
Abstract
Purpose:
The purpose of this study was to compare health behaviors and cancer screening among Californians with and without a family history of cancer.
Methods:
We analyzed data from the 2005 California Health Interview Survey to ascertain cancer screening test use and to estimate the prevalence of health behaviors that may reduce the risk of cancer. We used logistic regression to control for demographic factors and health-care access.
Results:
Women with a family history of breast or ovarian cancer were more likely to be up to date with mammography as compared with women with no family history of cancer (odds ratio = 1.69, 95% confidence interval (1.39, 2.04)); their health behaviors were similar to other women. Men and women with a family history of colorectal cancer were more likely to be up to date with colorectal cancer screening as compared with individuals with no family history of cancer (odds ratio = 2.77, 95% confidence interval (2.20, 3.49)) but were less likely to have a body mass index <25 kg/m2 (odds ratio = 0.80, 95% confidence interval (0.67, 0.94)).
Conclusion:
Innovative methods are needed to encourage those with a moderate-to-strong familial risk for breast cancer and colorectal cancer to increase their physical activity levels, strive to maintain a healthy weight, quit smoking, and reduce alcohol use.
Genet Med 2013:15(3):212–221
Similar content being viewed by others

Introduction
Hereditary breast and ovarian cancer syndrome and Lynch syndrome increase individual risk for breast, ovarian, colorectal (CRC), and uterine cancers.1 Inherited mutations associated with these syndromes account for up to 10% of each of these cancers in the United States.1 In addition to these genetic syndromes, family medical history (FMH) is an established risk factor for blood relatives to develop the same or related cancers. Along with shared genetic risk factors, families may also share the same environment and exposures, and similar health behaviors, which lead to increased cancer risk.
Nearly 8% of people in the United States reported having a first-degree relative with a history of breast cancer, 7.1%, with a history of lung cancer, 5.0%, with a history of CRC, 4.7%, with a history of prostate cancer, and 1.8%, with a history of ovarian cancer.2 Having a first-degree relative with breast cancer increases an individual’s risk twofold.3 Similarly, having a first-degree relative diagnosed with CRC doubles a person’s risk.4 Convincing evidence demonstrates that alcohol consumption increases risk for both pre- and postmenopausal breast cancers5 and CRC.6 Obesity increases risk for CRC6 and endometrial7 and postmenopausal breast cancer.5 Regular physical activity is associated with a lower risk of colon cancer,8 and likely reduces risk for endometrial cancer7 and breast cancer in postmenopausal women.5 Tobacco use can increase risk for CRC,9 and may modestly increase breast cancer risk based on findings from recent large prospective cohort studies.10 Fruit and vegetable consumption5,11 and dietary intake of fat5 likely have little effect on breast cancer risk. Although fruit and vegetable consumption has not been consistently linked with CRC,11 consumption of red and processed meat may increase risk, whereas high-fiber diets may lower risk.6 Approximately 23% of CRC cases could be prevented through the combination of no smoking, regular physical activity, limiting alcohol use, and maintaining a healthy diet and waist circumference.12
Modification of dietary and lifestyle behaviors can reduce the risk of breast and CRC even in individuals with FMH of these cancers.13,14 Although cancer screening test use is higher in persons with FMH of CRC15,16 and breast cancer,16 less is known about their health behaviors at the population-level.17 In addition, few studies have addressed how FMH can be used to motivate individuals to adopt and maintain healthy lifestyles to reduce disease risk.18
The aim of this study was to examine health behaviors (maintenance of healthy weight, prudent alcohol use, regular physical activity, fruit and vegetable consumption, and no smoking) of Californians who report having one or more family members with a history of cancer (primarily in first-degree relatives) as compared with health behaviors of individuals who report no FMH of cancer in a first-degree relative, with emphasis on family history of breast or ovarian cancers, CRCs, and FMH of early-onset cancer in a first-degree relative. CRC and breast cancer screening test use is also compared among these individuals. We used the 2005 California Health Interview Survey (CHIS), a population-based survey, to examine these factors.
