
Abstract
Obesity is a prevalent global health challenge with a significant yet unclear impact on musculoskeletal health, particularly among females. This systematic review aimed to unravel the association between obesity and musculoskeletal health, as well as functional mobility in women. A comprehensive literature search was conducted across PubMed, Scopus, Web of Science, and the Cochrane Library for articles published between January 2001 and December 2023. Studies were selected based on their examination of the relationship between overweight or obesity and musculoskeletal health (including bones, joints, and soft tissues) and/or functional mobility in adult females (age ≥19) within the general population. Studies focusing on selective populations, or involving subjects with other health conditions or work-related musculoskeletal issues, were excluded. The data collected revealed a direct impact of obesity on musculoskeletal health, gait, and functional mobility, especially among women. Markedly, there was a strong association between obesity and musculoskeletal pain, particularly lower back pain. Obesity significantly alters gait biomechanics, leading to increased plantar pressure, altered kinematic patterns, and higher energy expenditure during walking. Higher BMI was found to significantly impact mobility-related limitations. Data also revealed that obesity, especially with BMI levels above 35 kg/m², adversely affects weight-bearing tasks such as walking, stair climbing, and chair rise ability. The findings of this systematic review emphasize the need for targeted interventions to address obesity-related mobility challenges, gait alterations and musculoskeletal pain to allow independence and enhanced functional outcomes in the daily activities of individuals with obesity. Exploring gender differences in obesity towards better understanding of the effect of obesity on the musculoskeletal health and functional mobility of women is critical for devising female-specific mitigation measures and optimizing management and treatment modalities, including pharmacotherapy.
Similar content being viewed by others

Introduction
Prevalence
With more than two billion people (30% of the world’s population) overweight or with obesity and an annual cost of $2.1 trillion, obesity poses severe global health and economic problems [1]. According to new research by the McKinsey Global Institute (MGI), a devastating $2.1 trillion, or 2.8 percent of global GDP is currently spent on obesity related health problems annually, but less than 1% on prevention [2]. Today, obesity comprises the 5th leading risk factor for mortality in the world (around 3.4 million annual deaths), as it significantly increases the risk for developing numerous chronic diseases including coronary heart disease (by over 50%), ischemic stroke (by 44%), type 2 diabetes (by 23%), as well as many cancers (up to 41%) [1,2,3]. The problem is expected to worsen, where almost half of the world’s adult population is expected to be overweight or with obesity by 2030 [2]. The global trend of sustained growth in obesity prevalence indicates that the current measures in the prevention, treatment, and management of the condition are largely ineffective. World Health Organization (WHO) 2016 data reveals that the UAE currently ranks fifth in the world in obesity, at a prevalence rate of 36% (33% males and 39% females) [1]. In other words, three in every ten Emirati males and almost four out of every ten females have obesity, with an economic burden amounting to $6 billion/year in associated disease cost [2]. If we also include the percentage of overweight individuals, based on the most recent Global Burden of Disease report [1], more than 60% of men and 66% of women in the UAE are currently overweight or with obesity (average of 63% or more than double the global average of 30%). Furthermore, while the UAE slightly fares better than the US in adult obesity prevalence (US current rate is 38%), UAE children are 1.8 times more likely to have obesity than American children, indicating a dangerous future trend and prognosis as well as ineffective prediction tools and preventive/intervention strategies, particularly considering the very young median age of the population (30.3 years) [3]. This instigates huge health and economic challenges since obesity is an independent risk factor for both T2D and CVD, the major culprits for mortality and morbidity in the UAE [3].
The biomechanics of obesity
The biomechanical impact of obesity on the musculoskeletal system comprises a complex mechanical and biochemical interplay, typically resulting in a cascading vicious cycle of events leading to musculoskeletal dysfunction. The additional loading placed on the weight bearing joints (hip, knee, ankle), due to extra body weight, accelerates the wear of cartilage and increases the risk of joint pathology, including osteoarthritis. Excessive loading also compromises the structural integrity of these joints, resulting in a reduction of joint space, as well as formation of osteophytes and subchondral bone sclerosis. From a biochemical perspective, obesity results in systemic metabolic dysfunction due to secreted adipokines, including leptin, resistin, and adiponectin, associated with chronic low-grade inflammation. This pro-inflammatory state further exacerbates joint degradation and reduces the ability to regenerate cartilage, hence accelerating the progression of osteoarthritic changes and altering the joint biomechanics. Obesity-related metabolic syndrome and insulin resistance are also associated with joint pathology by enhancing oxidative stress and impairing chondrocyte function, leading to further breakdown of cartilage [4].
Mechanically, obesity poses a significant burden on the musculoskeletal system [5]. Individuals with higher waist circumference and body mass demonstrate difficulty in walking, balance, and maintaining strength and mobility while performing basic daily living activities. Individuals with obesity are reported to have greater musculoskeletal loading and higher, abnormally distributed joint loads, particularly on the lower extremity joints (hip, knee, ankle) during weight bearing tasks, such as walking and stair climbing [6, 7]. In their study on lower extremity joint forces in healthy weight, overweight, and individuals with obesity, Stanford et al. found a significant increase in absolute peak hip, knee, and ankle joint forces by 40%, 43%, and 48%, respectively, for the high-BMI versus normal group. This study also confirmed that body mass accounted for 70–80% of the variation in the peak compressive loads at the hip, knee, and ankle during gait, where the joint loads increased approximately linearly with the body mass [8]. A subject- and kinematics-specific musculoskeletal modeling approach was used by [9] to compare spinal loads between people with normal weight and people with obesity performing static two-handed load-reaching activities. Each model incorporated personalized muscle architectures, body mass distributions, and full-body kinematics for each subject and task. The results indicated that individuals with obesity experienced significantly larger (by ∼38% in average) L5-S1 compression (2305 ± 468 N versus 1674 ± 337 N) and shear (508 ± 111 N versus 705 ± 150 N) loads during all reaching activities.
Obesity is also associated with structural changes in the musculoskeletal system, decreased range of motion and mobility, modification of the gait patterns and changes in the absolute and relative energy expenditures for a given activity [7]. There is growing evidence on the impact of obesity on skeletal muscle function, including impairment in oxidative capacity, abnormal muscle fiber organization, and interruption of the calcium cycle, inducing easy fatigue and an overall decline in contractile function [10]. Individuals with obesity are also reported to have reduced maximum muscle strength in the lower limb muscles (anti-gravity muscles) relative to their body mass as compared to individuals without obesity [11]. This results in the increased risk of developing osteoarthritis and various functional limitations, especially in the elderly, where high levels of adiposity and sarcopenia may impair agonist muscle activation. Obesity-related decline in function and physical performance are due, in part, to compromised muscle strength, power, and endurance with several underlying mechanisms implicated, including alterations in myofilament protein function and cellular contractile properties, as well as morphological adaptations, such as shifts in fiber type composition and increased intramyocellular lipid content within skeletal muscle. Obesity is also associated with reducing skeletal muscle contractility in older adults. This potentially results in reduced function partly due to altered cellular (single fiber) and molecular (myosin-actin interactions) properties [12].
