findings should be viewed as preliminary and replicated in larger samples.
Conclusions
The results of the current study suggest that the use of Internet to offer genetic testing is a feasible modality that not only overcomes a number of logistical and service delivery challenges, but also may be appealing and support informed decision-making for a sizable sector of the public. However, not all would be well-served by this approach. Future research should build on these findings to refine decision-support approaches for different target audiences, contexts, and service triage. Such support could make better use of limited genetic services resources while facilitating better decision-making and appropriate use of genetic testing for common disease risk.
References
Guttmacher AE, Collins FS . Welcome to the genomic era. N Engl J Med 2003; 349: 996–998.
Wang C, Bowen DJ, Kardia SL . Research and practice opportunities at the intersection of health education, health behavior and genomics. Health Educ Behav 2005; 32: 686–701.
McClure JB . Are biomarkers a useful aid in smoking cessation? A review and analysis of the literature. Behav Med 2001; 27: 37–47.
Cobb NK, Graham AL, Bock BC, Papandonatos G, et al. Initial evaluation of a real-world Internet smoking cessation system. Nicotine Tob Res 2005; 7: 207–216.
Greendale K, Pyeritz RE . Empowering primary care health professionals in medical genetics: How soon? How fast? How far?. Am J Med Genet 2001; 106: 223–232.
Atienza AA, Hesse BW, Baker TB, Abrams DB, et al. Critical issues in eHealth research. Am J Prev Med 2007; 32: S71–S74.
Stone JH . Communication between physicians and patients in the era of E-medicine. N Engl J Med 2007; 356: 2451–2454.
Lobach DF, Detmer DE . Research challenges for electronic health records. Am J Prev Med 2007; 32: S104–S111.
Strange C, Dickson R, Carter C, Carpenter MJ, et al. Genetic testing for alpha1-antitrypsin deficiency. Genet Med 2004; 6: 204–210.
Carpenter MJ, Strange C, Jones Y, Dickson MR, et al. Does genetic testing result in behavioral health change? Changes in smoking behavior following testing for alpha-1 antitrypsin deficiency. Ann Behav Med 2007; 33: 22–28.
Green MJ, Peterson SK, Baker MW, Harper GR, et al. Effect of a computer-based decision aid on knowledge, perceptions, and intentions about genetic testing for breast cancer susceptibility: a randomized controlled trial. JAMA 2004; 292: 442–452.
Mannervik B . The isoenzymes of glutathione transferase. Adv Enzymol Relat Areas Mol Biol 1985; 57: 357–417.
Board P, Coggan M, Johnston P, Ross V, et al. Genetic heterogeneity of the human glutathione transferases: a complex of gene families. Pharmacol Ther 1990; 48: 357–369.
Houlston R . Glutathione S-transferase M1 status and lung cancer risk: a meta analysis. Cancer Epidemiol Biomarkers Prev 1999; 8: 675–682.
Benhamou S, Lee W, Alexandrie A, Boffetta P, et al. Meta- and pooled analyses of the effects of glutathione S-transferase MI polymorphisms and smoking on lung cancer risk. Carcinogenesis 2002; 23: 1343–1350.
McBride C, Halabi S, Bepler G, Lyna P, et al. Maximizing the motivational impact of feedback of lung cancer susceptibility on smokers' desire to quit. J Health Commun 2000; 5: 229–241.
Sanderson SC, Humphries SE, Hubbart C, Hughes E, et al. Psychological and behavioral impact of genetic testing smokers for lung cancer risk: a phase II exploratory trial. J Health Psychol. In press.
McBride C, Bepler G, Lipkus I, Lyna P, et al. Incorporating genetic susceptibility feedback into a smoking cessation program for African American smokers with low income. Cancer Epidemiol Biomarkers Prev 2002; 11: 521–528.
Lipkus IM, McBride CM, Pollak K, Lyna P, et al. Interpretation of genetic risk feedback among African American smokers with low socioeconomic status. Health Psychol 2004; 23: 178–188.
Coté ML, Kardia SL, Wenzlaff AS, Ruckdeschel JC, et al. Risk of lung cancer among white and black relatives of individuals with early-onset lung cancer. JAMA 2005; 293: 3036–3042.
