
Abstract
Background
We studied whether ozone (O3) exposure will affect the occurrence of KD, in Xiamen.
Methods
A time-stratified case-crossover design was conducted to explore the relationship between O3 exposure and KD in children. A total of 604 participants from 2017 to 2024 were included. Artificial intelligence technology combined with large data model was used to calculate O3 concentration, and O3 exposure was assigned to each participant. Poisson generalized additive model was used to calculate the risk effect of O3 and KD. Correlation and mediation analysis were used to study the mechanism of KD.
Results
When lag 2 to 6 days, O3 exposure will increase the occurrence of KD. On the 4th day of lag, O3 led to the highest risk of KD, relative risk(RR) = 1.09(95%CI = 1.008, 1.19). The results of mediation analysis showed that clinical indicators such as white blood cell (WBC), neutrophil (NEUT), and C-reactive protein (CRP) were the main mediators regulating the association between O3 and KD.
Conclusion
Our results show that exposure to O3 is a potential risk factor for KD in children, and clinical indicators such as WBC, NEUT, PLT and CRP are the main mediators regulating O3 and KD.
Impact
-
We studied the association between O3 exposure and the incidence of KD, and further analyzed the regulatory role of clinical indicators in this association. On the 4th day of lag, O3 led to the highest risk of KD, RR = 1.09(95%CI = 1.008,1.19). The relationship between O3 exposure and KD is mainly mediated by clinical indicators such as WBC, NEUT, PLT and CRP.
-
Our findings explain the association between O3 exposure and the incidence of KD, and further analyze the regulatory role of clinical indicators in the association. It is helpful to provide theoretical support for subsequent research.
Similar content being viewed by others


Introduction
KD is a childhood acute febrile systemic vasculitis disease, which occurs in the coronary artery and may lead to coronary dilatation, aneurysm and thrombosis.1 KD mainly affects children aged 6 months to 5 years old. It is the main cause of acquired heart disease in children in developed countries and is becoming the main factor of acquired heart disease in developing countries.2,3 The global incidence of KD is 100/100,000 per year. In Japan, the incidence rates in 2015 and 2016 were 330.2/100,000 and 309.0/100,000, respectively.4,5 However, the incidence rate in China from 2013 to 2017 was 68.8/100,000 to 107.3/100,000, showing an increasing trend.6
Related studies have shown that air pollutants such as O3, PM2.5 and PM10 can increase the incidence of diseases such as respiratory system, cardiovascular system, and autoimmune system, and ultimately lead to increased mortality in children.7,8 Lin et al. used the generalized additive model combined with the distributed lag nonlinear model to estimate the impact of daily air pollutants on the incidence of KD. The results showed that there was a positive correlation between the incidence of KD and the three main air pollutants, PM10, SO2 and NO2.2 A case-control study from 2004 to 2010 in Taiwan, collected 4192 cases of KD, randomized controlled at a ratio of 1:4, the results also showed that CO, NO, NO2 were positively correlated with the incidence of KD.9
At present, there is still a lack of research on the effect of O3 on the pathogenesis of KD.10 In this study, we investigated the association between O3 exposure and KD incidence and found the main clinical mediators that regulate the association between O3 and KD in Xiamen, China for 8 years. It is hoped that it will help readers to understand the possible mechanism and etiology of KD.
Methods
Data sources and quality control
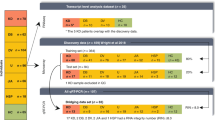
After excluding the clinical data of atypical and incomplete KD, the clinical data of 604 children with typical KD were collected in Xiamen, China, from January 1,2017 to October 1,2024. We conducted a case-cohort study, followed up pediatric patients regularly, and collected their residential addresses, medical data, demographic status, comorbidities, and other anthropometric and laboratory information (Figs. 1, 2). All participants provided written informed consent at the time of recruitment. The study protocol was approved by the Medical Ethics Committee of Xiamen Maternal and Child Health Hospital (3502Z20224ZD1235).

Flow diagram of the study.