Materials and Methods
Data source
Adult and family health history public-use data files of the 2005 CHIS (the most current data at the time this study was conducted) were obtained. CHIS is a population-based, random-digit-dialed telephone survey conducted every 2 years with noninstitutionalized California resident households to obtain information on health behaviors, health-care access, insurance coverage, health status, and a variety of other health-related topics. The CHIS uses a two-stage geographically stratified sampling design, and interviews are conducted in five languages to reach California’s diverse population. More information on CHIS methodology can be obtained at http://www.chis.ucla.edu/designs-methods.html. In 2005, more than 45,000 households participated in the CHIS, with an overall household response rate of 29.5%. This response rate is based on the American Association for Public Opinion Research’s overall response rate definition, which includes partially completed questionnaires (http://www.chis.ucla.edu/pdf/CHIS2005_method4.pdf).
In the 2005 CHIS adult survey, Californians aged 18–64 years were asked about their FMH of any cancer among first-degree (mother, father, brother(s), sister(s), and children) and second-degree (grandparents, aunts, and uncles) relatives. Distinctions were made between half and full siblings. For each affected family member, respondents were asked about the specific type of cancer (breast, ovarian, uterine/endometrial, or colon/rectal for female family members, and breast, colon/rectal, or prostate cancer for male family members) and if the affected family member was under age 50 years at the time of his or her diagnosis.
Inclusion criteria
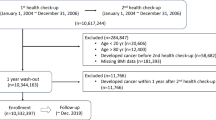
The adult CHIS public-use dataset included 43,020 adults. We excluded 9,833 adults aged >65 years because they were not asked about their FMH of cancer. We excluded an additional 2,501 respondents because they had a personal history of any cancer and 426 additional respondents who did not know if they had a first-degree family member with a history of cancer. This left 30,260 respondents for the analysis.
We created indicator variables ( Table 1 ) based on responses to the FMH module regarding type of cancer and the affected family member to classify respondents who would be at moderate-to-strong risk for cancer based on their FMH profile (degree of relation, number, and age of affected relatives): (i) any family history of cancer (primarily in a first-degree relative); or (ii) FMH of CRC; (iii) FMH of breast or ovarian cancer; and (iv) FMH history of CRC, breast, prostate, ovarian, or endometrial cancer in a first-degree relative diagnosed under age 50 (i.e., early onset), which included examining the subpopulations of FMH of CRC and breast or ovarian cancer separately in descriptive analyses only. We included ovarian cancer history and second-degree relatives in the same lineage to better classify women at moderate-to-strong risk for developing familial breast cancer.19 Of 18,501 respondents with no FMH of cancer in a first-degree relative, 251 women had female breast or ovarian cancer in two or more second-degree relatives in the same lineage or a second-degree male relative with breast cancer, and 83 respondents without a first-degree relative diagnosed with cancer had two or more second-degree relatives in the same lineage with CRC.
These respondents with FMH of breast, ovarian, or CRC were grouped with respondents having a first-degree relative with cancer. This left 12,026 respondents with an FMH of cancer, and 18,234 without.
Variables and statistical analysis
We examined the following demographic or health-care access variables: sex, age group, race/ethnicity (based on race/ethnic group respondent most identified with), household income, education level, health insurance coverage, marital status, general health condition, having a condition that substantially limits one or more basic physical activities, and having a usual place to go when sick or in need of health advice. We included the following health behaviors: eating five or more servings of fruits and vegetables/day (marker of a healthy diet/weight management aid),20 regular physical activity (20 min of vigorous physical activity 3 days or more in the past week or 30 min of moderate physical activity 5 days or more in the past week), smoking status (current, former/never smoked regularly), binge drinking in the past month (5 drinks or more per occasion for men and 4 or more drinks per occasion for women), and self-reported body mass index (underweight/normal: <25.0 kg/m2, overweight/obese: 25.0 kg/m2 or higher).
Respondents were considered up to date with cancer screening tests if they were screened according to 2005 United States Preventive Services Task Force guidelines. We classified respondents aged 50 years and older as being up to date with CRC screening if at least one of the following conditions were met: fecal occult blood test received within the past year, sigmoidoscopy within the past 5 years, or colonoscopy within the past 10 years. Women aged 40 years and older were considered up to date with screening for breast cancer if they had received mammography within the past 2 years. For women who were up to date with mammography screening, we examined the reason women provided for receiving their last mammogram. For men and women aged 40 years and older with FMH of CRC, we also assessed receipt of colonoscopy within the past 5 years and receipt of any CRC screening test within appropriate time intervals for average-risk individuals because more stringent screening is recommended in this population.21 Because women with FMH profiles of early-onset breast or ovarian cancer may be encouraged to initiate breast cancer screening at an earlier age than average-risk women,22 we examined the prevalence of women aged 30 years and older receiving a mammogram within the past year.
