
Abstract
Background
Evidence on the age-dependent association between adiposity and risk of dementia in the Chinese population is unclear. We aim to disentangle the association of mid- and late- life adiposity with subsequent dementia risk in Chinese adults and compare ageing trajectories of adiposity between those with/out dementia.
Methods
Dementia was ascertained based on cognitive batteries and the Activity of Daily Living Scale in the China Health and Retirement Longitudinal Study (CHARLS). Adiposity was measured by body mass index (BMI), waist circumference (WC), and waist-to-height ratio (WtHR). We estimated hazard ratio (HR) of adiposity for incident dementia by age groups (i.e. 50–64, and ≥65). Age trajectories of adiposity measures were fitted using a mixed-effect model in a case-control design. The interaction terms of age and dementia were included to examine the difference between cases and controls.
Results
Hazard ratios (HRs) for incident dementia in two age groups (50–64 and ≥65) were estimated in 13,355 participants. Raised mid-life BMI was associated with incident dementia (HR (95% CI): overweight 1.33 (1.03 to 1.73), obesity 1.63 (1.17 to 2.28)). Mid-life abdominal obesity was associated with incident dementia (WC 1.45 (1.15 to 1.84), WtHR 1.44 (1.08 to 1.94)), accounting for ≤24.2% of dementia cases. Among participants developing dementia, adiposity measures were higher in mid-life and declined faster with age, compared to those remaining dementia-free. Late-life adiposity was not associated with dementia risk.
Conclusion
Mid-life but not late-life adiposity was associated with dementia incidence in China. Accelerated weight loss in prodromal dementia is likely to explain the mixed evidence on adiposity and dementia risk in the Chinese population. Rapid decline in adiposity in later life may be an early sign. Reducing mid-life adiposity in the population may mitigate the future dementia burden.
Similar content being viewed by others

Introduction
The Chinese population continues to age rapidly, with a fast-rising number of dementia cases [1]. Evidence from high-income countries indicates that as many as 40% of cases can be prevented or delayed through targeting modifiable risk factors [2]. Mid-life obesity may be responsible for 16% of Chinese dementia cases, given its high and increasing prevalence in the population [3, 4].
Systematic reviews and meta-analysis based on research from high-income countries indicates that obesity but not being overweight was associated with late-life dementia [2, 5]. However, current evidence on the association between adiposity and risk of dementia in the Chinese population is inconsistent. Studies of adiposity in later life (65+ years), suggest underweight is a risk factor for dementia (Supplementary Table 1). One cohort study with a baseline in mid-life (45+ years) concluded that higher general and abdominal adiposity is protective for cognitive decline [6]. Uncertainty remains whether the age-dependent association between adiposity and dementia in high-income countries [7, 8] can be generalized to China. Furthermore, to assess excess body fat and its associated disease risks, lower body mass index (BMI) and waist circumference (WC) have been suggested for Asians compared to Europeans [9]. The age-specific association between adiposity and dementia may vary by ethnicity, due to variations in genetics, living environments and wider socioeconomic contexts, and requires further study in diverse populations [10].
Weight loss appears to be a feature of the long preclinical phase of dementia development [11,12,13]. Age-based trajectories of BMI and central adiposity measures by dementia status would illuminate our understanding of the age-dependent association in the Chinese context [14].
We hypothesize that (1) high BMI, WC, and waist-to-height ratio (WtHR) in mid-life, but not later life, are associated with raised subsequent dementia incidence; and (2) that age trajectories of BMI, WC and WtHR differ between those developing dementia and matched controls free of dementia over follow-up, reflecting increased weight loss with age of people in the preclinical phase of dementia. Further, we quantified the proportion of dementia cases that attribute to high BMI, WC, and WtHR by estimating the corresponding population attributable fraction (PAF) tailored to Chinese population.
Subjects and method
Study design and participants
This study used nationally representative panel data from four waves (in 2011, 2013, 2015, and 2018) of the China Health and Retirement Longitudinal Study (CHARLS). CHARLS is a national survey of a representative sample of Chinese population aged 45 years and older. The response rates were over 80% for each wave. Data on sociodemographic, lifestyle, health status, and clinical measurements were collected with standardized questionnaire and physical examination. Details about the study design of the CHARLS have been previously reported [15].