Moreover, obesity significantly leads to alterations in spinal biomechanics and kinematics of the pelvis, impacting postural balance, as well as the functional performance in a wide range of activities of daily living (ADLs). Increased loads on the pelvis and spine often disturb normal posture and gait patterns [13], leading to increased lumbar lordosis and waddling gait, characterized by excessive lateral pelvic tilt and trunk sway [14]. The increased mechanical load, muscle imbalances, gait alterations, and inflammatory state associated with obesity contribute to degenerative changes in the spine and pelvis, potentially leading to diminished functional mobility and chronic low back pain (CLBP)). Obesity has been associated with changes in spinal posture, and spinal as well as hip motion/kinematics in adults. This includes increased thoracic kyphosis but decreased spinal and hip mobility, except for thoracic lateral flexion [15].
Relative to the extensive literature available on many aspects of obesity, there is a scarcity of information pertaining to the functional musculoskeletal and biomechanical limitations imposed by the condition [5, 7]. Quantifying how obesity affects the biomechanics of locomotion and gait, muscle structure and function, as well as postural changes, provides insight into the relationship between metabolic and mechanical energetics, mechanical loading and the risk of musculoskeletal injury and allows for data-driven, informed intervention [6].
Obesity, mobility, and quality of life
Functional mobility (FM) is defined as a person’s physiological ability to move independently and safely in diverse environments in order to accomplish functional tasks/activities and to effectively participate in the activities of daily living (ADL) at home, at work, and in the community [8]. One of the big challenges in obesity is the vicious circle created by the extra weight, where the increase of weight typically leads to less mobility, which yet results in more weight gained. Pataky et al. [9] argued that while significant advances in the understanding of the nature of obesity and its consequences on musculoskeletal health, gait and posture have been accomplished, the functional capacity of individuals with obesity as related daily physical activities remains elusive [9]. This was mainly attributed to the focus one element of functional capacity (such as gait, endurance, or balance), rather than its multifaceted nature. The International Classification of Functioning and Disability (ICF) developed by WHO provides a global framework to describe the impact of health conditions, such as obesity, on functional living. In a review article by Forhan et al. [8], the compromised mobility experienced by persons with obesity was associated with reduced health-related quality of life (HRQoL) as compared to normal weight individuals. The various measures of quality of life and functional mobility used in the different articles consistently demonstrated an association between obesity, impairments of body functions and structures and personal and environmental factors which contributed to mobility disability. Busutil et al. [16] studied the effect of obesity on the HRQoL in Spain using Spanish National Health Survey data. They found that a BMI ≥ 35 reduced HRQOL even in the absence of chronic diseases. Obesity increased the probability of HRQOL problems in mobility (11.8%), self-care (2.2%), usual activities (4.3%) and pain/discomfort (7.4%). Furthermore, this study suggested that HRQOL in women was significantly worse than average.
Obesity is also associated with a significant psychosocial burden, which ultimately impacts the quality of life. Many individuals with obesity, especially women, also struggle with issues related to mood, self-esteem, depression and anxiety, and body image. This emotional distress can impact successful treatment, including exercise and diet, significantly affecting mobility and health-related quality of life (HRQoL) [17, 18]. In their study on the psychological impact of obesity, Asharaf et al. [19] highlighted the intricate interactions among obesity, weight-related symptoms, HRQoL, and mental health, where they found significant correlations between obesity and fatigue, joint pain, and depression. These authors emphasized the need for tailored interventions, early prevention, and targeted management strategies for vulnerable subgroups to enhance the overall mobility, well-being and mental health of individuals with obesity. Another recent study by [20] shows that although their male participants had a higher degree of obesity, their self-esteem showed a higher level of confidence. Interestingly, in accordance with the degree of obesity, the males perceived their own body image, at a pre-obesity level, although in terms of the abdominal obesity degree, most males were below the threshold value of 90%.
Obesity has also been closely linked with multiple social and environmental determinants, including individual characteristics (e.g. sex, age, race, ethnicity, and socioeconomic status (SES)), environmental characteristics (e.g. living space and sociocultural norms), and social hierarchy (e.g. social status/rank) influences [21]. In particular, socioeconomic disparities in obesity persist worldwide, where higher rates of obesity, and resulting lower functional mobility, are associated with low socioeconomic status individuals, as high calorie, energy dense food options are or perceived as more affordable. Additionally, environments experiencing deprivation, disorder, or high crime have been shown to be associated with higher odds of obesity, which may appear more frequently in low social status individuals [22].
Considering the high prevalence of obesity and consistent early onset, its devastating musculoskeletal health impact, and the significant effects on FM and HRQOL in females, this review focused on the association of obesity with musculoskeletal health and functional mobility in females. The remainder of the article is organized as follows: Section “Materials and methods” discusses the review approach, while Sections “Musculoskeletal health”, “Gait and function”, and “Functional mobility” provide the review results pertaining to musculoskeletal health, gait and function, and functional mobility among females, respectively. The economical burden of obesity/overweight is discussed in Section “Economical burden”. Sections “Clinical implications and future research directions” and “Limitations” highlight the clinical implications and limitations of this study, respectively, and finally, Section “Conclusion and future work” offers the concluding remarks.
Materials and methods
Review design
This review was performed in accordance with Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) protocol [23]. Motivated by the continuous worldwide increase in the prevalence of obesity and its impact on musculoskeletal system in association with gait and daily activities, and how the health span of females, from puberty to childbearing and through menopause, puts them at a unique risk for obesity, we systematically reviewed articles addressing the effect of overweight and/or obesity on the musculoskeletal health and mobility of female adults, which included observational studies of longitudinal and cross-sectional type, population and cohort-based studies, as well as reviews.
Search strategy
A systematic search of published articles between January 2001 to December 2023 was conducted using the databases of PubMed, Scopus, Web of Science, and Cochrane Library. According to the syntax rules of each database, the following keywords were logically combined to identify relevant studies addressing the effects of overweight/obesity on musculoskeletal biomechanics: obes*, overweight, excess weight, BMI, body mass index, weight gain, increased weight, bone health, bone mineral density, soft tissue, biomechanic*, orthopedic*, orthopedic*, low back pain, musculoskeletal pain, bone*, feet, foot, hip, joint*, injur*, fracture*, trauma*, lesion*, mobility, motion, movement, and walking. Included studies were those focused on female adults representing a general population. The search was limited to articles published in English language only.
A sample search query applied in the PubMed database is given in Table 1. The search results were further analyzed using the VOSviewer, which constructs maps of the keywords (title and abstract) based on occurrence, as shown in Fig. 1 [24]. This depiction helps to understand the nature of the articles identified during the search process while using a combination of keywords as discussed above. The size of the label and area of the circle represent the total occurrences of the keywords (i.e. the relative relevance of that keyword/topic among the list of the search results).

Keyword map generated using the VOSviewer illustrating the relevance of different keywords in the PubMed search results.
