
Abstract
Background
Child cohort studies are important resources that can inform strategies to prevent adult noncommunicable diseases (NCDs). Technological advances now enable direct measurement of NCD-relevant phenotypes at large scale. Across contemporary large child cohorts, we aimed to provide the first comprehensive map of NCD-relevant phenotype measurement and gaps.
Methods
We included cohorts with >8000 child participants that were recruiting in whole or part after 2010 and measuring phenotypes relevant to ten high-burden NCDs. Our database and gray literature search identified 15 cohort studies for inclusion. Details on phenotype measurement (methods, age, location) are presented in an online, searchable inventory.
Results
All 15 cohorts measure body size or composition. Most cohorts measure aspects of cardiovascular health (n = 10) and neurocognition (n = 9). Fewer measure musculoskeletal phenotypes (n = 6), pulmonary function (n = 6), vision (n = 6) and glucose (n = 4). Only two cohorts measure hearing or kidney function.
Conclusions
Today’s childhood cohorts are not measuring some phenotypes important to global burden of disease, notably kidney function and hearing. Given the rarity of very large contemporary child cohorts, cross-cohort coordination will be required if all major NCD precursors are to be adequately represented for future benefit.
Impact
-
This scoping review provides a comprehensive overview of NCD-relevant phenotype measurement across large, modern child cohort studies.
-
This review has identified measurement gaps in important areas that may obviate steps to prevent and detect NCDs with high global disease burden.
-
Findings may inform planning of collaborative projects and future data collection to address measurement gaps for greatest future benefit.
Similar content being viewed by others

Introduction
Noncommunicable diseases (NCDs) are the leading cause of death worldwide, accounting for more than 70% of all deaths, and contribute enormously to global disease burden.1,2 In Australia, as in other high-income countries, approximately 90% of deaths are caused by NCDs.3,4 Ten conditions of aging account for 59% of global burden of disease in adults aged 75 and older: cardiovascular diseases (ischaemic heart disease, stroke and hypertensive heart disease, 31.6%), chronic obstructive pulmonary disease (COPD, 8.5%), Alzheimer’s disease (5.6%), diabetes mellitus (4.0%), fractures resulting from falls (2.6%), chronic kidney disease (2.5%), age-related hearing loss (2.5%) and blindness and vision loss (1.7%).2 Since 2010, gains in life expectancy in high-income countries have either plateaued or fallen, largely due to the rise of NCDs and their risk factors.5,6 Action is needed for prevention and early detection of NCDs but, to do this, we need to understand the life course trajectories to these conditions.
Cohort studies are valuable resources that, through measurements over time, capture the exposures, antecedents and outcomes of NCDs. Cohort studies that recruit participants during pregnancy, childhood or adolescence and track participants as they develop are well placed for discoveries that could elucidate life course phenotype trajectories that underlie adult NCDs.7 All cohort studies must make choices as to their areas of focus. As no one cohort can measure everything, it is important that collectively these resources span critical areas relating to current and future health. Concurrent burden of childhood disease/disability, wellness and salutogenesis are all vital research areas; another is measuring early life phenotypic pathways to later life disease – the focus of this paper. Phenotype trajectories reflect the functioning of various body systems (e.g., pulmonary function, neurocognitive function) across the life course at the organ level.8 They provide insights into the pathophysiological changes preceding later disease and highlight the role of early exposures and risk factors. Trajectories offer opportunities to study mechanisms for their positive disruption and to target interventions during optimal windows of growth, peak and decline.9
Many cohort studies now combine self- or proxy-reported measures with repeated face-to-face, direct measures. For some phenotypes, self-report measures are gold standard (e.g., mental health)10 while for others (such as height and weight), self- or proxy-reported measures align closely with objective measurement.11,12 However, many childhood phenotypic precursors to adult NCDs are not routinely measured in clinical care and are asymptomatic (and therefore not known to parents or children). Earlier cohort studies had limited access to sophisticated measurement tools, and therefore focused on easy-to-measure phenotypes such as blood pressure, height and weight. With technological advances, today’s cohort studies can now directly measure multiple phenotypes across multiple body systems, in depth and at scale. These advances in measurement capabilities provide opportunities to construct life course trajectories of phenotypes relevant to major adult NCDs and characterize their variations, timing and drivers.