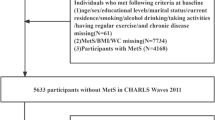
We selected data from CHARLS participants aged ≥50 years, and used the first height, weight and WC measurements as baseline. Participants with dementia at baseline (n = 525) or were missing covariates (n = 3495) at 2011 were excluded. Refreshment samples at CHARLS wave 2 (n = 866) and wave 3 (n = 1215) were selected using the same criteria. The detailed selection process is shown in Fig. 1, rending 13,355 for the analysis sample with 623 dementia cases.

Flow diagram of study participants.
Assessment of dementia
Dementia was defined as the coexistence of functional impairment and cognitive impairment, or self-reported, doctor-diagnosed dementia or memory-related diseases. The definition conforms to Diagnostic and Statistical Manual of Mental Disorders (DSM)-5 and International Classification of Diseases 10th edition (ICD-10) for dementia, which has been validated against a nationwide population-based survey [16]. Doctor-diagnosed memory-related diseases were identified by the item “Have you been diagnosed with memory-related diseases?” [15]. This information was used to identify cases among participants without cognitive scores (32%) [17].
Functional impairment was assessed by the Katz-scale in CHARLS [18]. Participants who required caregiving for one or more basic activities of daily living (bathing, getting in or out of bed, changing clothes, using toilet, cutting food and eating, controlling urination and bowel movement) were defined as functional impairment. Participants who reported functional impairment once but fully recovered to perform these activities independently in all subsequent waves, were not identified as having functional impairment.
Cognitive impairment was assessed using the Telephone Interview for Cognitive Status questionnaire (TICS), administered via face-to-face interviews across all CHARLS waves [15]. The 9-item TICS is a modified version of Mini-Mental State Examination, examined cognitive domains (i.e. orientation to time, memory, visuo-construction and attention) with a summary score ranging from 0-31 [19]. We previously derived three latent cognitive factors, namely orientation, memory, executive function and language, via confirmatory factor analysis based on TICS data from CHARLS [16]. Participants with two or more domains of impairment were defined as cognitive impairment. Domain-specific impairment was quantified as corresponding cognitive factor score of 1.5 standard deviations below the population mean of same education level. Participants with improved cognition by more than 1 standard deviation in two or more domains at the subsequent wave, were not identified as having cognitive impairment.
Assessment of adiposity
Referring to the national criteria for adult weight set by the National Health and Family Planning Commission of the People’s Republic of China, BMI was categorized into four groups: underweight (BMI < 18.5 kg/m2), normal weight (BMI = 18.5 kg/m2 to 24 kg/m2), overweight (BMI = 24 kg/m2 to 28 kg/m2), and obesity (BMI ≥ 28 kg/m2) [20]. To account for visceral excess fat distribution, WC and WtHR were also used to determined abdominal obesity [21, 22]. According to the national criteria and previous studies, WC was divided into two group: non-abdominal obesity (WC < 90 cm for male or <85 cm for female) and abdominal obesity (WC ≥ 90 cm for male or ≥85 cm for female) [20]. WtHR was divided into two group: on-abdominal obesity (WtHR < 0.5) and abdominal obesity (WtHR ≥ 0.5) [23]. Weight and height was measured in bare feet with the participant standing erect. WC was measured with the participants in standing position at the level of navel [15].
Covariates
Sociodemographic characteristics included baseline age, sex, and education level. Lifestyle included smoking frequency and drinking frequency. Education level was categorised as low education level (0 year), middle education level (1–6 years), and high education level (7 years or higher) [24]. Smoking frequency was measured by cigarettes / day. Drinking frequency was categorised into none, less than once per day, once per day, twice per day, and more than twice per day.
Statistical analysis
Following previous study and the National Bureau of Statistics [25, 26], A Cox proportional hazard model was used to separately test the age-specific (50–64 years and ≥65 years) association between each adiposity measure and subsequent dementia adjusting for sociodemographic characteristics, and lifestyle factors. To avoid over-adjustment, potential mediators in the etiological pathways such as cardiovascular disease and diabetes [27], were not adjusted in the model.