Selection criteria
This systematic review included original, peer-reviewed scientific journals and conference articles which met the following criteria:
-
The studies examining the relationship of overweight or obesity with musculoskeletal health, including bone, joint, and soft-tissues;
-
Research focusing on the association between overweight or obesity and functional mobility;
-
The population consisting of only female adults aged 19 and older, representing a general population;
-
Obesity defined based on height and weight or waist circumference or hip circumference or weight to hip ratio;
-
Inclusion of subjects with no disabilities and no history of other health issues, including inflammatory diseases, systemic disorders, osteoarthritis, osteoporosis, chronic venous disease, diabetes, and soft tissue infection.
The studies with the following characteristics were considered outside the scope of this review:
-
Studies focusing on a selective population, including, working population, softball pitchers, nurses, veterans, pregnant, computer workers, nursing home residence, older home care patients, adult twins, and post/pre-menopausal women;
-
Studies specifically investigating participants with inflammatory diseases (e.g., cancer), systemic disorders (e.g., diabetes mellitus and rheumatoid arthritis), osteoarthritis, total knee joint arthroplasty, leukemia, chronic venous disease, Type 2 diabetes, and soft tissue infections;
-
Articles involving subjects with post knee/hip replacement, and/or surgery and joint arthroplasty, post/pre-bariatric surgery;
-
Studies addressing subjects with work-related musculoskeletal issues;
-
Studies addressing combined effects of obesity and other parameters, e.g., influence of obesity and muscle strength on mobility;
-
Letters to editor and editorials, opinion pieces, conference summary, comment, short survey, and note;
-
Non-English publication.
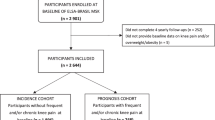
A PRISMA flow diagram illustrating the process of search and screening of articles is shown in Fig. 2.

Flowchart of the search and screening process based on PRISMA guidelines.
Data extraction
The title and abstract of each article were initially screened by one author (DMM) and verified by the other author (KK) against the predefined inclusion and exclusion criteria. The full text of the potentially eligible records was obtained and reviewed to determine final inclusion by DMM, followed by verification by KK. Extracted information included author name and year of publication, study design and setting, participant age, sample size, sample BMI, co-variables, adjustment parameters, assessment/measurement protocol, data analysis protocol, and key findings (Tables 2 and 3). Inconsistencies and disagreements were resolved through discussion, and if consensus could not be reached, a third author (FAA) was consulted. This process ensured inter-rater reliability and minimized bias in data collection. Additionally, the reference lists of the included articles were scanned to identify additional publications of interest.
The data were then analyzed using descriptive methods, including tabulation of the study characteristics and summarization of outcomes. Key characteristics and results were compared with similar studies to draw concluding remarks and identify future research direction.
Musculoskeletal health
Based on the search criteria, a total of 20 articles, including reviews which examined the musculoskeletal consequences of obesity, were identified (Table 2). Although several factors are known to contribute to musculoskeletal issues, this study will particularly focus on the association of obesity with musculoskeletal health in females.
This section is divided into three subsections highlighting pain and fracture, gait, and functional mobility.
Pain and fracture
The risk of developing lower back pain (LBP) with increasing BMI has been well documented in the literature for decades. However, the link between musculoskeletal pain and weight-related factors remains controversial. An earlier study, involving 709 Japanese middle-aged (40–69 years) women, found a higher prevalence of frequent shoulder pain at age 50, as well as an increased prevalence of frequent leg pain and difficulty of daily movements as a result of increased BMI [25]. On the other hand, data from U.A.E residents revealed only a moderate association of obesity with LBP [26]. This cross-sectional study analyzed interview questionnaire data of 374 females and 428 male residents of the U.A.E and identified that the prevalence of LBP in the population with obesity was higher among females (41.3%) than males (24.6%), further establishing the fact that obesity was moderately associated with LBP. In subsequent work, the authors reviewed 95 articles and the meta-analysis of 33 studies, and the results highlighted gender-specific observations on obesity and LBP. Based on the analysis of cross-sectional studies, both women with obesity and overweight exhibited an increased prevalence of back pain in the past 12 months. On the contrary, analyses from cohort studies revealed that obesity, but not overweight, was a risk factor for developing lower back pain in the past 12 months, among female subjects. Although men were at risk of developing lower back pain, the severity was less compared to women. A possible explanation for this gender-related difference could be the hormone-related obesity and associated changes in pain sensitivity, or difference in the proportion of mass distribution, or small sample size [27, 28].
A cross-sectional study which examined the young Finnish population of ages ranging from 24 to 39 for the association of various weight-related factors (BMI, waist circumference, hip circumference, waist-to-hip ratio), adipokins, and C-reactive protein with LBP further ascertained that obesity is associated with LBP in women, but not in men. Among the various weighted-related factors assessed, waist circumference was the highest risk factor for LBP in women. The effect of obesity and low back pain on the kinematics of trunk motion was also examined in [29]. This study was conducted on a small sample size of 37 women (13 subjects with obesity without LBP, 13 subjects with obesity with non-specific chronic LBP, and 11 normal subjects with no history of musculoskeletal issues), and the kinematics, including lateral bending (frontal plane) and forward flexion (sagittal plane) data were acquired. The subjects with obesity and chronic low back pain (cLBP) were characterized by a reduced range of motion of the spine as a result of impaired mobility, as well as increased lumbar lordosis as compared to individuals with obesity and no cLBP.
The thoracic range of motion was also found to be significantly lower in both the subjects with obesity without cLBP and the subjects with obesity with cLBP groups compared to the normal group, whereas the lumbar range of motion remained the same across the three sub-groups. Heuch et al. examined data from 2 surveys (HUNT 2 study and HUNT 3) conducted approximately 11 years apart in a Norwegian county further highlighted the risk of developing chronic LBP (cLBP) in relation to obesity [30]. This 11-year follow-up study, which examined data from 14,048 females, aged 30–69 years old found that crude risk, as well as crude recurrence of cLBP were higher among women than men in all age groups. The association between increasing BMI and recurrence of cLBP was noticeable among women after adjusting for age, while further adjustment for confounding factors weakened this association. Logistic regression analysis after adjusting for age also revealed a positive association of BMI with the risk of cLBP among women. Studies have further confirmed that obesity is a risk factor for musculoskeletal pain among women [31, 32]. In [31], data from 6079 middle-aged [33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52] Latin-American women revealed that women with low BMI (<18.5) showed non-significant lower risk, while women with overweight and obesity exhibited an increased risk of musculoskeletal pain. Rosa et. al reported similar findings in their cross-sectional study that examined a total of 466 middle-aged individuals (with 342 females) with severe obesity (BMI ≥ 35 kg/m2 with comorbidities or ≥ 40 kg/m2 without comorbidities). Prevalence of pain was reported by 95% of women (compared to 77.4% for men) with 57.8% reporting severe pain. A moderate positive correlation between BMI and pain at the shoulder (p = 0.010), knee (p = 0.042), and ankle (p = 0.024) joints was also recorded. This study further emphasizes that female gender and obesity were significant factors associated with the prevalence and intensity of MSK pain. A higher prevalence of moderate to severe LBP was also reported among community- dwelling older female Australians than males (18% vs. 11%) and being overweight or with obesity was a risk factor among females in developing LBP. Overweight female participants had 50% higher odds of reporting moderate to severe LBP as compared to healthy counterparts at baseline when adjusted for age and depression. Both males with obesity and females with obesity had more than twice the odds of reporting moderate to severe LBP compared to healthy subjects at baseline BMI. On the other hand, Handini et al. also found no correlation between increased BMI and LBP [53]. However, the study included only 12 female participants, and the findings may be influenced by the small sample size. Hussein et al. reported no association of pain intensity among patients with non-specific cLBP with the anthropometric measures of obesity, such as weight, BMI, waist circumference, hip circumference, waist-hip ratio [54]. The study included 132 participants in total, with 50 female participants. This study suggests that obesity may lead to the onset of LBP, however, the effect of obesity in worsening the pain intensity may be limited. It is worth noting that the conflicting findings in these studies may be attributed to the study design, including the population size, characteristics of the participants, and the confounding factors. For instance, Handini et al.’s study included only 12 female participants, which limits the generalizability of the results. In contrast, Hussein et al. considered a larger sample of 132 participants (50 females), providing more robust evidence. However, neither study explicitly reported the confounding factors considered, thus making it difficult to generalize the findings.