While the etiologies of many adult NCDs are now reasonably understood, it is less clear how to effectively act to alter their etiologic pathways and estimate the potential benefits of doing so. Mega-cohorts such as UK Biobank (N = 500,000) have demonstrated that size is critical in detecting patterns,13 with sample sizes of approximately 10,000 needed to build accurate prediction models.14,15 However, cohort studies for children with these large sample sizes are rare. Furthermore, few (if any) cohort studies have the repeated measures needed to construct phenotype trajectories across the entire life course and, even if they did, the early life components would reflect circumstances from many decades ago. Increasingly, researchers are seeking to combine data from multiple cohort studies to answer complex life course research questions. Retrospective harmonization of data can be challenging due to measurement heterogeneity, particularly for self-reported survey data or measures of latent constructs because of differences in construct definitions.16,17 However, direct measures of physiological phenotypes are typically measured as single summary values that can be standardized as z-scores and harmonized more readily than survey data.18 Methods and tools have been developed, for example, to combine phenotype measurements from multiple cohort studies across different, but overlapping, age ranges to piece together trajectories and characterize their patterns across the life course.19 Collaborations among cohort studies offer the opportunity to leverage the rich datasets available and solve these public health challenges.20
To capitalize on existing resources and inform planning for new cohort studies, an understanding is needed of the NCD-relevant phenotypic data available from recently established, large-scale cohorts. Therefore, we seek to identify contemporary, large (N > 8000) children’s longitudinal cohorts to map their direct phenotype measurement. This will identify both strengths and gaps in life course measurement internationally that may be critical to understanding NCD development and later burden of disease. An understanding of measurement gaps in areas relevant to major NCDs could inform the design of future data collection waves, to prioritize areas in need of more longitudinal research. This could also guide future data harmonization and cross-cohort collaboration. Collaboration could bridge gaps in individual cohorts with the same measures at different ages, increase statistical power and precision through pooling, and characterize differences or similarities in trajectory patterns across different populations, geographic locations and socioeconomic contexts. These efforts will enable researchers to use the rich datasets that cohort studies have developed to solve cutting-edge questions and to drive change in public health policies and practice that is urgently needed to address the growing burden of NCDs.
Aims
The aims of this scoping review were to (1) identify large-scale, contemporary, population-based cohort studies that measure phenotypes relevant to major adult NCDs from childhood; (2) synthesize NCD-relevant phenotypes into a set of domains consistent across studies; and (3) provide a comprehensive overview of phenotype and domain measurement across studies, including the ages at which they are measured and the methods used to measure them. Through addressing these aims, we also intended to identify potential opportunities for data harmonization and collaboration across cohorts, and to identify gaps in the measurement of important health domains relevant to major NCDs.
Methods
This scoping review was conducted following the Joanna Briggs Institute (JBI) methodology for scoping reviews,21 with minor modifications to the screening process where appropriate. As recommended by the JBI, our scoping review follows the Preferred Reporting Items for Systematic Review and Meta-Analyses, Scoping Review extension (PRISMA-ScR) guidelines (see Supplementary Material S1 for PRISMA-ScR checklist).22 Scoping reviews are appropriate for addressing exploratory research questions where the aims are to synthesize evidence across a large body of literature, identify coverage, or to provide an overview of concept definitions.23 Systematic reviews are better suited to addressing specific research questions, for example about treatment efficacy.24 We chose to conduct a scoping review, rather than a systematic review, because it was the most appropriate review type to address our aims of mapping the phenotypes measured by cohort studies and identifying gaps. We pre-specified our scoping review’s aims, eligibility criteria and methodology in our protocol at https://osf.io/7a8hd.
Eligibility criteria
Participants
We included cohort studies that recruit participants in the pregnancy, perinatal or childhood periods, before age 20 years (the age when adulthood begins, as defined by the World Health Organization).25 We included cohort studies that draw participants from the general population (i.e., recruitment is not restricted to specific conditions or circumstances).
Concept
We considered cohort studies that directly measure (as opposed to self- or proxy-report) phenotypes relevant to the top 10 noncommunicable causes of global disease burden in adults aged 75 and above: cardiovascular diseases (ischaemic heart disease, stroke, hypertensive heart disease), COPD, Alzheimer’s disease, diabetes, accidental falls, chronic kidney disease, age-related hearing loss, and blindness and vision loss.2 We included falls (an injury) due to the life course influences of bone density and muscle strength on the likelihood of falls occurring and resulting in fracture.26 We excluded cancer both because it has a large stochastic component (i.e., begins with a random mutation) and, although many risk factors operate across the life course, clear intermediary phenotypes are not evident.27 We also excluded low back pain because it is usually episodic rather than progressive,28 and evidence is unclear regarding intermediary phenotypes that directly lead to it.29
Context
We included individual, recently-commencing cohort studies with a baseline sample of ≥8000 child participants. Although evidence suggests sample sizes >10,000 are needed to detect patterns and develop accurate risk prediction models for NCD-relevant phenotypes,14,15 a preliminary literature review indicated that limiting studies to those with sample sizes >10,000 would yield a small number of studies for inclusion, while >8000 identifies important additional studies. We considered cohort studies that recruit participants on an individual level (i.e., not household-level surveillance studies) and that cease recruiting during or after 2010.
Search strategy
Usually, searches are intended to identify individual studies reported in a single publication. However, cohort studies are specifically intended to generate multiple publications. Our search strategy was therefore designed to identify relevant cohort studies from which we could then identify relevant sources for data extraction. We ran database searches on 03 September 2024 in MEDLINE, Embase and PubMed (see Supplementary Material S2 for search strategy) that included the terms cohort ‘profile’ or ‘protocol’, which are publications that describe the methodology and participants of cohort studies. We also searched websites and study networks that list or catalogue cohort studies (Supplementary Material S2). We limited inclusion to cohort studies with publications in English, due to a lack of resources to translate materials; however, recruitment could be in any or many languages.