Mixed models were used to explore how the trajectory of adiposity measures with age differed between those with subsequent dementia and those without. To account for age, sex, education, and the period effect in the measures and dementia, as well as the effects of selection bias and loss to follow-up, one dementia case was matched with four controls using the MatchIt package [28], based on baseline age, sex, education, year of inclusion and follow-up duration. The trajectories were modelled as a function of spline age to allow nonlinear trend [29]. To examine the differences in aging effect between cases and controls, dementia and its interaction with spline age were included. For ease of interpretation of the model coefficients, baseline age was centred at 65 years so that the coefficient of dementia indicated the difference in these measurements in the early old ages and birth year was centred at 1945. Due to the small number of dementia incidence and short follow-up under 60 (n = 169, 27%), trajectories were fitted only for those aged over 60 at baseline to avoid overfitting. Model selection was based on Akaike information criterion (AIC), Bayesian information criterion (BIC) and Wald test.
To quantify the impact on population of adiposity, PAF was interpreted as the proportion of dementia risk that could be eliminated. PAF was calculated based on Miettinen’s formula, where pc is the prevalence of risk in the cases and HRadj is the adjusted hazard ratio [30].
The prevalence was estimated using CHARLS and considering individual weight with household and individual non-response adjustment. To compare with Mukadam’s report [3], the prevalence was calculated aiming the same age group.
Sensitivity analyses were conducted by excluding dementia events that occurred at the adjacent wave after baseline to reduce the impact of reverse causation of weight loss.
All statistical analysis was performed with R (version 4.2.3).
Role of the funding source
The funders of the study had no role in study design, data collection, data analysis, data interpretation, or writing of the report, or in the decision to submit the paper for publication.
Ethics approval and consent to participate
The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guideline was followed [31]. All participants provided informed consent. CHARLS was approved by the Ethical Review Committee of Peking University (ethical approval number: IRB00001052-11015).
Results
Table 1 summary the follow-up, baseline demographics, adiposity measures, smoking frequency, and drinking frequency in the total population (N = 13,355) and in cases (N = 623) and control groups (N = 3115). In the 50–64 years group, compared with the no dementia group, those developed dementia during follow-up were older (mean baseline age 58.6 vs. 57.5) and had higher adiposity measures, and drank less. However, measures of adiposity were not different between dementia and no dementia group in the other age group. All measures of obesity were lower in the mid-life matched control group, but not different in the late-life group.
(Table 1. Baseline characteristics of participants in CHARLS by dementia).
A total of 31.8% participants were overweight and 12.2% had obesity in mid-life. Overweight (HR = 1.41 (1.08 to 1.82)) and obesity (HR = 1.76 (1.26 to 2.46)) were associated with higher risk of dementia in mid-life but not in older-age (overweight: HR = 1.07 (0.82 to 1.40), obesity: HR = 1.14 (0.74 to 1.75)). The analyses were underpowered to examine the effect of underweight on dementia. Further adjustment for smoking and drinking did not attenuate the association (overweight: HR = 1.41 (1.09 to 1.83), obesity: HR = 1.77 (1.26 to 2.47)). The association between abdominal obesity in mid-life and dementia was similar to obesity (measured by WC: HR = 1.56 (1.23 to 1.98), measured by WtHR: HR = 1.55 (1.16 to 2.08)). All covariates were analysed in the study, and details were presented in the Supplementary Table 2–4. Sensitivity analysis based on follow-up did not alter the association significantly and was presented in Supplementary Table 5.
(Table 2. Association of BMI, WC, and WtHR in different age group with dementia).
The trajectory of BMI with age was different in the case group compared with the control group (Fig. 2A). Those with dementia had higher BMI at 60 years and accelerated decline in later life. The BMI declined more slowly with age for those without dementia and was higher than demented patients after 78 years. The trajectory of WC (Fig. 2B) with age was similar to that of WtHR (Fig. 2C), which increased in mid-life and declined in later life. The changes of trajectories between cases and controls were close to that of BMI. Those with dementia had higher WC and WtHR in mid-life but experienced accelerated decline with aging, which was lower than the control group at 76 years and 80 years. Details of all mixed effect models for the trajectories were in Supplementary Table 3.

