
Abstract
Overweight and obesity are less closely associated with idiopathic intracranial hypertension (IIH) in young children than in post-pubescent children and adults. We examined the hypothesis that being overweight or obese (body mass index (BMI) ⩾85th percentile) in children is a risk factor for IIH recurrence. A total of 43 children with IIH who were followed up for an average of 9±3.4 years were evaluated in a retrospective case–control series. The rate of IIH recurrence was compared between children of healthy weight and children presenting with overweight or obesity, using survival curve analysis. The overall risk for long-term IIH recurrence in children is ~20%. Following weight stratification, the risk for IIH recurrence in our cohort was fivefold higher in children with a BMI ⩾85th percentile (57%) than in healthy weight children (11%; log-rank test P=0.04). Pediatricians may consider counseling families that weight control may be a means of decreasing the risk of IIH recurrence.
Similar content being viewed by others

Introduction
Pediatric idiopathic intracranial hypertension (IIH) is typically treated by a multidisciplinary team of neurologists, neuro-ophthalmologists and pediatricians. Obesity is a well-known risk factor for IIH in adults1,2 and has also been shown to be important in post-pubertal/adolescent children.3, 4, 5 In pre-pubertal children, however, IIH is less closely associated with being overweight or obese.3,6 Parents of children with pediatric IIH often enquire about the prognosis and rate of recurrence. The risk of IIH recurrence in adults is reported to be closely associated with obesity.6,7 Recurrence of IIH seems to occur in 20% of children,3,8 but data regarding childhood overweight and increased risk of IIH recurrence are lacking.
Materials and methods
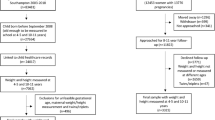
We conducted a long-term retrospective case–control study of children younger than 18 years of age who had IIH to determine the correlation between being overweight or obese (body mass index (BMI) ⩾85th percentile) and the rate of IIH recurrence and visual loss. The study was initiated following Institutional Review Board's approval. A total of 45 children (<18 years of age) who met the updated modified Dandy criteria for IIH9 were seen at our neuro-ophthalmology clinic between 2001 and 2003. Children with non-idiopathic or drug-induced (for example, steroid, minocycline or isotretinoin) intracranial hypertension were excluded. The rate of IIH recurrence was compared between children presenting with healthy weight at the time of IIH diagnosis (as defined by the BMI and BMI percentile calculator for children and teens)10 and those who were overweight or obese at presentation using Kaplan–Meier survival curve analysis, with patients stratified by BMI percentile. Follow-up BMI and BMI percentiles were collected from their pediatrician’s charts and from the children’s health maintenance organization (HMO) growth charts. Change in BMI percentile over the study period was assessed using a continuous paired analysis test. The primary outcome measure was an episode of recurrence, defined as a new onset of disease symptoms or papilledema occurring after remission that also met the modified Dandy criteria. Repeat lumbar puncture and neuroimaging were performed in all cases of recurrence. Remission was defined as a symptom-free period of at least 12 months, without papilledema and without medical treatment. A poor visual outcome was defined as one eye with best-corrected visual acuity of 20/200 or visual field constriction to <20° central.1
Results
The mean age (s.d.) of the 43 pediatric IIH patients for whom long-term neuro-ophthalmologic follow-up and body weight measurement data were available at diagnosis was 11 (4.5) years, with a mean (s.d.) follow-up of 9 (3.4) years. Eighteen patients were ⩽11 years old at presentation. Table 1 lists patient characteristics, listing subjects with recurrence at the top of the table. BMI data were available at presentation for all subjects, and at follow-up in all recurrent cases and in 79% of patients without recurrence. A total of 24 of the 43 pediatric IIH patients (56%) had a BMI ⩾85th percentile at presentation, indicating they were overweight or obese, whereas 19 patients (44%) presented with a BMI indicative of a healthy weight.
All patients presented with papilledema and symptoms typical of IIH. Intracranial opening pressure at presentation ranged between 250 and 400 mm of water (mean (s.d.)=300 (10) mm of water). IIH recurred in 8 of the 43 patients (19%), 7 of whom had a BMI⩾85th percentile (7 of the 23 (30%) subjects with obesity related IIH had recurrence). The cumulative incidence of recurrence among children with a BMI <85th percentile was 11%, compared with 57% among those with a BMI ⩾85th percentile (log-rank test, P=0.04; see Figure 1).

Life-table analysis of the cumulative incidence of IIH recurrence in children with a BMI ⩾85th percentile compared with a BMI <85th percentile.
During follow-up period, BMI percentile increased insignificantly from 93.62 to 95.5 (P=0.403) and from 71.55 to 75.48 (P=0.438) both among recurrent (n=8) and nonrecurrent (n=29) cases, respectively.
Poor visual outcome occurred in six patients with a BMI <85th percentile (5.3%) and five patients with a BMI ⩾85th percentile (20.8%; P=0.3).