We used SAS v9.2 (SAS Institute, Cary, NC) and SAS callable SUDAAN release 10 (Research Triangle Institute, Research Triangle Park, NC) to conduct all analyses to account for the complex sampling design of CHIS. In both the descriptive and multivariate logistic regression analyses, the jackknife method was used to calculate variance, because replicate weights were provided to accurately calculate variance due to the complex sampling design of the CHIS. All estimates were weighted to produce population estimates that account for the probability of selection and factors associated with survey design and administration (e.g., nonresponse and under-coverage due to lack of a residential landline).
We conducted a descriptive analysis comparing respondents with each of the different FMHs of cancer profiles with persons without an FMH of cancer, to obtain percentages and standard errors on demographic characteristics, health behaviors of interest, and cancer screening test use. P values were obtained from Rao–Scott χ2 tests. We conducted a multivariate logistic regression analysis, building separate logistic regression models with the following seven outcomes as dichotomous variables (yes vs. no): (i) eating five or more servings of fruits and vegetables per day; (ii) engaging in regular physical activity; (iii) not a current smoker; (iv) body mass index <25.0 kg/m2; (v) no alcoholic binge drinking in the past month (i.e., the month preceding survey) and (vi) up to date with CRC screening and (vii) breast cancer screening. Models were run separately for any FMH of cancer, FMH of breast or ovarian cancer (women only), FMH of CRC, and FMH of early-onset cancer in a first-degree relative to obtain odds ratios (ORs) and 95% confidence intervals (CIs) for the outcomes of interest adjusted for demographic characteristics and health-care access. The referent group in all models was respondents without an FMH of cancer. We used a backwards-elimination approach to eliminate nonsignificant (P > 0.05) covariates from all models (with the exception of age, race/ethnicity, and having a usual health-care provider). Covariates initially included in the health behavior models were age, sex (except for the FMH of breast or ovarian cancer model), race/ethnicity, household income, health insurance status, education level, having a usual health-care provider, having a condition that substantially limits one or more basic physical activities, marital status, and general health status. Covariates initially included in the cancer screening models were: age, race/ethnicity, household income, health insurance status, education level, having a usual health care provider, marital status, and sex (CRC screening models).
Results
Prevalence of FMH of cancer was higher among women, older age groups, and more educated, higher-income individuals ( Table 2 ). Non-Latino whites and American Indians/Alaska Natives (42.8 and 37.5%, respectively) reported a higher prevalence of any FMH of cancer, whereas Asian/Pacific Islanders and Latinos had the lowest prevalence (22.1 and 17.6%, respectively; P < 0.0001). Prevalence of FMH of cancer was more often reported by individuals with health-care coverage and who had a usual health-care provider.
Nearly 45% of men and women with an FMH of CRC consumed five or more servings of fruits and vegetables per day as compared with 49.5% of men and women without an FMH of cancer ( Table 3 ; P = 0.0057). After adjustment for demographic characteristics and health-care access, men and women with an FMH of CRC were 16% less likely to consume five or more servings of fruits and vegetables per day (OR = 0.84, 95% CI (0.73, 0.96)). After adjustment for demographic characteristics and health-care access in multivariate models, no significant differences were found for binge drinking. Men and women with an FMH of any cancer had lower rates of a body mass index <25.0 kg/m2 as compared with men and women with no FMH of cancer (42.6 vs. 45.7%, respectively; P = 0.0001); results are similar for persons with an FMH of CRC (39.4%; P = 0.0011) and an FMH of early-onset cancer (41.6%; P = 0.0074). After adjustment for demographic characteristics and health-care access, men and women with an FMH of any cancer were 9% less likely to report being normal/underweight as compared with persons without an FMH of cancer (OR = 0.91, 95% CI (0.85, 0.98)), and men and women with an FMH of CRC were 20% less likely to report being normal/underweight (OR = 0.80; 95% CI (0.67, 0.94)).