Study screening
Citations identified from the database search were uploaded to Covidence systematic review software30 and duplicates were removed using the in-built duplicate-removal function. Records were then dual-screened for inclusion by title and abstract. Following this, two authors independently reviewed all potentially relevant texts in full. Disagreements were resolved through discussion between the two reviewers and, if an agreement could not be reached, were resolved through discussion with the wider research team (i.e., authors of this paper).
Websites and study networks were manually reviewed by one author, following a pilot where two authors reviewed two websites independently to check for consensus. Eligible cohort studies identified from websites and study networks were listed in an Excel document.
Data extraction
We developed a data extraction form in Qualtrics.31 The data extraction form was piloted and iteratively revised. As cohort studies often have many associated publications and materials from which to extract relevant information, data was extracted from multiple sources (see Supplementary Material S3). Where available, data extraction was prioritized from published cohort protocols and profiles. Individual cohort study websites were also important resources for data extraction, particularly if the website contained data collection protocols, a data dictionary, or described the measurements collected. If these sources did not yield sufficient evidence, relevant publications were identified through a Google Scholar search for publications that used data from the cohort study and described the data collection methods. If information was still unclear, we contacted the cohort study directly for clarification.
The data extracted included the study aim(s) and focus, recruitment details, sampling frame, sample size, study location, data access, and phenotype measurement (including the specific phenotype, participant age at measurement and methods used). We extracted information on the measurement of phenotypes relevant to our NCDs of interest defined above (see ‘Concept’ section). We extracted direct measurements only, except for measures of body size or composition, where both direct and reported measures were extracted. This was done because self- and parent-reported measures of body size or composition (such as height and weight) have been shown to have a high level of accuracy.11,12
Evidence synthesis
The characteristics of each cohort study, including the location, focus, sampling frame, recruitment details, sample size, data collection, and data access were summarized. We synthesized phenotypes into nine overarching domains, with domains corresponding to body systems relevant to our NCDs of interest (see ‘Concept’ section). The domains included cardiovascular health (relevant to cardiovascular diseases), pulmonary function (COPD), the musculoskeletal system (falls), vision (blindness and vision loss), neurocognition (Alzheimer’s disease), kidney function (chronic kidney disease), hearing (age-related hearing loss), glucose control (diabetes) and body size or composition (relevant to most NCDs). The domains measured in each of the cohorts across childhood were summarized in a figure, to provide a domain-level overview of coverage and gaps. Additionally, we created an interactive, searchable table with more detail on the measurement of specific phenotypes using the Shiny package in R 4.3.0.32,33
Results
Search and study characteristics
The database search identified 214 articles in PubMed, 686 in Ovid MEDLINE and 1164 in Embase. After removing duplicate records, we screened 1290 articles by title and abstract and excluded 1058 articles. We then reviewed the full texts of the remaining 232 articles and identified 9 cohort studies for inclusion in this review. Our review of websites and study networks identified 1714 records. Duplicates could not be automatically removed and were instead removed manually during the screening process. We excluded 1708 records and identified an additional 6 unique cohort studies. Figure 1 shows the study screening and selection process.

Source: Page MJ, et al. BMJ 2021;372:n71. https://doi.org/10.1136/bmj.n71.
Table 1 lists the cohorts and summarizes the characteristics of the identified large children’s life course phenotypic cohorts. Their international rarity is immediately evident. We identified only 15 such cohorts recruiting since 2010,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48 of which only seven commenced in the last decade. Most of the included cohort studies are birth cohorts (n = 9), recruiting participants either during pregnancy or soon after birth. Most of the cohort studies are located in high-income countries (n = 11), with three based in Japan and one based in each of the USA, UK, France, Finland, Australia, South Korea, the Netherlands and Norway.49 One study is based in Iran (lower middle income) and the remaining three are based in China (upper middle income).49 The baseline sample sizes of the included cohort studies ranged from 8066 (Young-HUNT4) to 100,148 (Japan Environment and Children’s Study) child participants.
Measurement of NCD-relevant phenotypes and domains
Figure 2 summarizes the domain-level phenotype measurements in each cohort study against age, and Table 2 summarizes their specific phenotypes measured. A more detailed overview of these phenotypes within each domain, including the age(s) at which they are measured, the measurement tools used and the location of data collection, is provided in an interactive, searchable table accessible via this link: https://katiemcbain.shinyapps.io/Cohortmeasures/.