A Trajectory of BMI with age in the dementia group (cases) compared with the non-dementia group (controls). B Trajectory of waist circumference with age in the dementia group (cases) compared with the non-dementia group (controls). C Trajectory of waist-to-height ratio with age in the dementia group (cases) compared with the non-dementia group (controls). Trajectory of adiposity measures with age by dementia (cases) and non-dementia (controls) *Bands indicate 95% CI. BMI body mass index. **Baseline age, sex, education, year of inclusion, and follow-up duration were matched. ***Due to very few cases, trajectories were fitted only for those aged over 60 at baseline to avoid overfitting.
Furthermore, we estimated that 10.5%, 5.1%, 17.2%, 24.2% of dementia would be due to overweight, obesity, abdominal obesity measured by WC and WtHR in the future. Details of PAF estimation were in Table 3.
(Table 3. PAF of overweight, obesity, and abdominal obesity for dementia).
Discussion
Utilizing nationwide ageing cohort spanning over eight years, our study confirmed that mid- but not late-life adiposity was associated with increased risk of subsequent dementia in Chinese population, accounting for up to 24% of future dementia cases. Moreover, we revealed that those who developed dementia had higher adiposity measures in mid-life but declined faster with age than their cognitive healthy counterparts. To our best knowledge, we are the first study clarifying the age-dependent association of adiposity and dementia risk in the Chinese population, which has been mixed and largely overlooked previously [32,33,34,35].
Our finding on the positive associations between mid-life obesity, abdominal obesity and dementia incidence are in line with evidence in high-income countries [36,37,38]. Additionally, we found that mid-life overweight also increased risk of dementia, which was not found in American and European population [38]. This association may result from a high proportion of abdominal obesity among Chinese overweight, while about one-third in the westerners [39]. In our study, 75.9% of mid-life overweight participants were found to have abdominal obesity, and the relation between abdominal obesity and visceral adipose tissue has been widely reported [40]. Such that for a given BMI, higher concentrations of visceral adipose tissue, which are associated with metabolic risks [41], are more commonly seen in Chinese population than their Western counterparts [42]. A recent study using structural equation modelling suggests that metabolic consequences of adiposity- such as diabetes, hypertension and cardiovascular disease- may mediate the relationship between adiposity and cognitive decline [27]. Accordingly, our analysis was adjusted only for baseline sociodemographic and lifestyle factors to avoid over-adjustment. Our finding is further supported by a latest Mendelian randomization study in Singapore, which verified a causal relationship between increased visceral adiposity and reduced cognition among 6099 Chinese mid-aged (mean age 51.9) adults [43].
Our updated PAFs of several adiposity measures further indicated the vital role of abdominal obesity. As such 17–24% new dementia cases may be avoided if abdominal obesity can be controlled, about 50% larger than prior estimates [3]. Our trajectories reveal that participants from later birth cohorts had higher average adiposity measures, corresponded to previous evidence [44]. The increasing trends in mid-life abdominal obesity across generations underscored the importance of early prevention and intervention in adiposity across Chinese population.
We did not find any statistically significant association of degree of adiposity, including underweight, in late-life with dementia incidence. This observation differs from prior findings that link late-life underweight with a high risk of dementia and cognitive impairment, based on the Shanghai Ageing Study [34] and the Chinese Longitudinal Healthy Longevity Survey [45]. The proportion of participants aged 80+ in these two studies was at least twice as many as in CHARLS, which at present lacks power to detect possible increased dementia risk linked to low adiposity. Reverse causation, namely accelerated weight loss and declining abdominal obesity as a result of prodromal dementia, is likely to take place progressively from early old age and to continue into late old age [7]. Our analysis of the age-trajectory of adiposity between participants who develop dementia and those who remain dementia-free lends support to this proposition. The trajectories show that participants who developed dementia had higher adiposity measures in mid-life, which dropped faster as they aged, and around 80 years, their adiposity measures became lower than their cognitively healthy counterparts.
Moreover, the differences in age-related decline rate of BMI between dementia and non-dementia people in China were 1.5 times than those of their American and European counterparts [12, 13]. Besides ethnic variations of weight change, sociocultural factors may also contribute to this huge disparity [46, 47]. Awareness and knowledge about dementia is generally low among Chinese public [48] and health personnel [49], rending large number of undiagnosed and untreated individuals hiding in community [50]. Once identified, those with dementia are more likely to be in later stages, experiencing faster and irreversible health deterioration such like weight loss. Thus, timely cognitive impairment screening should be introduced to high-risk middle-aged adults with overweight and obesity, combined with continue monitoring on their weight and cognitive function change over years.