Among men and women aged 50 years and older with an FMH of CRC, 71.5% were up to date with CRC screening, as compared with 44.5% of persons without an FMH of cancer (P < 0.0001). After adjustment for demographic characteristics and health-care access, men and women with an FMH of CRC were nearly 2.8 times more likely to be up to date (OR = 2.77; 95% CI (2.20, 3.49)), whereas persons with an FMH of any cancer and persons with an FMH of early-onset cancer were more likely to be up to date as compared with persons without an FMH of cancer (OR = 1.33, 95% CI (1.17, 1.51) and OR = 1.37, 95% CI (1.12, 1.66), respectively). Nearly 58% of men and women aged 40–64 years with an FMH of CRC and 53% with an FMH of early-onset CRC were up to date at screening intervals recommended for the average-risk population (P < 0.0001 and P < 0.0001, respectively). Among this age group, 42.0% of persons with an FMH of early-onset CRC had received a colonoscopy within the past 5 years (P < 0.0001). These findings were nearly identical to all persons with an FMH of CRC.
Although women with an FMH of breast or ovarian cancer reported higher levels of regular physical activity, lower rates of not being a current smoker, and lower rates of normal/underweight status as compared with women without an FMH of cancer, these differences for physical activity, smoking status, and weight disappeared after adjustment for demographic characteristics and health-care access ( Table 4 ).
Eighty-five percent of women aged 40–64 years with an FMH of breast or ovarian cancer had received a mammogram within the past 2 years, as compared with 73.7% of women without an FMH of cancer (P < 0.0001). After adjustment for demographic characteristics and health-care access, women with an FMH of breast or ovarian cancer were nearly 1.7 times more likely to be up to date as compared with women without an FMH of cancer (OR = 1.69, 95% CI (1.39, 2.04)). Among women aged 30–64 years who had received a mammogram within the past 2 years, 33.2% of women with an FMH of breast or ovarian cancer and 41.7% with an FMH of early-onset breast or ovarian cancer reported that the reason for the test was due to family history, as compared with 2.6% of women with no FMH of any cancer (P < 0.0001). Younger women (aged 30–49 years) more frequently reported family history as a reason for the test than older women (data not shown). Fifty-six percent of women aged 30–64 years with an FMH of early-onset breast or ovarian cancer had received a mammogram within the past year (P < 0.0001). Rates were highest among women aged 50–59 years (78.7%) as compared with women aged 30–39 years and 40–49 years (28.4 and 55.5%, respectively; data not shown).
Discussion
In this large, population-based study, we found that men and women with an FMH of CRC were less likely to maintain a healthy weight and consume five or more servings of fruits and vegetables per day (which increases risk for CRC), than those without an FMH of cancer. Conversely, we found that men and women with an FMH of cancer were more likely to be up to date with cancer screenings than those without. To our knowledge, these weight-related findings are some of the first to be presented for individuals with an FMH of cancer. In addition, our study, being one of only a few that is population-based, strengthens the literature on all health behaviors and cancer screenings in those with an FMH of cancer.
Although our findings on weight among individuals with an FMH of CRC appear to be novel, our health behavior findings on physical activity and alcohol use are generally similar to those from other recent studies.17,23 In our study, women with an FMH of breast or ovarian cancer had health behaviors similar to women without an FMH of cancer. Other studies have found similar results,24,25 although some studies have found more intense or higher levels of physical activity in women with a family history of breast cancer,26,27,28 or greater practice of health behaviors was observed, as compared with the general population.26 In some of these studies, data were drawn on women of higher education or socioeconomic status;26,28 therefore, these findings may not be generalizable to other populations, including ours.