Discussion
This study of 43 children with IIH who were followed up for over 6 years revealed that the risk of IIH recurrence is significantly (fivefold) higher in overweight or obese children than healthy weight children. Children with IIH recurrence continued to be overweight or obese, whereas nonrecurrent cases continued with more healthy body mass despite a nonsignificant trend of increase in BMI percentile in both groups. The majority of adult IIH patients (for whom the recurrence rate is high) tend to be overweight, whereas only 56% of the children in the cohort examined in this study had a BMI ⩾85th percentile. The low prevalence of pediatric IIH does not facilitate large prospective or long-term follow-up studies. Despite the retrospective design of this study, the very long-term follow-up (~9 years) of this series provides important information to attending pediatricians that underscores the impact of weight on the risk of IIH recurrence in children. A possible reason for the significant difference in IIH recurrence rates between overweight or obese children and healthy weight children may be that overweight or obese children with IIH represent a population in which the disease is similar to adult IIH, whereas healthy weight children constitute a different IIH subgroup. We excluded non-idiopathic intracranial hypertension cases such as those that were drug-induced (for example, due to minocycline, isotretinoin, steroids, growth hormone and so on) and those that were related to venous thrombosis. The grouping of findings from both idiopathic and drug-induced intracranial hypertension cases, as has been done in other studies,11,12 may mask the association between weight and intracranial hypertension recurrence in children, as drug-induced intracranial hypertension tends not to recur once the offending drug is discontinued.
Our study examined whether overweight is a risk for IIH recurrence, and thus differs from the large cohort study conducted by Brara et al.,4 which estimated the impact of being overweight on the risk for developing IIH. Szewka et al.1 commented that although the findings of the study by Brara et al. underscore the similarity between adult IIH and the disease in post-pubertal children, weight appears to have less of an effect in younger, pre-pubertal children. Although no observational study can show causality, our study shows a probable link between overweight and IIH recurrence, even in young children with IIH. Forty-two percent of our study population was younger than 11 years of age, as opposed to only 15% of the patients in the study by Brara et al.
The 9-year follow-up, the exclusion of non-idiopathic intracranial hypertension, and the fact that our study population was composed of equal numbers of pre- and post-pubertal IIH patients indicate that being overweight or obese has an important role in a less-addressed aspect of long-term prognosis: the recurrence rate. The overall risk of IIH recurrence over the long term in our cohort of children was 19%. Following weight stratification, the risk was fivefold (57%) greater in children with a BMI ⩾85th percentile compared with healthy weight children (11%). The results of our study suggest that pediatricians could have a crucial role in decreasing the risk of IIH recurrence by counseling families on the importance of weight control.
References
Szewka AJ, Bruce BB, Newman NJ, Biousse V . Pediatric idiopathic intracranial hypertension and extreme childhood obesity: a comment on visual outcomes. J Pediatr 2012; 161: 972.
Biousse V, Bruce BB, Newman NJ . Update on the pathophysiology and management of idiopathic intracranial hypertension. J Neurol Neurosurg Psychiatry 2012; 83: 488–494.
Tibussek D, Distelmaier F, von Kries R, Mayatepek E . Pseudotumor cerebri in childhood and adolescence — results of a Germany-wide ESPED-survey. Klin Padiatr 2013; 225: 81–85.
Brara SM, Koebnick C, Porter AH, Langer-Gould A . Pediatric idiopathic intracranial hypertension and extreme childhood obesity. J Pediatr 2012; 161: 602–607.
Balcer LJ, Liu GT, Forman S, Pun K, Volpe NJ, Galetta SL et al. Idiopathic intracranial hypertension: relation of age and obesity in children. Neurology 1999; 52: 870–872.
Babikian P, Corbett J, Bell W . Idiopathic intracranial hypertension in children: the Iowa experience. J Child Neurol 1994; 9: 144–149.
Pollak L, Zohar E, Glovinsky Y, Huna-Baron R . Reevaluation of presentation and course of idiopathic intracranial hypertension - a large cohort comprehensive study. Acta Neurol Scand 2013; 127: 406–412.
Tibussek D, Schneider DT, Vandemeulebroecke N, Turowski B, Messing-Juenger M, Willems PH et al. Clinical spectrum of the pseudotumor cerebri complex in children. Childs Nerv Syst 2010; 26: 313–321.
Friedman DI, Jacobson DM . Diagnostic criteria for idiopathic intracranial hypertension. Neurology 2002; 59: 1492–1495.
Center for Disease Control and Prevention. BMI percentile calculator for child and teen. English version. At: http://apps.nccd.cdc.gov/dnpabmi/.
Soiberman U, Stolovitch C, Balcer LJ, Regenbogen M, Constantini S, Kesler A . Idiopathic intracranial hypertension in children: visual outcome and risk of recurrence. Childs Nerv Syst 2011; 27: 1913–1918.
Honorat R, Marchandot J, Tison C, Cances C, Chaix Y . Treatment and prognosis of idiopathic intracranial hypertension in children. Retrospective study (1995–2009) and literature review. Arch Pediatr 2011; 18: 1139–1147.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article
Cite this article
Stiebel-Kalish, H., Serov, I., Sella, R. et al. Childhood overweight or obesity increases the risk of IIH recurrence fivefold. Int J Obes 38, 1475–1477 (2014). https://doi.org/10.1038/ijo.2014.44
Received:
Revised:
Accepted:
Published:
Issue date:
DOI: https://doi.org/10.1038/ijo.2014.44
Keywords
This article is cited by
-
Diagnosis, treatment and prevention of pediatric obesity: consensus position statement of the Italian Society for Pediatric Endocrinology and Diabetology and the Italian Society of Pediatrics
Italian Journal of Pediatrics (2018)
-
An update on idiopathic intracranial hypertension
Acta Neurochirurgica (2017)