Another study has also highlighted the association of increased musculoskeletal pain among women with BMI 27–34, and an increased all-course and cardiovascular mortality among those with a BMI higher than 40 kg/m2 [55]. In [56] and [57], obesity and overweight were found to be associated with lower back pain. Another recent study has reported higher prevalence of low-muscle mass among younger females (aged 18–32 years) in comparison to older adults, aged 45–88 years old. Besides, higher prevalence of obesity, as well as low bone density was observed among older females compared to the younger population [58]. Additionally, the association of obesity with MSK was explored in the review articles by Wearing et al. and Anandacoomarasamy et al. [33, 59].
Besides musculoskeletal pain, the complex relationship between obesity and fracture was also explored by several researchers [34,35,36,37]. In a meta-analysis of a prospective cohort study, Tang et al. concluded that obesity in adults is significantly associated with a decreased risk of developing a hip fracture. Shen et al. also reported the association of increased BMI with a lower risk of major osteoporotic fractures and hip fractures in women [35]. This protective association of BMI with major osteoporotic fractures was largely explained by higher bone mineral density (BMD), but mostly in association with hip fractures. It was suggested that factors not associated with BMD, such as cushioning soft tissue thickness at the hip, may have contributed to the lower risk of hip fractures among women. A cohort study by Sogaard et al. suggested that women with higher BMI ( ≥ 25 kg/m2) had a decreased risk of hip fracture as compared with those with BMI < 22 and 22–24.9 kg/m2. The inverse association between BMI and hip fracture was linear in women in the age group of 70–79. However, for the age group of 50–59 and 60–69, the hip fracture risk was highest for those with BMI < 22 kg/m2, and the nonlinear association leveled off at BMIs 25 kg/m2 and above [36]. Kim et al. suggest that the association of BMI and hip fracture may depend upon ethnicity, as they observed that obesity was associated with an increased risk of hip fracture in women in particular, while overweight was associated with a lowest risk [37].
Gait and function
Walking, or gait is a fundamental movement pattern, which results from an extremely complex interplay between the musculoskeletal system and central nervous system. It has been well-documented that obesity poses significant challenges to the normal walking of subjects with overweight or obesity as they need to carry the excess body weight or body fat over the long term. Changes in the biomechanics of walking can be observed as alterations in foot plantar pressure, kinematics, kinetics, as well as spatiotemporal parameters. This review included 9 articles that focus on the association of obesity with gait (see Table 4).
In a gait study on Czech females [38], the authors investigated the effects of BMI on the absolute and relative plantar pressure parameters during walking in women with different BMI levels. It involved 163 Czech women with age ranging from 45 to 65 years (mean ± SD of age, 57.4 ± 5.3 years and BMI, 27.0 ± 5.3 kg/m2) representing three BMI groups (normal weight: <24.9, overweight: <29.9, and obesity: <34.9).
The BMI was objectively measured using a digital medical scale with a stadiometer (InBody BSM370; BioSpace, Seoul, South Korea) and gait analysis was performed by means of a Footscan pressure measurement system (RSscan International, Olen, Belgium). The analyzed pressure data included absolute peak pressure, contact percentage, absolute pressure impulse, and relative pressure impulse derived from ten-foot regions (first toe, second through fifth toes, first metatarsal, second metatarsal, third metatarsal, fourth metatarsal, fifth metatarsal, midfoot, medial heel, and lateral heel). A statistically significant between-group difference in the mean peak pressure values and absolute pressure impulse was observed in all foot regions except for second through fifth toes (p > 0.05). Similarly, the contact pressure demonstrated a significant between-group difference for the metatarsal regions and midfoot. In addition, relative pressure impulse reported a significant between-group difference for all foot regions except for the second through fifth toes and the first metatarsal. It can be concluded that increased body mass contributed to a higher peak pressure and total load on the foot during overground walking in women. In addition, pressure increase in the lateral forefoot and midfoot was also noticed. On the other hand, Jung et al. examined the effects of BMI on the plantar pressure while crossing an obstacle [39]. Twenty-seven middle-aged females who participated in a study were grouped into four according to their BMI, such as normal (age 52.80 ± 2.58 years and BMI 21.90 ± 0.68 kg/m2), overweight (age 48.37 ± 6.30 years and BMI 24.51 ± 0.95 kg/m2), slight obesity (age 50.85 ± 6.01 years and BMI 27.61 ± 1.8 kg/m2), moderate obesity (age 48.28 ± 5.05 years and BMI 39.13 ± 13.93 kg/m2). The results showed that during walking over obstacles of 10 cm height or above, an increase in BMI caused a significant increase in the plantar pressure in specific foot regions. Further, walking over obstacles of 20 cm, an increased plantar pressure was observed in all groups, including the normal-weight group.
Gill et al. assessed how different levels of obesity (Class I obesity: ≥30 to <35 kg/m2, Class II obesity: ≥ 35 to <40 kg/m2, and Class III obesity: >40 kg/m2) affect flat ground walking and obstacle crossing in adults through experiments involving 13 normal weight, 18 overweight/Class I, 16 Class II, and 20 Class III female adults with obesity [40]. They reported that the normal BMI group had faster gait velocity, lower variability in the velocity, shorter percentage of the gait cycle spent in stance and longer percentage in swing, as compared to those in the higher BMI classes. Class I showed faster velocity and less variability in velocity than Class II and Class III individuals. Notably, no differences were observed in the velocities between Class II and Class III. These findings suggest that increases in the classes of obesity contribute to remarkable changes in the walking patterns and lead to limited participation in challenging activities.