Taken together, our health behavior findings indicate that there may be missed opportunities to improve the health of a population that is at increased risk of cancer. FMH of cancer represents a complex interaction between genes and environment. Because only a small fraction of cancer cases are attributable to hereditary syndromes, clinicians should consider health behavior counseling when they encounter patients with FMH of cancer because they may be exhibiting the same negative behaviors that likely contributed to their relative’s cancer. Studies have shown that persons with an FMH of breast or CRC are more likely to receive recommendations from health-care providers to improve health behaviors, but the overall number receiving these recommendations may be low.17,29 In one study, women with an FMH of breast cancer were more likely to report making one or more health behavior changes because of a recently diagnosed first-degree relative.30 Persons with an FMH of CRC may also be willing to make health behavior changes and to follow through,17 but awareness of risk factors for CRC may be low.31 In addition, awareness of an FMH of cancer may not always translate into positive health behaviors. Conversely, it may place too much emphasis on genetic susceptibility.32 In this study, we were unable to assess if our study findings were due to a lack of awareness of risk factors for breast and CRC. Regardless, patients with an FMH of cancer may benefit from a targeted approach to improving their health behaviors. Findings from the Family Healthware Impact trial indicate modest increases in physical activity levels after a targeted intervention.33
Results from our cancer screening analysis showed that women with an FMH of breast or ovarian cancer were nearly 1.7 times more likely to be up to date with mammography screening as compared with women without an FMH of cancer, but nearly 15% were not up to date with recommendations for women at average risk for breast cancer. Although men and women with an FMH of CRC were 2.8 times more likely to be recently screened as compared with men and women without an FMH of cancer, nearly 29% were not currently up to date with recommendations for average-risk individuals. Nearly 42% of women with an FMH of early-onset breast or ovarian cancer reported that the reason for their last mammogram was due to an FMH of cancer. Although sample sizes were small, we found this varied considerably by age. Younger women more frequently reported family history as a reason as compared with older women. Our findings of increased cancer screening test use among Californians with an FMH of cancer are similar to those of other studies that examined this.15,16 These findings indicate that many patients and their health-care providers recognize the increased risk conferred by an FMH of cancer. However, screening for CRC is suboptimal for men and women with an FMH of early-onset CRC; 58% had not received a colonoscopy within the past 5 years. Although having an FMH of cancer did increase the odds of breast and CRC screening, a considerable portion of individuals in our study with an FMH of early-onset CRC or breast or ovarian cancer were not appropriately screened considering their FMH profile. Although sample sizes were small, only 28% of women aged 30–39 years with an FMH of early-onset breast or ovarian cancer had received a mammogram within the past year (data not shown). These study findings may be due in part to the challenges of collecting FMH of cancer in the clinical setting. Primary-care clinicians are often the first health-care providers to ascertain family health histories and refer patients for cancer screening.34 Barriers to collecting the FMH include lack of time,18,34 limited tools for use in primary care,34 concerns about validity of self-reported FMH,35 and lack of clear guidelines to assist in collecting, interpreting, and using FMH for disease risk management.36 Some investigators have indicated that the accuracy of self-reports of FMH of cancer may be improved if tools rather than interviews are used,34 and if information is collected outside of clinical visits, where it could be checked with relatives.35 The US Surgeon General’s family health history initiative encourages Americans to learn more about their family’s health history, and a computerized tool is available to record family health information (available at http://www.hhs.gov/familyhistory/). Guidelines on how to systematically assess risk of cancer or use the information to guide prevention efforts are limited, but some resources are available to providers. The American Medical Association provides resources and tools to assist providers in collecting histories (available at http://www.ama-assn.org/ama/pub/physician-resources/medical-science/genetics-molecular-medicine/family-history.page?). As electronic medical records are increasingly adopted by primary-care physicians, existing tools must be able to interface or be integrated into these systems. However, electronic medical records may allow more extensive FMHs to be assembled more easily.37
This study is subject to some limitations. Currently, standardized definitions do not exist for moderate and high-risk FMH of cancer profiles, so some respondents may have been misclassified. CHIS is a cross-sectional telephone survey, so self-reported demographic, health behavior, FMH, and cancer screening information may all be subject to social desirability bias. FMH of cancer was not verified against medical records or cancer registry data, so under- or over-reporting was possible, and this likely occurred with endometrial cancer, which is not reported as accurately as other cancer sites.38 Foreign-born status may partially explain racial and ethnic differences in reporting FMH of cancer.39 However, accurate self-reporting of family history of cancer in first-degree relatives for CRC and breast and prostate cancer is high.38 Our results for California are not generalizable to the overall US population. Because we examined seven different outcomes for several different cancer FMH profiles, some findings may be due to chance alone. Despite these limitations, few population-based surveys collect data on FMH of cancer that includes age of onset and second-degree relatives. CHIS is a large health survey from a racially and ethnically diverse population; therefore, most of our analyses were not constrained by small sample sizes.
Conclusion
Individuals with an FMH of CRC or breast or ovarian cancer are at higher risk of developing these same cancers and would benefit from adopting healthier lifestyles that may reduce their own cancer risk. Innovative methods may be needed by California health-care providers to raise awareness of behavioral risk factors and motivate these individuals to adopt healthier lifestyles.
Disclosure
The authors declare no conflict of interest.
References
Shulman LP . Hereditary breast and ovarian cancer (HBOC): clinical features and counseling for BRCA1 and BRCA2, Lynch syndrome, Cowden syndrome, and Li-Fraumeni syndrome. Obstet Gyn Clin North Am 2010;37:109–133.