1BIGCS measures vision at precise ages. The vision measurement at age 6 years is standalone, unlike the other domains at that age which are measured in children >6 years of age. 2CPCD plans to repeat measures at annual school physical examinations. 3The Hokkaido Birth Cohort comprises two separate birth cohorts with some differences in the phenotypes and ages measured in each. See Shiny app for more details. 4Some measures in JECS are conducted in the sub-cohort only. See Shiny app for more details. The measures at age 10 and 12 years are planned. 5In Lifelines, some phenotypes are measured at the baseline assessment and are repeated at the second assessment, whereas others are only measured in one assessment. See Shiny app for more details. 6The PERSIAN birth cohort plans to measure neurocognition but has not specified the age(s) when this will be measured. It is therefore missing from this figure, but is included in Table 2 and in the Shiny app. In addition to directly measuring body size or composition at the ages shown on this figure, body size or composition is also collected every 2 months from the participant’s logbook, and no end date has been specified.
Cardiovascular
Cardiovascular health is measured by ten of the 15 cohort studies on at least one occasion. Measurement spans from age 1–19 years, with a gap at age 3-4. All ten of these studies measure blood pressure, while five also measure pulse rate and two measure heart rate variability using an electrocardiogram.
Pulmonary
Six of the cohort studies measure pulmonary function, but only two measure it repeatedly. Collectively, pulmonary function is measured from age 6–17 years. Two of the cohort studies measure lung function using spirometry, one measures vital capacity instrumentally, two assess airway inflammation using exhaled nitric oxide (FeNO) and two measured lung or respiratory function but did not specify the measurement tool used.
Musculoskeletal
Musculoskeletal phenotypes are measured by six cohort studies, collectively from age 6 years. Specific musculoskeletal phenotypes measured by the cohort studies include bone density, which is measured using dual x-ray absorptiometry (DEXA) by two studies and calcaneal ultrasound imaging by one study; muscle mass, which is measured using DEXA by one study and bioimpedance by two studies; strength, which is measured using a jump test by one study; and grip strength, which is measured by three studies.
Vision
Vision is measured by six cohort studies, collectively from the first year of life to age 16 years. Within this domain, visual acuity is measured by four studies, eye refraction by two studies and axial length by one study. One study describes assessing vision through vision screening but did not provide details on the exact measures used.
Neurocognition
Nine of the cohorts have measured neurocognition at least once. Together, cohorts that measure neurocognition assess this domain each year from the first year of life to age 17 years, excluding age 5–6 years. Cohort studies measuring neurocognition use a wide range of measures that assess many different phenotypes, with very few occasions of the same measure being used in multiple cohort studies; in total, we identified 53 unique measures in this domain. Of the six cohort studies that measured the subcategory of neurodevelopment, two use the Ages and Stages Questionnaire, two use the Denver Developmental Screening Test, and two use the Bayley Scales of Infant Development. Of the three cohort studies that measure intelligence, all use the Weschler Intelligence Scale for Children, alongside other measures.
Kidney
Two of the cohort studies measure kidney function, with one study measuring it on two occasions in children aged between 8 and 17 years and the other measuring it at age 7 years. One study measures kidney function through measures extracted from urine samples (albumin and creatinine) and blood (urea and uric acid). Both studies extract measures of creatinine from blood samples (enabling estimation of glomerular filtration rate, eGFR).
Body size or composition
All 15 cohort studies measure body size or composition on at least one occasion, and all but two do so repeatedly. Collectively, the cohort studies measure body size or composition every year from birth to age 19 years. Specific phenotypes measured within this domain vary and include anthropometric measurements (e.g., weight, height, waist circumference, arm circumference, skinfold thickness), bioimpedance and DEXA body scans. Of the five cohort studies that include self- or parent-reported anthropometric measurements, three of them also include direct, in-person measurements.
Hearing
Hearing is measured by two of the cohort studies, spanning ages 0-1, 5-6, 10-11 and 16-17 years. Hearing is measured using an auditory test by one study, and the other study states it measures hearing acuity but not the measure used.
Glucose control
Glucose control is measured by four cohort studies, collectively spanning age 5, 6 and 8–17 years. Of the four studies that measure phenotypes in this domain, all four measure HbA1c, two measure blood glucose, one measures blood insulin and one measures blood glycoalbumin.
Summary of measurement coverage and gaps
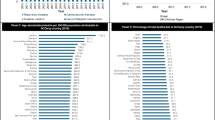
The health domains measured by the most cohort studies are body size or composition, cardiovascular health and neurocognition. These are also the domains with the greatest number of studies measuring them on at least two occasions (Fig. 3). Measurement across the cohort studies also spans the longest childhood age range for these three domains. The most diversity of phenotype measures is in the neurocognition domain, which may limit cross-cohort analyses.

a Cohort studies that repeat measurement, ranked from least to most domains repeated. b Domains measured on at least two occasions, ranked from least to most repeated domains.
The health domains measured by the fewest number of cohort studies are hearing and kidney function. These are also the domains with the fewest number of cohort studies repeating measurement on at least one other occasion, alongside the musculoskeletal domain.