Obesity has also been associated with a different standing posture and altered trunk movement [41]. The standing posture in females with obesity was characterized by limitations in forward flexion and a larger pelvic tilt in the initial position, similar to a pattern that is often observed in women at later stages of pregnancy. The forward translation of the center of mass may have been compensated by adopting a higher pelvic tilt, which eventually led to non-specific or even specific low back pain [41]. In addition, changes in the thoracic movement during forward flexion and lateral bending were also reported. In support of these claims, Gilleard and Smith found that increased BMI was associated with restricted trunk forward motion both in sitting and standing posture [42]. A possible explanation could be the adjacent positioning of the anterior thigh and the abdominal tissue resulting in limited forward flexion motion while seated, and the decreased stability causing difficulties while standing. No significant differences in pelvic segment displacement and hip joint range of motion between the groups were observed during seated and standing flexion. Although not significant, the mediolateral width of the base of support increased with the increase in BMI. Further movement restrictions were observed in thoracic segment and thoracolumbar spine range of motion. Moreover, subjects with obesity exhibited an altered posture accompanied by an increase in the hip joint moment during standing work tasks. Several of the postural adaptations perceived in the obesity group were comparable with those seen during the progression of pregnancy.
Another important quantitative indicator of efficient walking is the energy expenditure. In general, the gross energy cost per distance forms a U-shaped curve when plotted against walking speed, and individuals typically prefer to walk at a speed that minimizes the energy required to walk a given distance. It has been observed that the metabolic rate for walking at a given speed is 0 to 33% higher in individuals with obesity as compared to their normal counterparts [43, 44]. Based on experimental trials involving 20 adult women (10 subjects with obesity and 10 normal-weight), Browning and Kram confirmed that women with obesity presented 11% higher metabolic cost when averaged across different walking speeds, greater relative aerobic effort while walking at preferred speed as compared to normal subjects [43]. In a subsequent study, these authors assessed the metabolic rates, energy cost per distance of walking vs. speed relationships, as well as the preferred walking speed of both women and men with obesity in relation to normal-weights. In addition, the effect of the adipose tissue distribution on the metabolic walking cost was also examined. They suggested both gender- and obesity-driven differences in the net metabolic rate, where women with obesity showed 10% higher net metabolic rate as compared to men with obesity and normal-weight women, and 20% higher rate as compared to normal-weight men [44]. The preferred walking speed was similar across the groups and was close to the speed that minimizes the energy cost per distance. However, they were unable to report conclusive results on the effects of the thigh or body mass distribution on the net metabolic rate. Another study [45] found that women with obesity walk with a greater relative effort, which can mostly be attributed to obesity-related increases in joint torques. In [46], the authors assessed changes in gait after a 30-min walking session. Ten women with obesity and ten normal-weight women participated in this study. They found a weak association between the hip/knee moments with BMI.
In summary, gait abnormalities in individuals with obesity are often reflected in reduced walking speed, step length, cadence, and swing time, increased stance phase and double-limb support time, a greater magnitude and rate of rearfoot eversion, reduced hip, knee, and ankle range of motion, and higher plantar pressure, ground reaction forces, and loads at knee [38,39,40].
Functional mobility
Increasingly used as an outcome in MSK rehabilitation assessment and numerous clinical studies, functional mobility remains poorly defined and non-standardized. The current definition is subjective and falls under the general umbrella of a person’s physiological ability to move independently and safely in a variety of environments to accomplish functional activities for daily living. Various qualitative and quantitative tools have been proposed over the years, including the International Classification of Functioning and Disability (ICF) from WHO, the Functional Mobility Scale (FMS), the Gillette, and the Functional Assessment Questionnaire Scale. Higher BMI has been reported to have a significant association with functional mobility-related limitations in both men and women. An older study [47] examined the association of different body composition indices, including muscle mass, percentage of body fat, and BMI, with functional limitations in a representative U.S. sample. This cross-sectional study involved 1391 men and 1526 women, aged 70 years or above, with a mean BMI of 26.4 and 26.4 kg/m2, respectively. They were grouped into five BMI classes, such as underweight (BMI < 18.5), normal-weight (BMI 18.5–24.99), overweight (BMI 25–29.99), class I obesity (BMI 30–34.99), and class II obesity (BMI ≥ 35). A questionnaire consisting of five mobility-related items (difficulty walking a quarter mile; difficulty walking up 10 steps without resting; difficulty carrying something as heavy as 10 pounds; difficulty stooping, crouching or kneeling; and difficulty standing up from an armless chair) were used to assess functional limitations. Statistical analyses revealed that women in the underweight, overweight, and obesity groups were significantly more likely to experience mobility limitations than those in the normal-weight group. Besides, no association between muscle mass and functional limitations were reported.
Researchers have also focused on the association of past or present obesity, as well as long-term weight loss, with functional limitations. Stenholm et al. explored the influence of early or late onset of obesity and obesity duration on walking limitations among middle-aged and older populations [48]. In a retrospective longitudinal study based on a representative sample of a Finnish population aged 50–99 years, statistical analysis revealed that subjects with obesity since the age of 30 (age and gender adjusted odds ratio (OR) 8.97, 95% confidence interval (CI), 3.06–26.29), 40 (OR 6.01, 95% CI, 2.55–14.14), and 50 (OR 4.33, 95% CI, 2.59–7.23) years had a higher risk of walking limitations as compared to individuals without obesity. Also, subjects with obesity ever since the ages of 30 and 40 years old had the highest prevalence of walking limitations (57% and 49%). This study found no association between neither age and obesity duration, nor between gender and obesity duration. Another similar study [49] assessed the association of overweight/obesity in young, middle, and late adulthood, and its cumulative effect over the adult life course, in which, participants aged 70–79 years at baseline were assessed over 7 years of follow-up recording their functional mobility (difficulty walking 1/4 mile or climbing 10 steps) semi-annually. BMI was calculated using recalled height at ages 25 and 50 years, and measured height at ages 70–79 years. This study further underlined the fact that overweight/obesity at young, middle, and late adulthood were associated with increased risk of incident mobility limitations in both men (1.6 fold higher) and women (2.8 fold higher) in late adulthood as compared to normal weight. Importantly, walking disability was more common in women with obesity than men with obesity. In [50], the authors explored how BMI and body composition (both total and segmental) affect functional capacity according to gender and obesity grade, by measuring the distance traveled during a 6 min Walk Test (6MWT). Six min Walk Distance (6MWD) was positively correlated with fat free mass (FFM), fat free mass of upper limb, and fat free mass of lower limb, and negatively with BMI, fat mass, fat mass of upper limb, and fat mass of lower limb among female participants. Several studies also investigated the association of functional mobility with different obesity measures. For example, Santarem et al. highlighted that total and segmental fat free mass or FFM associated better with walking performance than BMI. De Souza et al. reported higher prevalence rate of mobility (21.7% to 66.0%) and activities of daily living (ADL) (20.4% to 43.9%) disability among women than men [51]. On the other hand, gender-combined analyses revealed that higher values of waist circumferences are significantly associated with mobility disability, even for a short duration (4 years). Association of higher BMI levels with increased mobility limitations were also underscored by [52], where data from 2865 Black, 1846 Hispanic, and 9721 White middle-aged and older women were analyzed to draw conclusions. Refer to Table 5 for the details of the review outcomes.
In conclusion, although the exact definition of functional mobility varied among studies, the majority have consistently reported that a higher BMI, particularly above 35 kg/m2, adversely affects weight bearing tasks, including walking, stair climbing, and chair rise ability. Compared to men with obesity, women were found to have an increased risk of developing functional mobility limitations. This trend has been witnessed in both middle-aged and older population. Moreover, as most of the studies suggest, BMI and waist circumference could better predict the onset of mobility impairments [60].