Ramsey SD, Yoon P, Moonesinghe R, Khoury MJ . Population-based study of the prevalence of family history of cancer: implications for cancer screening and prevention. Genet Med 2006;8:571–575.
Pharoah PD, Day NE, Duffy S, Easton DF, Ponder BA . Family history and the risk of breast cancer: a systematic review and meta-analysis. Int J Cancer 1997;71:800–809.
Butterworth AS, Higgins JP, Pharoah P . Relative and absolute risk of colorectal cancer for individuals with a family history: a meta-analysis. Eur J Cancer 2006;42:216–227.
World Cancer Research Fund/American Institute for Cancer Research. Continuous Update Project Report Summary. Food, Nutrition, Physical Activity, and the Prevention of Breast Cancer. World Cancer Research Fund International: London, 2008.
World Cancer Research Fund/American Institute for Cancer Research. WCRF/AICR Systematic Literature Review Continuous Update Project Report: The Associations Between Food, Nutrition and Physical Activity and the Risk of Colorectal Cancer. World Cancer Research Fund International: London, 2010.
World Cancer Research Fund/American Institute for Cancer Research. Food, Nutrition, Physical Activity, and the Prevention of Cancer: A Global Perspective. American Institute for Cancer Research: Washington, DC, 2007.
Wolin KY, Yan Y, Colditz GA, Lee IM . Physical activity and colon cancer prevention: a meta-analysis. Br J Cancer 2009;100:611–616.
Botteri E, Iodice S, Bagnardi V, Raimondi S, Lowenfels AB, Maisonneuve P . Smoking and colorectal cancer: a meta-analysis. JAMA 2008;300:2765–2778.
Xue F, Willett WC, Rosner BA, Hankinson SE, Michels KB . Cigarette smoking and the incidence of breast cancer. Arch Intern Med 2011;171:125–133.
Key TJ . Fruit and vegetables and cancer risk. Br J Cancer 2011;104:6–11.
Kirkegaard H, Johnsen NF, Christensen J, Frederiksen K, Overvad K, Tjønneland A . Association of adherence to lifestyle recommendations and risk of colorectal cancer: a prospective Danish cohort study. BMJ 2010;341:c5504.
Slattery ML, Levin TR, Ma K, Goldgar D, Holubkov R, Edwards S . Family history and colorectal cancer: predictors of risk. Cancer Causes Control 2003;14:879–887.
Gramling R, Lash TL, Rothman KJ, et al. Family history of later-onset breast cancer, breast healthy behavior and invasive breast cancer among postmenopausal women: a cohort study. Breast Cancer Res 2010;12:R82.
Beydoun HA, Beydoun MA . Predictors of colorectal cancer screening behaviors among average-risk older adults in the United States. Cancer Causes Control 2008;19:339–359.
Shah M, Zhu K, Palmer RC, Jatoi I, Shriver C, Wu H . Breast, colorectal, and skin cancer screening practices and family history of cancer in U.S. women. J Womens Health (Larchmt) 2007;16:526–534.
Zlot AI, Silvey K, Newell N, Coates RJ, Leman R . Family history of colorectal cancer: clinicians’ preventive recommendations and patient behavior. Prev Chronic Dis 2012;9:E21.
Claassen L, Henneman L, Janssens AC, et al. Using family history information to promote healthy lifestyles and prevent diseases; a discussion of the evidence. BMC Public Health 2010;10:248.
Scheuner MT, McNeel TS, Freedman AN . Population prevalence of familial cancer and common hereditary cancer syndromes. The 2005 California Health Interview Survey. Genet Med 2010;12:726–735.
Rolls BJ, Ello-Martin JA, Tohill BC . What can intervention studies tell us about the relationship between fruit and vegetable consumption and weight management? Nutr Rev 2004;62:1–17.
Levin B, Lieberman DA, McFarland B, et al.; American Cancer Society Colorectal Cancer Advisory Group; US Multi-Society Task Force; American College of Radiology Colon Cancer Committee. Screening and surveillance for the early detection of colorectal cancer and adenomatous polyps, 2008: a joint guideline from the American Cancer Society, the US Multi-Society Task Force on Colorectal Cancer, and the American College of Radiology. CA Cancer J Clin 2008;58:130–160.
Saslow D, Boetes C, Burke W, et al.; American Cancer Society Breast Cancer Advisory Group. American Cancer Society guidelines for breast screening with MRI as an adjunct to mammography. CA Cancer J Clin 2007;57:75–89.