Data access across cohorts
All of the included cohort studies describe how data can be accessed. Only one specifically describes being Open Access. Details on data access for each study are summarized in Table 3.
Discussion
Principal findings
This is the first scoping review to provide a comprehensive overview of phenotype and domain measurement in large, population-based child cohort studies. We identified 15 cohort studies that directly measure phenotypes relevant to major adult NCDs from childhood. Body size or composition is the most widely measured domain across the cohort studies, closely followed by cardiovascular health and neurocognition. Less than half of the cohort studies measure phenotypes within the domains of musculoskeletal function, pulmonary function, vision and glucose control. Hearing and kidney function are measured by only two cohort studies. Phenotypes measured across several cohorts offer opportunities for collaboration and data harmonization, spanning multiple years in childhood. Our review has identified gaps in the measurement of other important phenotypes, which limit opportunities to map their trajectories and to address research questions targeting these phenotypes and their relevant NCDs. Findings from this review may assist in the planning and design of future cohort studies and analyses.
Strengths and limitations
A strength of this scoping review is that we not only searched for eligible cohort studies via publications on databases, but we also searched gray literature in the form of websites (including study registration sites) and study networks. This enabled us to find cohort studies that have not yet published cohort protocols or profiles, particularly newer studies that are not yet at the stage of sharing these publications, such as GenV. By focusing on major adult NCDs that contribute to global disease burden, we have highlighted the phenotypic data available in childhood to address major population challenges. Our interactive, searchable Shiny app table, allows researchers and other stakeholders interested in these data to readily search for and identify cohort studies with relevant measurements, facilitating collaboration or the wisdom of plugging gaps at the earliest opportunity.
This scoping review also has limitations. Some cohort studies may not have yet publicly shared details of all data collection waves, and others may have changed plans shared in earlier publications. Researchers seeking to use the data described in this review should verify details through direct contact with the relevant cohort studies and reviewing technical documents where available in data access portals. Large cohort studies are expensive to run and are funded for short periods at a time, meaning that data collection is planned in stages, focusing on funded age ranges. Because we reviewed contemporary studies, some of the newer studies recruiting participants at birth (such as GenV) are only beginning to collect measurements early in the life course, whereas other studies (such as the ABCD Study) have already collected measures in older age ranges. The most widely measured health domains in the older childhood years, and the most often repeated measures, may shift over time as younger participants in newer cohort studies reach those later ages.
Interpretation of findings and implications
It is not surprising that the most widely-measured phenotypes across these cohort studies fall within the domains of body size or composition, cardiovascular health and neurocognition. These domains are relevant to later life conditions with high burden of disease – cardiovascular disease is the leading cause of global disease burden from age 50 years onwards, while Alzheimer’s disease is the fourth highest contributor in adults 75 and over.2 Childhood overweight and obesity is a major public health challenge in many countries and is a recognized risk factor for many adult NCDs.50 These three health domains can be measured using a variety of tools, including those that are fast, non-invasive and affordable, such as body mass index via anthropometry or blood pressure via sphygmomanometer. These measures are well suited to large-scale, population-based research, and were the dominant measures used across the cohort studies in this review. Other important measures of these domains that are invasive, costly, time-consuming or bulky, such as carotid-artery intima-media thickness, were completely absent from these very large cohort studies. This highlights the importance of low-cost, low burden measures for these types of studies.
Where phenotypes are measured widely and at multiple ages throughout childhood, our findings suggest that there are opportunities for cross-cohort collaboration and data harmonization. Pooled data analysis could be undertaken, for example, to construct phenotype trajectories that include datapoints at most, if not all, of the childhood years for body size or composition, neurocognition and cardiovascular phenotypes. This could be done using methods that allow trajectories to be developed from multiple cohorts spanning different, but overlapping, age ranges, such as those developed by Hughes et al.19 As measures of body size or composition are regularly repeated across the cohort studies, trajectories could be compared across cohorts to investigate the role of contextual influences such as socioeconomic factors, environmental conditions, or policies.
We did not include umbrella initiatives bringing together multiple smaller cohorts. For example, the ~60,000 children in the USA-based Environmental influences on Child Health Outcomes (ECHO) Cohort51 come from 69 individual cohorts that vary in decade, geography and life stage at recruitment and who they represent (general population or at high risk of a targeted condition), with no single participating cohort individually meeting our pre-specified inclusion criteria. We fully acknowledge that ECHO’s standardized prospective measurement52 of heart rate, blood pressure, body composition and anthropometry, neurodevelopment and lung function (via spirometry) will further strengthen phenotypic data beyond that reported in our review.