The distribution map of participants in this study.
The current diagnostic criteria for typical KD is persistent fever (≥5days) and at least four of the five clinical symptoms: (1)oral erythema; (2)bilateral conjunctival congestion; (3)rash (maculopapule, diffuse erythroderma, polymorphic erythema); (4)hand and foot erythema/edema/ desquamation; (5)cervical lymphadenopathy.11 The disease was coded using the 11th revised edition of the International Classification of Diseases(ICD-11; WHO 2024).12
Exposure assessment
The air pollution dataset comes from China High Air Pollutants (CHAP), a high-resolution near-surface air pollutant dataset in China. The dataset is produced by using artificial intelligence technology, surface solar radiation intensity and air temperature as the main predictors, combined with large data such as ground air pollution monitoring station monitoring data, atmospheric reanalysis and pollutant emission inventory.13 Finally, the daily average pollutant exposure concentration at a spatial resolution of 1 km was established. Random 10-fold cross-validation R2 value was 0.86.14 Based on the residential address of the child, we obtain the geographical coordinates, and use Arcmap10.3 software to perform spatial location matching to calculate the pollutant concentration of each participant’s residence, and obtain the corresponding spatial location pollutant value.
Study design and statistical analysis
The association between air pollutants and KD was studied using a time-stratified case-crossover design. This research design can control confounding factors and risks that change over time in the short term.15,16 The case group was used as its own control group to avoid the deviation of exposure on different dates.17 It can also control all known and unknown confounding factors, such as age, weight, socio-economic factors and genetic predisposition. Time series methods have been widely used to study the impact of the environment on adverse health outcomes.2,18
Poisson generalized additive model was used to analyze the influence of daily weather conditions on the occurrence of KD. The model can be applied to linear and nonlinear models, and has the advantages of interpretability, flexibility and regularization.19 In order to consider the time lag effect of various exposures, the lag time is from the day of fever to 8 days ago, that is, to study the effect of 0–8 days lag of O3 on the occurrence of KD.
In stratified analyses, we considered factors such as sex (male/female), age group (<1year, ≥1year), and school attendance (yes, no) to assess associations in important subgroups. Before considering the multi-pollutant model, we calculated the Spearman correlation between air pollutants. If the correlation coefficient between the two exposed variables is too high (more than 0.7), it is excluded from the analysis.20 Directed acyclic graph (DAG) is an intuitive and rigorous tool to identify variables. Controlling variables at the design or analysis stage is sufficient to eliminate confounding factors and some forms of selection bias, and is often used to evaluate causal problems in clinical and epidemiological studies.21,22 After referring to the relevant literature of previous studies, we used DAG to evaluate the confounding factors, and considered the following covariates into the final model: age, sex, past history, comorbidities and so on23,24,25 (Fig. 3). In order to determine the causal mediating effect of clinical indicators, we conducted mediating analysis to study the mechanism of KD, and calculated the average direct effect (ADE), the average causal mediating effect (ACME) value and the total effect value (TE).26

Directed acyclic graph of KD and related risk factors.
Sensitivity analyses
Firstly, the crude model only included the association between O3 exposure concentration and KD in children. Model 1 adjusted for age, sex, medical history, blood routine, and other factors based on the crude model; in Model 2, considering the deterioration of air quality due to population migration and extensive firecrackers during the Lunar New Year, we excluded the data of 40 days before and after New Year’s Eve and re-estimated the O3 concentration.27 Model 3 Because other air pollutants, such as PM2.5, PM10 and temperature, may also affect the occurrence of KD, we adjusted it into the multi-pollutant model.28,29 In Model 4, considering that microbial infection may also lead to KD, we excluded participants with infection-induced disease and reanalyzed the association between O3 and KD.30
Two-tailed probability P < 0.05 was considered statistically significant. All analyses were performed using R software version 4.0.5 with software packages “dlnm”, “splines”, “tsModel”, “forestploter” and so on.
Results
Characteristics of participants
A total of 604 children with KD were included in this study. 131 subjects were excluded according to the following criteria: (1)Lack of specific address information (n = 38); (2)Participants were older than 16 years(n = 44); (3)Patients who were lost to follow-up (n = 17); (4)repeated participants (n = 6); (5)Lack of clinical data (n = 26) (Fig. 1). As a result, a total of 473 subjects were available for analysis. Table 1 shows the descriptive characteristics of the participants in the study, with an average age of 1 year and 2 months. The maximum number of children aged 1 to 3 years old was 313(66.11%), of which male children were more than female children, and male children were 289(61.09%). The number of children attending school is low, at 101(21.34%). The median O3 exposure concentration on the first day was 101.55 (81.93,178.5) μg/m3.
Correlation analysis of air pollutants and meteorological factors
The correlation between pollutants and meteorological factors was analyzed. The results showed that there was a negative correlation between temperature and wind speed (P < 0.05), and the correlation coefficient was −0.21. O3 was positively correlated with wind speed (P < 0.05), and the correlation coefficient was 0.28. There was a positive correlation between PM2.5 and O3 (P < 0.01), and the correlation coefficient was −0.72. Temperature was negatively correlated with SO2, PM10, CO and NO2 (P < 0.05) (Fig. 4).