Using nationally representative aging cohort in China, our study disentangled the association of mid- and late-life adiposity with subsequent dementia risk in Chinese adults and compare aging trajectories of adiposity between those with/out dementia, which broaden the evidence to another ethnicity. Nevertheless, limitations should be noted. First, dementia was not diagnosed by neurologist. However, this algorithmic definition is standard practice in population-based cohorts with limited resources and has been validated against survey with clinical diagnosis [16]. Besides, the maximum follow-up in our study was seven years, which was relatively short compared to relevant studies (over 10 years). Limited by the follow-up time, we cannot fully assess the association between mid-life adiposity and later-life dementia at this stage because 83.1% of the dementia cases for the middle-aged group were identified at age 60 and above, with 56.9% of them occurring at age over 65 (Supplementary Fig. 1). Our trajectories of adiposity measures were anchored by age but not time to dementia. This may not be the best way to characterize weight loss in prodromal dementia [29]. Future studies with longer follow-up fitted these trajectories by year before dementia, would facilitate the understanding of the long-term association and the identification of when and how much weight is lost before dementia onset following the etiologic stage. Last, our PAFs rely on the assumption that the distribution of other dementia risk factors remains constant. The assumption may result in underestimation because adiposity also increases the risk of other dementia risk factors (e.g., cardiovascular diseases). However, this does not undermine the value of preventing mid-life abdominal obesity based on the relative importance of the three different adiposity measures.
In conclusion, our study disentangles the association of mid- and late-life adiposity with subsequent dementia risk in Chinese adults. Mid-life adiposity is associated with dementia in Chinese population, which may cause up to 24.2% dementia cases in the future. The adiposity measures with age in those develop dementia are significantly different for those cognitive intact. Our findings provide evidence for the importance of weight management and monitoring since in mid-life to meet the challenge of dementia in China.
Data availability
The datasets analysed during the current study are available on https://charls.pku.edu.cn/.
References
Alzheimer’s Disease International, M.U. World Alzheimer Report 2015. 2015. https://www.alzint.org/resource/world-alzheimer-report-2015/
Livingston G, Huntley J, Sommerlad A, Ames D, Ballard C, Banerjee S, et al. Dementia prevention, intervention, and care: 2020 report of the Lancet Commission. Lancet. 2020;396:413–46. https://doi.org/10.1016/S0140-6736(20)30367-6
Mukadam N, Sommerlad A, Huntley J, Livingston G. Population attributable fractions for risk factors for dementia in low-income and middle-income countries: an analysis using cross-sectional survey data. Lancet Glob Health. 2019;7:e596–e603. https://doi.org/10.1016/S2214-109X(19)30074-9
Wang Y, Zhao L, Gao L, Pan A, Xue H. Health policy and public health implications of obesity in China. Lancet Diabetes Endocrinol. 2021;9:446–61. https://doi.org/10.1016/S2213-8587(21)00118-2
Kivimäki M, Luukkonen R, Batty GD, Ferrie JE, Pentti J, Nyberg ST, et al. Body mass index and risk of dementia: analysis of individual-level data from 1.3 million individuals. Alzheimer’s Dementia. 2018;14:601–9. https://doi.org/10.1016/j.jalz.2017.09.016
Zhang J, Tang G, Xie H, Wang B, He M, Fu J, et al. Higher adiposity is associated with slower cognitive decline in hypertensive patients: secondary analysis of the China stroke primary prevention trial. J Am Heart Assoc. Oct 2017;6. https://doi.org/10.1161/jaha.117.005561
Luchsinger JA, Patel B, Tang MX, Schupf N, Mayeux R. Measures of adiposity and dementia risk in elderly persons. Arch Neurol. 2007;64:392–8. https://doi.org/10.1001/archneur.64.3.392
Whitmer RA, Gunderson EP, Barrett-Connor E, Quesenberry CP Jr, Yaffe K. Obesity in middle age and future risk of dementia: a 27 year longitudinal population based study. BMJ. 2005;330:1360. https://doi.org/10.1136/bmj.38446.466238.E0
WHO Expert Consultation. Appropriate body-mass index in Asian populations and its implications for policy and intervention strategies. (vol 363, pg 157, 2004). Lancet. 2004;363:902.