While this scoping review has identified promising opportunities for collaboration and pooled analyses, we have also identified notable gaps in the measurement of health domains relevant to burden of disease. Cohort studies represent significant investments in population health and provide important opportunities to identify prevention strategies, but today’s large child cohorts are not capturing the precursors to some high-burden adult NCDs. This will limit our ability to understand early life trajectories to these important conditions of ageing. There may be several reasons for these measurement gaps, relating to the invasiveness, costs, or time involved in measuring some domains and phenotypes. Hearing can be challenging to measure, particularly in large cohort studies which aim to measure multiple aspects of health in often short timeframes. Pure tone audiometry, the gold standard for measuring hearing, can be expensive and time-consuming, and traditionally has required a sound-proof environment, all of which are limiting for large-scale studies.53 The sparse measurement of this domain provides a rationale for new measures to be developed that are better suited for large-scale, population-based research. Kidney function, along with glucose control, are measured through biospecimen collections (blood and urine). Many of the cohort studies included in this review collect and store bio-samples, including urine and blood, but we have only reported on those that described extracting measures of either kidney health or glucose control. The reported gaps in measurement in these domains may therefore reflect either a low priority or the high cost and logistics of bioassays to extract measures from collected and stored samples. Therefore, stored samples reflect a further opportunity, as funding becomes available, to redress some of these gaps.
Future research
This review highlights opportunities for analyses combining data from multiple studies, so that these important resources can become knowledge as soon as possible. There are also opportunities for future research to integrate these phenotypic measurements (phenome) with other multi-omic techniques to strengthen causal inference and enhance understanding of NCD prevention, including through personalized preventive approaches.54,55 While we have focused on large cohorts, sub- or nested cohorts offer rich and immediate opportunities for detailed analyses such as bioassays that may later become available to larger cohorts as technology and costs allow. Future cohort studies, or cohort studies planning data collection waves, may also use our findings to guide their planning. This can enable collaboration or address some of the measurement gaps identified. Launching and planned cohorts have the opportunity to address gaps by drawing on new imaging, wearable and adaptive technologies.56,57,58
This scoping review focused on a range of organ-level physiological phenotypes within nine high-level domains relevant to major adult NCDs of ageing. Future reviews may focus on risk factors for adult NCDs (e.g., physical activity), measures relevant to different areas (e.g., child health conditions) or an area in greater detail and including, for example, smaller cohort studies that may have more concentrated aims. Future reviews may look at phenotypes measured in adult cohorts, particularly as midlife is another important transitional period for health trajectories.59 Future research is also needed to identify or create cost-effective, low-burden measures that are suitable for large-scale research. Currently, it appears that limitations in the measures available to large cohorts may limit the translational evidence these studies can generate and that is needed to reduce future disease burden.
Conclusions
We have mapped the availability and gaps in phenotypes relevant to major adult NCDs measured by contemporary large-scale child cohort studies. The widely-measured domains of body size or composition, neurocognition, and cardiovascular health offer opportunities for data pooling and harmonization that could support larger sample sizes, comparison across cohorts, or bridge gaps in individual cohorts by combining the same measures at different ages. However, for some important domains phenotypes are lacking (notably kidney function and hearing). If these gaps are not addressed, the enormous investments in these cohort studies will not adequately inform understanding of pathways to substantive portions of disease burden. Cross-cohort planning to measure key phenotypes within underrepresented domains could address these gaps. This will ensure that all major NCD precursors are adequately represented over time for greatest future benefit.
Data availability
All relevant data are included in this manuscript and its supplementary information files.
References
Hadian, M., Mozafari, M. R., Mazaheri, E. & Jabbari, A. Challenges of the health system in preventing non-communicable diseases; systematized review. Int J. Prev. Med. 12, 71–71 (2021).
GBD 2019 Diseases and Injuries Collaborators. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet. 396, 1204–1222 (2020).
GBD 2019 Australia Collaborators. The burden and trend of diseases and their risk factors in Australia, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet Public Health. 8, e585–e599 (2023).
World Health Organization. Noncommunicable diseases country profiles 2018. (2018). Available at: https://www.who.int/publications/i/item/9789241514620.
Mehta, N. K., Abrams, L. R. & Myrskylä, M. US life expectancy stalls due to cardiovascular disease, not drug deaths. Proc. Natl Acad. Sci. USA 117, 6998–7000 (2020).
Lopez, A. D. & Adair, T. Slower increase in life expectancy in Australia than in other high income countries: the contributions of age and cause of death. Med. J. Aust. 210, 403–409 (2019).
Power, C., Kuh, D. & Morton, S. From developmental origins of adult disease to life course research on adult disease and aging: insights from birth cohort studies. Annu. Rev. Public Health 34, 7–28 (2013).
Kuh, D. et al. in The New Dynamics of Ageing The New Dynamics of Ageing (Walker, A. ed.) 59–80 (Bristol University Press, 2018).
Ben-Shlomo, Y., Cooper, R. & Kuh, D. The last two decades of life course epidemiology, and its relevance for research on ageing. Int. J. Epidemiol. 45, 973–988 (2016).
Croarkin, P. E. et al. Performance and psychometric properties of novel brief assessments for depression in children and adolescents. JAACAP Open (2024).