Burton AM, Peterson SK, Marani SK, et al. Health and lifestyle behaviors among persons at risk of Lynch syndrome. Cancer Causes Control 2010;21:513–521.
Madlensky L, Vierkant RA, Vachon CM, et al. Preventive health behaviors and familial breast cancer. Cancer Epidemiol Biomarkers Prev 2005;14:2340–2345.
Spector D, Deroo LA, Sandler DP . Lifestyle behaviors in black and white women with a family history of breast cancer. Prev Med 2011;52:394–397.
Emmons KM, Kalkbrenner KJ, Klar N, Light T, Schneider KA, Garber JE . Behavioral risk factors among women presenting for genetic testing. Cancer Epidemiol Biomarkers Prev 2000;9:89–94.
Audrain J, Schwartz M, Herrera J, Goldman P, Bush A . Physical activity in first-degree relatives of breast cancer patients. J Behav Med 2001;24:587–603.
Ochoa EM, Gómez-Acebo I, Rodríguez-Cundín P, Navarro-Córdoba M, Llorca J, Dierssen-Sotos T . Relationship between family history of breast cancer and health-related behavior. Behav Med 2010;36:123–129.
Zlot AI, Cox SL, Silvey K, Leman R . The effect of chronic disease family history on healthcare provider practice and patient behavior among Oregonians. Public Health Genomics 2012;15:189–200.
Lemon SC, Zapka JG, Clemow L . Health behavior change among women with recent familial diagnosis of breast cancer. Prev Med 2004;39:253–262.
Akhtar S, Sinha S, McKenzie S, Sagar PM, Finan PJ, Burke D . Awareness of risk factors amongst first degree relative patients with colorectal cancer. Colorectal Dis 2008;10:887–890.
O’Neill SC, McBride CM, Alford SH, Kaphingst KA . Preferences for genetic and behavioral health information: the impact of risk factors and disease attributions. Ann Behav Med 2010;40:127–137.
Ruffin MT, Nease DE, Jr ., Sen A, et al. Effect of preventive messages tailored to family history on health behaviors: the Family Healthware Impact Trial. Ann Fam Med 2011;9:3–11.
Qureshi N, Wilson B, Santaguida P, Carroll J, Allanson J, Culebro CR, Brouwers M, Raina P . Collection and Use of Cancer Family History in Primary Care: Evidence Report/Technology Assessment No. 159. Agency for Healthcare Research and Quality: Rockville, MD, 2007.
Murf HJ, Syngal S . Does this patient have a family history of cancer? An evidence-based analysis of the accuracy of family cancer history. JAMA 2004;292:1480–1489.
Wood ME, Stockdale A, Flynn BS . Interviews with primary care physicians regarding taking and interpreting the cancer family history. Fam Pract 2008;25:334–340.
Qureshi N, Wilson B, Santaguida P, et al. Family history and improving health. Evid Rep Technol Assess (Full Rep) 2009;186:1–135.
Ziogas A, Anton-Culver H . Validation of family history data in cancer family registries. Am J Prev Med 2003;24:190–198.
Orom H, Coté ML, González HM, Underwood W 3rd, Schwartz AG . Family history of cancer: is it an accurate indicator of cancer risk in the immigrant population? Cancer 2008;112:399–406.
Acknowledgements
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Townsend, J., Steele, C., Richardson, L. et al. Health behaviors and cancer screening among Californians with a family history of cancer. Genet Med 15, 212–221 (2013). https://doi.org/10.1038/gim.2012.118
Received:
Accepted:
Published:
Issue date:
DOI: https://doi.org/10.1038/gim.2012.118
Keywords
This article is cited by
-
First-degree relatives of cancer patients: a target group for primary prevention? A cross-sectional study
British Journal of Cancer (2018)
-
Lifestyle Risk Factors for Breast Cancer in BRCA1/2‐Mutation Carriers Around Childbearing Age
Journal of Genetic Counseling (2017)
-
Risque moyen ou élevé de cancer colorectal : comment classer en 2014 ? Faut-il changer le paradigme ?
Acta Endoscopica (2014)
-
Risque de néoplasie rectocolique en cas d’antécédent familial de carcinome ou d’adénome rectocolique. Faut-il revoir les recommandations de dépistage en 2014 ?
Acta Endoscopica (2014)
-
Associations among family history of cancer, cancer screening and lifestyle behaviors: a population-based study
Cancer Causes & Control (2013)