Economical burden
In the last few decades, obesity has become a growing concern worldwide, reaching pandemic proportions [61]. Whilst overweight and obesity were generally considered the problems of high-income countries, recent trends reveal that low and middle-income countries are also witnessing an upsurge. Economic growth, urbanization and global free trade are some of the factors resulting in a global upsurge in the prevalence of obesity. It has also been reported that the prevalence of obesity tends to be higher among the wealthy in low-income countries and the economically disadvantaged in high-income countries [62]. These differences can be explained by various reasons, including increased food affordability with rising income, dietary shifts towards more Westernized eating patterns, and the adoption of sedentary lifestyles and occupations among wealthier individuals. However, in societies with higher income levels, there is a prevailing social stigma surrounding obesity, in addition to access to healthy diets, healthcare, education, and weight loss-promoting activities, which further amplifies the disparities in obesity rates [63].
Within the UAE, the current economic boom is steered by swift urbanization and increased inundation of expatriate workforce. This shift in economic climate is witnessed by rapid changes in lifestyle leading to a more modern, fast-paced and technology driven way of life. Combination of these factors has led to a reduction in domestic as well as occupational or leisure-driven physical activity in addition to the consumption of unhealthier, calorie-dense, prepackaged food choices. The aforementioned factors explain a sudden surge in obesity and related disorders in the country. In fact, the prevalence of obesity and overweight has doubled in the UAE between 1989 and 2017 [64]. As per the Central Intelligence Agency World Factbook, the prevalence rate of obesity in the UAE is 31.7% and the countries in the GCC region are ranked among the top 40 in the world for high prevalence of obesity and cardiometabolic disorders [65].
The high prevalence rate of obesity has a significant direct economic impact for individuals as well as the entire nation. This is evidenced by the direct healthcare care costs associated with the treatment of obesity and its related disorders. There is a significant correlation between individuals living with obesity and the use of at-home health care services, increased number of hospital visits, a surge in prescribed medications and a higher hospital admission rate with surgical and non-surgical treatments than individuals with optimum BMI. They also incur a higher cost of care and longer hospital stays [66]. There are also indirect costs that increase the economic burden resulting from lost or reduced productivity and human capital, especially arising from complications of obesity such as musculoskeletal disorders. Studies worldwide have shown that individuals with obesity have a higher rate of absenteeism from work than individuals without obesity, and work at less than full capacity when present at work [67].
Clinical implications and future research directions
The findings from this literature review address several gaps in our current understanding of the impact of obesity on musculoskeletal health and mobility in women, offering valuable clinical insights. Healthcare professionals may need to recognize that obesity has dual health implications, affecting both metabolic and musculoskeletal systems. The scientific evidence demonstrates that women with BMI values above 35 kg/m² experience elevated musculoskeletal pain mainly in their lower back thus requiring regular pain evaluations and prompt intervention strategies. Treatment plans should include hormonal factors and body composition analysis because the literature shows gender-specific musculoskeletal effects of obesity. The documented changes in gait patterns and mobility impairments require healthcare professionals to implement functional mobility assessments together with personalized physical therapy in their clinical practice. Weight reduction combined with muscle strengthening and biomechanical correction interventions will help reduce pain while enhancing both gait efficiency and overall mobility. The protective effects of obesity on certain fractures need to be evaluated against its negative effects on physical function. Medical professionals should implement a combined approach of weight management and physical rehabilitation with psychosocial support to improve musculoskeletal health and maintain independence in women who have obesity.
Future studies should focus on investigating the short- and the long-term effects of structured weight-loss interventions, exercise, and physiotherapy on mobility and pain management in women with obesity. Exploring the efficacy of these interventions in women with varying degrees of obesity will provide key insights into the management of their mobility and pain over time. Longitudinal studies will also help understand the long-term effects of obesity on musculoskeletal health in women. Based on the results of this review, future studies should track changes in gait, musculoskeletal health, and functional mobility over a period of time, in order to more comprehensively assess the effect of obesity on musculoskeletal health.
Limitations
Identifying suitable studies has proven challenging due to several limitations, including a scarcity of studies that independently compare the effects of obesity on male and female populations separately and limited research has specifically focused on female participants in the examination of the impact of obesity on musculoskeletal health, gait, and functional mobility.
Conclusion and future work
In conclusion, the comprehensive analysis of the literature reveals a clear and multifaceted impact of obesity on musculoskeletal health, gait, and functional mobility, particularly among women. The association between obesity and musculoskeletal pain, particularly lower back pain, is well-documented, with numerous studies highlighting increased prevalence and severity of pain in women with obesity. Gender-specific differences further suggest that hormonal factors and body mass distribution may play critical roles in these associations. While obesity is linked to an increased risk of musculoskeletal pain and reduced functional mobility, it appears to have a protective effect against certain types of fractures, likely due to higher bone mineral density and cushioning from soft tissues. The variability in findings across different studies indicates the need for more targeted research to fully understand the complex interplay between obesity and musculoskeletal health in women. Addressing obesity through effective interventions could potentially mitigate its adverse effects on musculoskeletal health, improving the quality of life for many women.
The reviewed literature also highlights the substantial impact of obesity on gait and functional mobility in females. Obesity significantly alters walking biomechanics, leading to increased plantar pressure, altered kinematic patterns, and higher energy expenditure during walking. These changes result in slower walking speeds, reduced range of motion, and greater physical effort required for movement. The studies consistently demonstrate that higher BMI levels are associated with greater deviations from normal gait patterns, contributing to increased risk of musculoskeletal issues and decreased functional mobility. Addressing obesity through targeted interventions is crucial for improving gait efficiency and reducing the risk of mobility-related health problems in females with obesity.
Additionally, the review of literature on functional mobility underscores the significant impact of higher BMI on mobility-related limitations, particularly in women. Despite variations in the definition of functional mobility, studies consistently show that obesity, especially with BMI levels above 35 kg/m2, adversely affects weight-bearing tasks such as walking, stair climbing, and chair rise ability. Women are more susceptible to mobility limitations compared to men, with walking disability being notably prevalent. The findings emphasize that both BMI and waist circumference are reliable predictors of mobility impairments, highlighting the need for targeted interventions to address obesity-related mobility challenges, thereby improving the overall quality of life and independence in daily activities for individuals with obesity.
References
WHO. Facts report. Geneva, Switzerland: World Health Organization; 2017.
Anandacoomarasamy A, Fransen M, March L. Obesity and the musculoskeletal system. Curr Opin Rheumatol. 2009;21:71–7.
Hills A, Hennig E, McDonald M, Bar-Or O. Plantar pressure differences between obese and non-obese adults: a biomechanical analysis. Int J Obes. 2001;25:1674–9.
Bollinger LM. Potential contributions of skeletal muscle contractile dysfunction to altered biomechanics in obesity. Gait Posture. 2017;56:100–7.
Frey C, Zamora J. The effects of obesity on orthopaedic foot and ankle pathology. Foot Ankle Int. 2007;28:996–9.