Chai, L. K., Collins, C. E., May, C., Holder, C. & Burrows, T. L. Accuracy of parent-reported child height and weight and calculated body mass index compared with objectively measured anthropometrics: secondary analysis of a randomized controlled trial. J. Med. Internet Res. 21, e12532 (2019).
Olfert, M. D. et al. Self-reported vs. measured height, weight, and BMI in young adults. Int. J. Environ. Res Public Health 15, 2216 (2018).
Littlejohns, T. J., Sudlow, C., Allen, N. E. & Collins, R. UK Biobank: opportunities for cardiovascular research. Eur. Heart J. 40, 1158–1166 (2019).
Schulz, M. A. et al. Different scaling of linear models and deep learning in UK Biobank brain images versus machine-learning datasets. Nat. Commun. 11, 4238 (2020).
Pate, A., Emsley, R., Sperrin, M., Martin, G. P. & van Staa, T. Impact of sample size on the stability of risk scores from clinical prediction models: a case study in cardiovascular disease. Diagn. Progn. Res. 4, 14 (2020).
Sharma, V. et al. Evaluating the harmonization potential of oral health-related questionnaires in national longitudinal birth and child cohort surveys. J. Public Health Dent. 84, 307–320 (2024).
Gatz, M. et al. Data harmonization in aging research: not so fast. Exp. Aging Res. 41, 475–495 (2015).
Ullah, A. et al. Obstructive and restrictive spirometry from school age to adulthood: three birth cohort studies. EClinicalMedicine 67, 102355 (2024).
Hughes, R. A., Tilling, K. & Lawlor, D. A. Combining longitudinal data from different cohorts to examine the life-course trajectory. Am. J. Epidemiol. 190, 2680–2689 (2021).
O’Connor, M. et al. Better together: advancing life course research through multi-cohort analytic approaches. Adv. Life Course Res. 53, 100499 (2022).
Peters, M. D. J. et al. Updated methodological guidance for the conduct of scoping reviews. JBI Evid. Synth. 18, 2119–2126 (2020).
Tricco, A. C. et al. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann. Intern Med. 169, 467–473 (2018).
Peterson, J., Pearce, P. F., Ferguson, L. A. & Langford, C. A. Understanding scoping reviews: definition, purpose, and process. J. Am. Assoc. Nurse Pr. 29, 12–16 (2017).
Munn, Z. et al. Systematic review or scoping review? Guidance for authors when choosing between a systematic or scoping review approach. BMC Med. Res. Methodol. 18, 143 (2018).
World Health Organization. Adolescent Health. Available from: https://www.who.int/health-topics/adolescent-health#tab=tab_1.
Lems, W. F. & Raterman, H. G. Critical issues and current challenges in osteoporosis and fracture prevention. An overview of unmet needs. Ther. Adv. Musculoskelet. Dis. 9, 299–316 (2017).
Davey Smith, G. Post-modern epidemiology: when methods meet matter. Am. J. Epidemiol. 188, 1410–1419 (2019).
Hartvigsen, J. et al. What low back pain is and why we need to pay attention. Lancet 391, 2356–2367 (2018).
Herlin, C. et al. Modic changes-their associations with low back pain and activity limitation: a systematic literature review and meta-analysis. PLoS ONE 13, e0200677 (2018).
Covidence Systematic Review Software (Veritas Health Innovation, Melbourne, Australia). Available at: https://www.covidence.org/.
Qualtrics software. Copyright © 2024 Qualtrics. (Provo, UT, USA, 2023). Available at: https://www.qualtrics.com.
Chang, W. et al. Shiny: web application framework for R. (R package version 1.8.0.9000, 2024). Available at: https://github.com/rstudio/shiny.
R Core Team. R: a language and environment for statistical computing. (R Foundation for Statistical Computing, Vienna, Austria, 2023).
Jernigan, T. L., Brown, S. A. & Dowling, G. J. The adolescent brain cognitive development study. J. Res Adolesc. 28, 154–156 (2018).
Raynor, P. Born in Bradford, a cohort study of babies born in Bradford, and their parents: protocol for the recruitment phase. BMC Public Health 8, 327 (2008).
Qiu, X. et al. The Born in Guangzhou Cohort Study (BIGCS). Eur. J. Epidemiol. 32, 337–346 (2017).
Zhao, L., Shek, D. T. L., Zou, K., Lei, Y. & Jia, P. Cohort profile: Chengdu Positive Child Development (CPCD) survey. Int J. Epidemiol. 51, e95–e107 (2022).
Charles, M. A. et al. Cohort Profile: The French National Cohort of Children (ELFE): birth to 5 years. Int. J. Epidemiol. 49, 368–369j (2020).
Figueiredo, R. A. O. et al. Cohort profile: the Finnish Health in Teens (FIN-HIT) study: a population-based study. Int J. Epidemiol. 48, 23–24h (2019).
Wake, M., Goldfeld, S. & Davidson, A. Embedding life course interventions in longitudinal cohort studies: Australia’s GenV opportunity. Pediatrics 149, e2021053509R (2022).