Nianogo RA, Rosenwohl-Mack A, Yaffe K, Carrasco A, Hoffmann CM, Barnes DE. Risk factors associated with Alzheimer disease and related dementias by sex and race and ethnicity in the US. Jama Neurology. 2022;79:584–91. https://doi.org/10.1001/jamaneurol.2022.0976
Jack CR Jr, Knopman DS, Jagust WJ, Petersen RC, Weiner MW, Aisen PS, et al. Tracking pathophysiological processes in Alzheimer’s disease: an updated hypothetical model of dynamic biomarkers. Lancet Neurol. 2013;12:207–16. https://doi.org/10.1016/S1474-4422(12)70291-0
Bäckman K, Joas E, Waern M, Östling S, Guo X, Blennow K, et al. 37 years of body mass index and dementia: effect modification by the APOE genotype: observations from the prospective population study of women in Gothenburg, Sweden. J Alzheimers Dis. 2015;48:1119–27. https://doi.org/10.3233/jad-150326
Suemoto CK, Gilsanz P, Mayeda ER, Glymour MM. Body mass index and cognitive function: the potential for reverse causation. Int J Obes. 2015;39:1383–9. https://doi.org/10.1038/ijo.2015.83
Gustafson D. Adiposity indices and dementia. Lancet Neurology. 2006;5:713–20. https://doi.org/10.1016/s1474-4422(06)70526-9
Zhao YH, Hu YS, Smith JP, Strauss J, Yang GH. Cohort profile: the China health and retirement longitudinal study (CHARLS). Int J Epidemiol. 2014;43:61–68. https://doi.org/10.1093/ije/dys203
Liu YY, Wu YJ, Cai JH, Huang Y, Chen YT, Venkatraman TM, et al. Is there a common latent cognitive construct for dementia estimation across two Chinese cohorts? Alzheimer’s & Dementia: Diagnosis, Assessment & Disease Monitoring. 2022;14. https://doi.org/10.1002/dad2.12356
Liu Y, Wu Y, Chen Y, Lobanov-Rostovsky S, Liu Y, Zeng M, et al. Projection for dementia burden in China to 2050: a macro-simulation study by scenarios of dementia incidence trends. Lancet Regional Health Western Pacific. 2024;50:101158. https://doi.org/10.1016/j.lanwpc.2024.101158
Katz S, Downs TD, Cash HR, Grotz RC.Progress in development of the index of ADL.Gerontologist. 1970;10:20–30. https://doi.org/10.1093/geront/10.1_part_1.20
Brandt J, Spencer M, Folstein M. The telephone interview for cognitive status. Cogn Behav Neurol. 1988;1:111–8.
National Health and Family Planning Commission of the People’s Republic of China Criteria of weight for adults (WS/T 428–2013). Beijing: Standards Press of China; 2013. http://www.nhc.gov.cn/wjw/yingyang/201308/a233d450fdbc47c5ad4f08b7e394d1e8.shtml
Seagle HM, Wyatt HR, Hill JO. Chapter 24 - Obesity: overview of treatments and interventions. In: Coulston AM, Boushey CJ, Ferruzzi MG, eds. Nutrition in the Prevention and Treatment of Disease (Third Edition). Academic Press; 2013:445–64
Seagle HM, Wyatt H, Hill JO. Chapter 31 - Obesity: overview of treatments and interventions. In: Coulston AM, Rock CL, Monsen ER, eds. Nutrition in the Prevention and Treatment of Disease. Academic Press; 2001:465–80
Browning LM, Hsieh SD, Ashwell M. A systematic review of waist-to-height ratio as a screening tool for the prediction of cardiovascular disease and diabetes: 0.5 could be a suitable global boundary value. Nutr Res Rev. 2010;23:247–69. https://doi.org/10.1017/S0954422410000144
Li H, Jia J, Yang Z. Mini-mental state examination in elderly Chinese: a population-based normative study. J Alzheimer’s Dis JAD. 2016;53:487–96. https://doi.org/10.3233/jad-160119
Liu Z, Albanese E, Li S, Huang Y, Ferri CP, Yan F, et al. Chronic disease prevalence and care among the elderly in urban and rural Beijing, China - a 10/66 Dementia Research Group cross-sectional survey. BMC Public Health. 2009;9:394. https://doi.org/10.1186/1471-2458-9-394