Schwartz AG . Lung cancer: family history matters. Chest 2006; 130: 936–937.
Carter CL, Key J, Marsh L, Graves K . Contemporary perspectives in tobacco cessation: what oncologists need to know. Oncologist 2001; 6: 496–505.
Schilling A, Conaway MR, Wingate PJ, Atkins JN, et al. Recruiting cancer patients to participate in motivating their relatives to quit smoking. A cancer control study of the Cancer and Leukemia Group B (CALGB 9072). Cancer 1997; 79: 152–160.
Codori AM, Petersen GM, Miglioretti DL, Larkin EK, et al. Attitudes toward colon cancer gene testing: factors predicting test uptake. Cancer Epidemiol Biomarkers Prev 1999; 8: 345–351.
McBride CM, Pollak KI, Garst J, Keefe F, et al. Distress and motivation for smoking cessation among lung cancer patients' relatives who smoke. J Cancer Educ 2003; 18: 150–156.
Roberts JS, Barber M, Brown TM, Cupples LA, et al. Who seeks genetic testing for Alzheimer's disease? Findings from a multisite, randomized clinical trial. Genet Med 2004; 6: 197–203.
Ostroff JS, Buckshee N, Mancuso CA, Yankelevitz DF, et al. Smoking cessation following CT screening for early detection of lung cancer. Prev Med 2001; 33: 613–621.
Schnoll RA, Rothman RL, Lerman C, Miller SM, et al. Comparing cancer patients who enroll in a smoking cessation program at a comprehensive cancer center with those who decline enrollment. Head Neck 2004; 26: 278–286.
Sanderson SC, Wardle J . Will genetic testing for complex diseases increase motivation to quit smoking? Anticipated reactions in a survey of smokers. Health Educ Behav 2005; 32: 640–653.
Pew Foundation. Internet penetration and impact, 2006. Available at: www.pewinternet.org. Accessed June 27, 2007.
Lorence DP, Park H, Fox S . Assessing health consumerism on the Web: a demographic profile of information-seeking behaviors. J Med Syst 2006; 30: 251–258.
O'Connor AM, O'Brien Pallas LL, Decisional conflict. In: Mcfarlane GK, Mcfarlane EA, editors. Nursing diagnosis and intervention. Toronto:Mosby, 1989; 486–496.
Marteau TM, Dormandy E, Michie S . A measure of informed choice. Health Expect 2001; 4: 99–108.
Witte K, Allen M . A meta-analysis of fear appeals: implications for effective public health campaigns. Health Educ Behav 2000; 27: 591–615.
Petty RE, Cacioppo JT, The elaboration likelihood model of persuasion. In: Berkowitz L, editor. Advances in experimental social psychology. New York, NY: Academic Press 1986; 19: 123–205.
Ruiter RAC, Kok G, Verplanken B, Brug J . Evoked fear and effects of appeals on attitudes to performing breast self-examination: an information-processing perspective. Health Educ Res 2001; 16: 307–319.
Rogers RW . Cognitive and physiological processes in fear appeals and attitude change: a revised theory of protection motivation. In: Cacioppo JT, Petty RE, Social psychophysiology: a sourcebook. New York, NY: Guilford Press, 1983: 153–176.
McBride CM, Emmons K, Lipkus I . Understanding the potential of teachable moments for motivating smoking cessation. Health Educ Res 2003; 18: 156–170.
Heatherton TF, Kozlowski LT, Frecker RC, Fagerström KO . The Fagerstrom test for nicotine dependence: a revision of the Fagerstrom tolerance questionnaire. Br J Addict 1991; 86: 1119–1127.
Olson DH, Bell R, Porter J . FACES II: family adaptability and cohesion scale. St. Paul, MN: Family Social Science, University of Minnesota, 1982.
Michie S, Dormandy E, Marteau TM . The multi-dimensional measure of informed choice: a validation study. Patient Educ Couns 2002; 48: 87–91.