Catan L, Amaricai E, Onofrei RR, Popoiu CM, Iacob ER, Stanciulescu CM, et al. The impact of overweight and obesity on plantar pressure in children and adolescents: a systematic review. Int J Environ Res Public Health. 2020;17:6600.
Stanley TL, Chen ML, Goodman E. The typology of metabolic syndrome in the transition to adulthood. J Clin Endocrinol Metab. 2014;99:1044–52.
Forhan M, Gill SV. Obesity, functional mobility and quality of life. Best Pract Res Clin Endocrinol Metab. 2013;27:129–37.
Pataky Z, Armand S, Müller-Pinget S, Golay A, Allet L. Effects of obesity on functional capacity. Obesity. 2014;22:56–62.
Alaniz-Arcos JL, Ortiz-Cornejo ME, Larios-Tinoco JO, Klünder-Klünder M, Vidal-Mitzi K, Gutiérrez-Camacho C. Differences in the absolute muscle strength and power of children and adolescents with overweight or obesity: a systematic review. BMC Pediatr. 2023;23:474.
Tomlinson D, Erskine R, Morse C, Winwood K, Onambélé-Pearson G. The impact of obesity on skeletal muscle strength and structure through adolescence to old age. Biogerontology. 2016;17:467–83.
Straight CR, Toth MJ, Miller MS. Current perspectives on obesity and skeletal muscle contractile function in older adults. J Appl Physiol. 2021;130:10–6.
Khalaf K, Mohan DM, Al Hindi M, Khandoker AH, Jelinek HF. Plantar pressure alterations associated with increased BMI in young adults. Gait Posture. 2022;98:255–60.
Arora P, Dey S. The impact of obesity on spinal biomechanics and pelvic kinematics: a pathway to chronic low Back pain. Medknow. Indian J Pain 2024;38:S1–S3 https://doi.org/10.4103/ijpn.ijpn_89_24
Bayartai M-E, Luomajoki H, Tringali G, De Micheli R, Abbruzzese L, Sartorio A. Differences in spinal posture and mobility between adults with obesity and normal weight individuals. Sci Rep. 2023;13:13409.
Busutil R, Espallardo O, Torres A, Martínez-Galdeano L, Zozaya N, Hidalgo-Vega Á. The impact of obesity on health-related quality of life in Spain. Health Qual Life Outcomes. 2017;15:1–11.
Moradi M, Mozaffari H, Askari M, Azadbakht L. Association between overweight/obesity with depression, anxiety, low self-esteem, and body dissatisfaction in children and adolescents: a systematic review and meta-analysis of observational studies. Crit Rev Food Sci Nutr. 2021;62:555–70.
Sarwer DB, Polonsky HM. The psychosocial burden of obesity. Endocrinol Metab Clin. 2016;45:677–88.
Asharaf H, Thimothy G, George S, Jose J, Paily R, Josey J, et al. Psychological impact of obesity: a comprehensive analysis of health-related quality of life and weight-related symptoms. Obes Med. 2024;45:100530.
Rusu L, Piele D, Ilie E, Ionescu G, Marin MI, Rusu MR, et al. The relationship between body composition, physical activity, self-esteem, and body image in female and male adolescents. Sports. 2025;13:11.
Jalilzadeh M, Goharinezhad S. Exploring the multifaceted factors influencing overweight and obesity: a scoping review. Front Public Health. 2025;13:1540756.
Bittner JM, Gilman SE, Chen Z, Perkins NJ, Cheon BK. Socioeconomic mobility, metabolic health, and diet: mediation via subjective socioeconomic status. Obesity. 2024;32:2035–44.
Page MJ, Moher D, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. PRISMA 2020 explanation and elaboration: updated guidance and exemplars for reporting systematic reviews. BMJ. 2021;372:n160.
Van Eck N, Waltman L. Software survey: VOSviewer, a computer program for bibliometric mapping. Scientometrics. 2010;84:523–38.
Tsuritani I, Honda R, Noborisaka Y, Ishida M, Ishizaki M, Yamada Y. Impact of obesity on musculoskeletal pain and difficulty of daily movements in Japanese middle-aged women. Maturitas. 2002;42:23–30.
Bener A, Alwash R, Gaber T, Lovasz G. Obesity and low back pain. Coll Antropol. 2003;27:95–104.
Craft RM, Mogil JS, Aloisi AM. Sex differences in pain and analgesia: the role of gonadal hormones. Eur J Pain. 2004;8:397–411.
Snijder M, Van Dam R, Visser M, Seidell J. What aspects of body fat are particularly hazardous and how do we measure them?. Int J Epidemiol. 2006;35:83–92.
Vismara L, Menegoni F, Zaina F, Galli M, Negrini S, Capodaglio P. Effect of obesity and low back pain on spinal mobility: a cross sectional study in women. J Neuroeng Rehabil. 2010;7:1–8.
Heuch I, Heuch I, Hagen K, Zwart J-A. Body mass index as a risk factor for developing chronic low back pain: a follow-up in the Nord-Trøndelag Health Study. Spine. 2013;38:133–9.
Blümel JE, Arteaga E, Mezones-Holguín E, Zúñiga MC, Witis S, Vallejo MS, et al. Obesity is associated with a higher prevalence of musculoskeletal pain in middle-aged women. Gynecol Endocrinol. 2017;33:378–82.
Rosa S, Martins D, Martins M, Guimarães B, Cabral L, Horta L. Body Mass Index and Musculoskeletal Pain: A Cross-Sectional Study. Cureus. 2021;13:e13400. https://doi.org/10.7759/cureus.13400.
Anandacoomarasamy A, Caterson I, Sambrook P, Fransen M, March L. The impact of obesity on the musculoskeletal system. Int J Obes. 2008;32:211–22.
Tang X, Liu G, Kang J, Hou Y, Jiang F, Yuan W, et al. Obesity and risk of hip fracture in adults: a meta-analysis of prospective cohort studies. PLoS ONE. 2013;8:e55077.
Shen J, Leslie WD, Nielson CM, Majumdar SR, Morin SN, Orwoll ES. Associations of body mass index with incident fractures and hip structural parameters in a large Canadian cohort. J Clin Endocrinol Metab. 2016;101:476–84.
Søgaard AJ, Holvik K, Omsland TK, Tell GS, Dahl C, Schei B, et al. Age and sex differences in body mass index as a predictor of hip fracture: a NOREPOS study. Am J Epidemiol. 2016;184:510–9.
Kim SH, Yi SW, Yi JJ, Kim YM, Won YJ. Association between body mass index and the risk of hip fracture by sex and age: a prospective cohort study. J Bone Miner Res. 2018;33:1603–11.
Tománková K, Přidalová M, Svoboda Z, Cuberek R. Evaluation of plantar pressure distribution in relationship to body mass index in Czech women during walking. J Am Podiatr Med Assoc. 2017;107:208–14.
Jung J-M, Lee S-Y, Hwangbo G, Han J-T, Kim C-Y, Lee E-H. Plantar foot pressure distribution of middle-aged obese women while walking over obstacles of different heights. J Phys Ther Sci. 2011;23:725–8.
Gill SV. Effects of obesity class on flat ground walking and obstacle negotiation. J Musculoskelet Neuronal Interact. 2019;19:448.