Statistics, N.B.O. National data. Explanatory Notes on Main Statistical Indicators. In: China Statistical Yearbook. National Bureau of Statistics of China. 2024. https://www.stats.gov.cn/sj/ndsj/2024/indexeh.html. Accessed 13 Dec 2024
Morys F, Dadar M, Dagher A. Association between midlife obesity and its metabolic consequences, cerebrovascular disease, and cognitive decline. J Clin Endocrinol Metab. 2021;106:e4260–74. https://doi.org/10.1210/clinem/dgab135
Ho D, Imai K, King G, Stuart EA. MatchIt: nonparametric preprocessing for parametric causal inference. J Statis Software. 2011;42:1–28. https://doi.org/10.18637/jss.v042.i08
Singh-Manoux A, Dugravot A, Shipley M, Brunner EJ, Elbaz A, Sabia S, et al. Obesity trajectories and risk of dementia: 28 years of follow-up in the Whitehall II study. Alzheimers Dement. 2018;14:178–86. https://doi.org/10.1016/j.jalz.2017.06.2637
Khosravi A, Nielsen RO, Mansournia MA. Methods matter: population attributable fraction (PAF) in sport and exercise medicine. Br J Sports Med. 2020;54:1049–54. https://doi.org/10.1136/bjsports-2020-101977
von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. Lancet. 2007;370:1453–7. https://doi.org/10.1016/s0140-6736(07)61602-x
Ren R, Qi J, Lin S, Liu X, Yin P, Wang Z, et al. The China Alzheimer Report 2022. Gen Psychiatr. 2022;35:e100751. https://doi.org/10.1136/gpsych-2022-100751
Liu M, He P, Zhou C, Zhang Z, Zhang Y, Li H, et al. Association of waist-calf circumference ratio with incident cognitive impairment in older adults. Am J Clin Nutr. 2022;115:1005–12. https://doi.org/10.1093/ajcn/nqac011
Lei Q, Tian H, Xiao Z, Wu W, Liang X, Zhao Q, et al. Association between body mass index and incident dementia among community-dwelling older adults: the Shanghai aging study. J Alzheimers Dis. 2022;86:919–29. https://doi.org/10.3233/JAD-215517
Cui GH, Guo HD, Xu RF, Jiang GX, Chen SD, Cheng Q. The association of weight status with cognitive impairment in the elderly population of a Shanghai suburb. Asia Pac J Clin Nutr. 2013;22:74–82. https://doi.org/10.6133/apjcn.2013.22.1.18
Kivipelto M, Ngandu T, Fratiglioni L, Viitanen M, Kareholt I, Winblad B, et al. Obesity and vascular risk factors at midlife and the risk of dementia and Alzheimer disease. Arch Neurol. 2005;62:1556–60. https://doi.org/10.1001/archneur.62.10.1556
Ma Y, Ajnakina O, Steptoe A, Cadar D. Higher risk of dementia in English older individuals who are overweight or obese. Int J Epidemiol. 2020;49:1353–65. https://doi.org/10.1093/ije/dyaa099
Albanese E, Launer LJ, Egger M, Prince MJ, Giannakopoulos P, Wolters FJ, et al. Body mass index in midlife and dementia: systematic review and meta-regression analysis of 589,649 men and women followed in longitudinal studies. Alzheimers Dement. 2017;8:165–78. https://doi.org/10.1016/j.dadm.2017.05.007
Sun JY, Huang WJ, Hua Y, Qu Q, Cheng C, Liu HL, et al. Trends in general and abdominal obesity in US adults: evidence from the National Health and Nutrition Examination Survey (2001–2018). Front Public Health. 2022;10:925293. https://doi.org/10.3389/fpubh.2022.925293
Lear SA, Humphries KH, Kohli S, Birmingham CL. The use of BMI and waist circumference as surrogates of body fat differs by ethnicity. Obesity. 2007;15:2817–24. https://doi.org/10.1038/oby.2007.334
Abraham TM, Pedley A, Massaro JM, Hoffmann U, Fox CS. Association between visceral and subcutaneous adipose depots and incident cardiovascular disease risk factors. Circulation. 2015;132:1639–47. https://doi.org/10.1161/CIRCULATIONAHA.114.015000
Pan XF, Wang L, Pan A. Epidemiology and determinants of obesity in China. Lancet Diabetes Endocrinol. 2021;9:373–92. https://doi.org/10.1016/S2213-8587(21)00045-0