Henneman L, Timmermans DR, van der Wal G . Public experiences, knowledge and expectations about medical genetics and the use of genetic information. Community Genet 2004; 7: 33–43.
Sanderson SC, Wardle J . Associations between anticipated reactions to genetic test results and interest in genetic testing: will self-selection reduce the potential for harm? Genet Test. In press.
Codori AM, Hanson R, Brandt J . Self-selection in predictive testing for Huntington's disease. Am J Med Genet 1994; 54: 167–173.
Mastromauro C, Myers RH, Berkman B . Attitudes toward presymptomatic testing in Huntington's disease. Am J Med Genet 1987; 26: 271–282.
Decruyenaere M, Evers-Kiebooms G, Boogaerts A, Cloostermans T, et al. Nonparticipation in predictive testing for Huntington's disease: individual decision-making, personality and avoidant behavior in the family. Eur J Hum Genet 1997; 5: 351–363.
Edwards W . The theory of decision-making. Psychol Bull 1954; 51: 380–417.
Conner M, Norman P, editors. Predicting health behavior: research practice with social cognitive models. Buckingham: Open University Press, 1995.
Gaugler JE, Given WC, Linder J, Kataria R, et al. Work, gender and stress in family cancer caregiving. Support Care Cancer 2007. DOI: 10.1007/s00520–007-0331–2007.
Kim Y, Baker F, Spillers RL, Wellisch DK . Psychological adjustment of cancer caregivers with multiple roles. Psychooncology 2006; 15: 795–804.
Hammond D, McDonald PW, Fong GT, Borland R . Do smokers know how to quit? Knowledge and perceived effectiveness of cessation assistance as predictors of cessation behavior. Addiction 2004; 99: 1042–1048.
Hughes JR . Comorbidity and smoking. Nicotine Tob Res 1999; 1: S149–S152.
Johnson EO, Breslau N . Is the association of smoking and depression a recent phenomenon?. Nicotine Tob Res 2006; 8: 257–262.
Audrain J, Boyd NR, Roth J, Main D, et al. Genetic susceptibility testing in smoking-cessation treatment: one-year outcomes of a randomized trial. Addict Behav 1997; 22: 741–751.
Lerman C, Gold K, Audrain J, Lin TH, et al. Incorporating biomarkers of exposure and genetic susceptibility into smoking cessation treatment: effects on smoking-related cognitions, emotions, and behavior change. Health Psychol 1997; 16: 87–99.
Acknowledgements
This research was supported (in part) by the Intramural Research Program of the National Human Genome Research Institute, National Institutes of Health. This study was supported by grant U01CA092622 from the National Cancer Institute and NHGRI. Manuscript preparation was supported by the Battelle Shared Postdoctoral Fellowship. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NCI, NHGRI, or NIH. We thank the physicians and nurses of the H. Lee Moffitt Comprehensive Cancer Center and the NHGRI Bioinformatics Core for their assistance during the study and Cristopher Price for his statistical expertise. Most importantly, we thank the patients and their family members who participated in this study.
Author information
Authors and Affiliations
Corresponding author
Additional information
Disclosure: The authors declare no conflict of interest.
Rights and permissions
About this article
Cite this article
O'Neill, S., White, D., Sanderson, S. et al. The feasibility of online genetic testing for lung cancer susceptibility: uptake of a web-based protocol and decision outcomes. Genet Med 10, 121–130 (2008). https://doi.org/10.1097/GIM.0b013e31815f8e06
Received:
Accepted:
Issue date:
DOI: https://doi.org/10.1097/GIM.0b013e31815f8e06
Keywords
This article is cited by
-
A Genetic Lung Cancer Susceptibility Test may have a Positive Effect on Smoking Cessation
Journal of Genetic Counseling (2015)
-
Genetic Risk Assessment for Women with Epithelial Ovarian Cancer: Referral Patterns and Outcomes in a University Gynecologic Oncology Clinic
Journal of Genetic Counseling (2013)
-
Predictors of patient uptake of colorectal cancer gene environment risk assessment
Genome Medicine (2012)
-
Direct-to-consumer genomic testing: systematic review of the literature on user perspectives
European Journal of Human Genetics (2012)