Menegoni F, Vismara L, Capodaglio P, Crivellini M, Galli M. Kinematics of trunk movements: protocol design and application in obese females. J Appl Biomater Biomech. 2008;6:178–85.
Gilleard W, Smith T. Effect of obesity on posture and hip joint moments during a standing task, and trunk forward flexion motion. Int J Obes. 2007;31:267–71.
Browning RC, Kram R. Energetic cost and preferred speed of walking in obese vs. normal weight women. Obes Res. 2005;13:891–9.
Browning RC, Baker EA, Herron JA, Kram R. Effects of obesity and sex on the energetic cost and preferred speed of walking. J Appl Physiol. 2006;100:390–8.
Koushyar H, Anderson DE, Nussbaum MA, Madigan ML. Relative effort while walking is higher among women who are obese, and older women. Med Sci Sports Exerc. 2020;52:105–11.
Singh B, Vo H, Francis SL, Janz KF, Yack HJ. Changes in gait over a 30-min walking session in obese females. Med Sci Sports Exerc. 2017;49:555–62.
Davison KK, Ford ES, Cogswell ME, Dietz WH. Percentage of body fat and body mass index are associated with mobility limitations in people aged 70 and older from NHANES III. J Am Geriatr Soc. 2002;50:1802–9.
Stenholm S, Rantanen T, Alanen E, Reunanen A, Sainio P, Koskinen S. Obesity history as a predictor of walking limitation at old age. Obesity. 2007;15:929–38.
Houston DK, Ding J, Nicklas BJ, Harris TB, Lee JS, Nevitt MC, et al. Overweight and obesity over the adult life course and incident mobility limitation in older adults: the health, aging and body composition study. Am J Epidemiol. 2009;169:927–36.
Correia de Faria Santarém G, De Cleva R, Santo MA, Bernhard AB, Gadducci AV, Greve JMDA, et al. Correlation between body composition and walking capacity in severe obesity. PLoS ONE. 2015;10:e0130268.
de Souza Barbosa JF, dos Santos Gomes C, Costa JV, Ahmed T, Zunzunegui M, Curcio C-L, et al. Abdominal obesity and mobility disability in older adults: a 4-year follow-up of the international mobility in aging study. J Nutr Health Aging. 2018;22:1228–37.
Sharma A. Body mass index and mobility limitations: an analysis of middle-aged and older Black, Hispanic, and White women in the US. Obes Res Clin Pract. 2018;12:547–54.
Handini L. Correlation analysis between women’s body mass index and mechanical low back pain. Indian J. Forensic Med. Toxico. 2020;14:1959−63.
Hussien H, Kamel E, Kamel R. Association between pain intensity and obesity in patients with chronic non-specific low back pain. Biosci Res. 2019;16:3579–83.
Radojčić MR, Perera RS, Chen L, Spector TD, Hart DJ, Ferreira ML, et al. Specific body mass index trajectories were related to musculoskeletal pain and mortality: 19-year follow-up cohort. J Clin Epidemiol. 2022;141:54–63.
Sengar M, Gupta A, Kunwar R. Correspondence analysis to demonstrate the relationship between musculoskeletal pain and body mass index. Cureus. 2023;15. https://doi.org/10.7759/cureus.40570.
Lucha-López MO, Hidalgo-García C, Monti-Ballano S, Márquez-Gonzalvo S, Ferrández-Laliena L, Müller-Thyssen-Uriarte J, et al. Body mass index and its influence on chronic low back pain in the Spanish population: a secondary analysis from the European Health Survey (2020). Biomedicines. 2023;11:2175.
Abidin NZ. Obesity and musculoskeletal health of young and older malaysian women: a cross-sectional study. Malays J Med Sci. 2023;30:137.
Wearing SC, Hennig EM, Byrne NM, Steele JR, Hills AP. Musculoskeletal disorders associated with obesity: a biomechanical perspective. Obes Rev. 2006;7:239–50.
Vincent HK, Vincent KR, Lamb KM. Obesity and mobility disability in the older adult. Obes Rev. 2010;11:568–79.
Koliaki C, Dalamaga M, Liatis S. Update on the obesity epidemic: after the sudden rise, is the upward trajectory beginning to flatten?. Curr Obes Rep. 2023;12:514–27.
Collaborators GO. Health effects of overweight and obesity in 195 countries over 25 years. N Engl J Med. 2017;377:13–27.
Boutari C, Mantzoros CS. A 2022 update on the epidemiology of obesity and a call to action: as its twin COVID-19 pandemic appears to be receding, the obesity and dysmetabolism pandemic continues to rage on. Metabolism. 2022;133:155217. https://doi.org/10.1016/j.metabol.2022.155217.
Radwan H, Ballout RA, Hasan H, Lessan N, Karavetian M, Rizk R. The epidemiology and economic burden of obesity and related cardiometabolic disorders in the United Arab Emirates: a systematic review and qualitative synthesis. J Obes. 2018;2018:2185942.
Agency CI. The world factbook 2016. Central Intelligence Agency; 2016. https://www.cia.gov/the-world-factbook/.
Okunogbe A, Nugent R, Spencer G, Ralston J, Wilding J. Economic impacts of overweight and obesity: current and future estimates for eight countries. BMJ Glob health. 2021;6:e006351.
Goettler A, Grosse A, Sonntag D. Productivity loss due to overweight and obesity: a systematic review of indirect costs. BMJ Open. 2017;7:e014632.
Shiri R, Solovieva S, Husgafvel-Pursiainen K, Taimela S, Saarikoski LA, Huupponen R, et al. The association between obesity and the prevalence of low back pain in young adults: the Cardiovascular Risk in Young Finns Study. Am J Epidemiol. 2008;167:1110–9.
Gilmartin-Thomas JF, Cicuttini FM, Owen AJ, Wolfe R, Ernst ME, Nelson MR, et al. Moderate or severe low back pain is associated with body mass index amongst community-dwelling older Australians. Arch Gerontol Geriatr. 2020;91:104231.
Funding
This research is supported by ASPIRE, the technology program management pillar of Abu Dhabi’s Advanced Technology Research Council (ATRC), via the ASPIRE Precision Medicine Research Institute Abu Dhabi (ASPIREPMRIAD) award grant number VRI-20-10.
Author information
Authors and Affiliations
Contributions
DMM, FAA, and KK conceived the idea. DMM, FAA, and KK formulated the objective for this review. DMM designed the search strategy, conducted abstract screening and full text review, extracted the data, and drafted the manuscript. KK, FAA, and NK contributed to writing the manuscript. KK, FAA, and NK provided significant guidance on the content of the manuscript, overall supervision, and critical feedback. All authors contributed to the manuscript revision and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Menoth Mohan, D., Al Anouti, F., Kohli, N. et al. Association of obesity with musculoskeletal health and functional mobility in females—a systematic review. Int J Obes 49, 2184–2205 (2025). https://doi.org/10.1038/s41366-025-01881-8
Received:
Revised:
Accepted:
Published:
Version of record:
Issue date:
DOI: https://doi.org/10.1038/s41366-025-01881-8