Mina T, Yew YW, Ng HK, Sadhu N, Wansaicheong G, Dalan R, et al. Adiposity impacts cognitive function in Asian populations: an epidemiological and Mendelian Randomization study. Lancet Reg Health-W. Apr 2023;33doi:ARTN 100710. https://doi.org/10.1016/j.lanwpc.2023.100710
Gordon-Larsen P, Wang H, Popkin BM. Overweight dynamics in Chinese children and adults. Obes Rev. 2014;15:37–48. https://doi.org/10.1111/obr.12121
Ren Z, Li Y, Li X, Shi H, Zhao H, He M, et al. Associations of body mass index, waist circumference and waist-to-height ratio with cognitive impairment among Chinese older adults: based on the CLHLS. J Affect Disord. 2021;295:463–70. https://doi.org/10.1016/j.jad.2021.08.093
Yang YC, Walsh CE, Johnson MP, Belsky DW, Reason M, Curran P, et al. Life-course trajectories of body mass index from adolescence to old age: Racial and educational disparities. Proc Natl Acad Sci USA. Apr 2021;118. https://doi.org/10.1073/pnas.2020167118
Clarke P, O’Malley PM, Johnston LD, Schulenberg JE. Social disparities in BMI trajectories across adulthood by gender, race/ethnicity and lifetime socio-economic position: 1986–2004. Int J Epidemiol. 2009;38:499–509. https://doi.org/10.1093/ije/dyn214
Shim YS, Park KH, Chen C, Dominguez JC, Kang K, Kim HJ, et al. Caregiving, care burden and awareness of caregivers and patients with dementia in Asian locations: a secondary analysis. BMC Geriatr. 2021;21:230. https://doi.org/10.1186/s12877-021-02178-x
Zhao W, Jones C, Wu MW, Moyle W. Healthcare professionals’ dementia knowledge and attitudes towards dementia care and family carers’ perceptions of dementia care in China: an integrative review. J Clin Nurs. 2022;31:1753–75. https://doi.org/10.1111/jocn.15451
Jia L, Quan M, Fu Y, Zhao T, Li Y, Wei C, et al. Dementia in China: epidemiology, clinical management, and research advances. Lancet Neurol. 2020;19:81–92. https://doi.org/10.1016/S1474-4422(19)30290-X
Acknowledgements
This study was supported by the National Science Foundation of China/the Economic and Social Research Council, UK Research and Innovation joint call: Understanding and Addressing Health and Social Challenges for Ageing in the UK and China. UK-China Health and Social Challenges Ageing Project (UKCHASCAP): present and future burden of dementia, and policy responses. (Grant number 72061137003, ES/T014377/1). The funders of the study had no role in study design, data collection, data analysis, data interpretation, or writing of the report, or in the decision to submit the paper for publication.
Author information
Authors and Affiliations
Contributions
MRZ contributed to the analysis and interpretation of the data and drafted the manuscript. YTC contributed to the analysis and interpretation of the data, and reviewed and edited the manuscript. SLR contributed to the discussion, and reviewed and edited the manuscript. YYL contributed to the data analysis. AS contributed to the review. EJB and JL contributed to the study concept and design, and reviewed and edited the manuscript. All authors approved the final version of the manuscript and agreed to be accountable for all aspects of the work, ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Zeng, M., Chen, Y., Lobanov-Rostovsky, S. et al. Adiposity and dementia among Chinese adults: longitudinal study in the China Health and Retirement Longitudinal Study (CHARLS). Int J Obes 49, 706–714 (2025). https://doi.org/10.1038/s41366-024-01698-x
Received:
Revised:
Accepted:
Published:
Version of record:
Issue date:
DOI: https://doi.org/10.1038/s41366-024-01698-x
This article is cited by
-
Lung function as a mediator: bridging appendicular skeletal muscle mass and dementia in middle-aged and older Chinese adults
European Journal of Medical Research (2026)