Kishi, R. et al. Cohort profile: the Hokkaido Study on Environment and Children’s Health in Japan. Int J. Epidemiol. 40, 611–618 (2011).
Michikawa, T. et al. Baseline profile of participants in the Japan Environment and Children’s Study (JECS). J. Epidemiol. 28, 99–104 (2018).
Jeong, K. S. et al. Cohort profile: beyond birth cohort study - the Korean Children’s Environmental Health Study (Ko-Chens). Environ. Res. 172, 358–366 (2019).
Scholtens, S. et al. Cohort profile: Lifelines, a three-generation cohort study and biobank. Int J. Epidemiol. 44, 1172–1180 (2015).
Zare Sakhvidi, M. J. et al. The Prospective Epidemiological Research Studies in Iran (PERSIAN) Birth Cohort protocol: rationale, design and methodology. Longitud. Life Course Stud. 12, 241–262 (2021).
Wang, X. et al. Cohort profile: the Shanghai Children’s Health, Education and Lifestyle Evaluation, Preschool (SCHEDULE-P) study. Int. J. Epidemiol. 50, 391–399 (2021).
Kuriyama, S. et al. Cohort profile: Tohoku Medical Megabank Project Birth and Three-Generation Cohort Study (TMM BirThree Cohort Study): rationale, progress and perspective. Int. J. Epidemiol. 49, 18–19m (2020).
Holmen, T. L. et al. Cohort profile of the Young-HUNT Study, Norway: a population-based study of adolescents. Int. J. Epidemiol. 43, 536–544 (2014).
The World Bank. The World by Income and Region. (2022). Available at: https://datatopics.worldbank.org/world-development-indicators/the-world-by-income-and-region.html.
Nishtar, S., Gluckman, P. & Armstrong, T. Ending childhood obesity: a time for action. Lancet 387, 825–827 (2016).
Knapp, E. A. et al. The Environmental influences on Child Health Outcomes (ECHO)-Wide Cohort. Am. J. Epidemiol. 192, 1249–1263 (2023).
ECHO Program Materials. Environmental influences on Child Health Outcomes (ECHO) Cohort data and biospecimen collection protocol. (version 3.0, 2023). Available at: https://echochildren.org/protocol-and-mop/.
Oosterloo, B. C. et al. Assessing hearing loss in older adults with a single question and person characteristics; comparison with pure tone audiometry in the Rotterdam study. PLoS ONE 15, e0228349 (2020).
Noble, A. J. et al. A final frontier in environment-genome interactions? integrated, multi-omic approaches to predictions of non-communicable disease risk. Front Genet. 13, 831866 (2022).
Farina, S. et al. The current landscape of personalised preventive approaches for non-communicable diseases: a scoping review. PLoS ONE 20, e0317379 (2025).
Wu, C. T. et al. A Precision health service for chronic diseases: development and cohort study using wearable device, machine learning, and deep learning. IEEE J. Transl. Eng. Health Med. 10, 2700414 (2022).
Huhn, S. et al. The impact of wearable technologies in health research: scoping review. JMIR Mhealth Uhealth 10, e34384 (2022).
Doherty, A. et al. Large scale population assessment of physical activity using wrist worn accelerometers: the UK Biobank study. PLoS ONE 12, e0169649 (2017).
Infurna, F. J., Gerstorf, D. & Lachman, M. E. Midlife in the 2020s: opportunities and challenges. Am. Psychol. 75, 470–485 (2020).
Acknowledgements
The authors would like to thank Ms. Poh Chua for her assistance with developing the database search strategy for this review. Research at the Murdoch Children’s Research Institute is supported by the Victorian Government’s Operational Infrastructure Support Program. KM was supported by a PhD stipend funded by Australian National Health & Medical Research Council (NHMRC) Ideas GNT1186123. DD was funded by an Australian Research Council Discovery Early Career Award (DECRA) DE230101174 and by the Center of Research Excellence in Driving Global Investment in Adolescent Health funded by NHMRC GNT1171981. AS was supported by funding from the Royal Australasian College of Physicians, the University of Melbourne and the Murdoch Children’s Research Institute. MW was supported by NHMRC Principal Research Fellowship 1160906.
Funding
Open access funding provided by Royal Children's Hospital (RCH), Victorian Health Libraries Consortium (VHLC).
Author information
Authors and Affiliations
Contributions
KM, DD, AS, SC, TO and MW contributed to conception and design, acquisition of data, or analysis and interpretation of data. KM drafted the manuscript, and all authors revised it critically for important intellectual content. All authors approved the final version to be published.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
McBain, K., Dumuid, D., Shipton, A. et al. A scoping review of adult NCD-relevant phenotypes measured in today’s large child cohort studies. Pediatr Res 98, 2058–2072 (2025). https://doi.org/10.1038/s41390-025-04056-3
Received:
Revised:
Accepted:
Published:
Version of record:
Issue date:
DOI: https://doi.org/10.1038/s41390-025-04056-3