Correlation analysis of air pollutants and meteorological factors.
Stratified analysis of KD under O3 exposure
Stratified analysis of children ‘s sex, age, past medical history and other factors showed that sex, age and past medical history were risk factors. The age of children was associated with the risk of KD, RR was 9.27 and 12.35, 95%CI = (3.45, 14.93), (4.39,15.19). There was no correlation between the occurrence of KD and no previous history and living in rural areas (Fig. 5).

RR: relative risk.
Effect of O3 exposure on KD and exposure window
The distribution lag effect model was used to analyze the relationship between O3 and KD. Without adjusting the relevant factors, the results showed that the occurrence of KD was significantly correlated with O3 from lag 2 days to lag 5 days. On the 2th day of lag, exposure to O3 increased the risk of KD by 7.1%(RR = 1.07,95%CI = (1.001,1.15)). On the 4th day of lag, O3 led to the highest risk of KD, RR = 1.09(95%CI = 1.008,1.19) (Fig. 6).

The figure shows a correlation between short-term O3 exposure and KD. The dashed lines represent a 95% confidence interval. The crude model only included the association between O3 exposure concentration and KD in children.
Clinical indicators and KD mediation analysis
The mediating role of related clinical indicators, such as WBC, NEUT and PLT, between O3 exposure and KD was evaluated. The results showed that lymphocyte (LY), hemoglobin (HB) and fibrinogen (FIB) had direct mediating effects. Clinical indicators such as WBC, NEUT, PLT, and alanine aminotransferase (ALT) have significant direct and indirect mediating effects. In addition, these clinical indicators are considered to be risk factors for KD (Table 2).
Sensitivity analysis
In Model 1, the age, sex, allergy history and other factors of the children were adjusted as covariates, and the results remained stable. In model 2, due to the high daily average value of O3 during the Chinese New Year, we excluded O3 exposure for 40 days before and after Lunar New Year ‘s Eve, and reassessed the association between O3 and KD. The results did not change substantially.31 Model 3, a variety of pollutant models showed that the effect of O3 exposure on KD was enhanced, but the change was not significant. Model 4, excluding the participants caused by infection, the model remains stable. All sensitivity analyses confirm the robustness of our main conclusions (Table 3 and Figs. 6–10).

The figure shows a correlation between short-term O3 exposure and KD. The dashed lines represent a 95% confidence interval. Model 1 adjusted for age, sex, medical history, blood routine, and other factors based on the crude model.

The figure shows a correlation between short-term O3 exposure and KD. The dashed lines represent a 95% confidence interval. In model 2, we excluded the data of 40 days before and after New Year’s Eve and re-estimated the O3 concentration.

The figure shows a correlation between short-term O3 exposure and KD. The dashed lines represent a 95% confidence interval. In model 3, we included the multi-pollutant model for adjustment.

The figure shows a correlation between short-term O3 exposure and KD. The dashed lines represent a 95% confidence interval. In model 4, we excluded participants with infection-induced disease.
Discussion
Environmental temperature, ultraviolet radiation and humidity are the key factors affecting O3 concentration. The increase of O3 concentration will lead to an increase in the incidence of chronic diseases.32,33 A six-year study has shown that short-term O3 exposure increases the risk of death at different temperature levels.34 Related studies have shown that O3 may be a risk factor, which can induce oxidative stress, cause acute inflammatory response, and lead to systemic autoimmune response.35,36 In the acute phase of KD, the excessive production of reactive oxygen species in the body due to related incentives will destroy the balance between oxidation and anti-oxidation (reduction) reactions, thereby triggering a vicious cycle of inflammatory reactions and reactive oxygen metabolites, forming diffuse vasculitis, leading to coronary artery damage.37 A study counted the degree of coronary artery dilatation in 282 children with KD in Australia. The results showed that only 47(16.7%) had coronary artery dilatation and 19(6.8%) had coronary artery aneurysm.38Preschool children, urban residents, and increased outdoor activities may be high risk factors, which is consistent with our stratified analysis.39,40
Studies have shown that cytokine storms such as IL-6, IL-10, IFN-α, IFN-γ, IL-1β, and IL-1 activation are associated with the severity of autoimmune diseases.41,42,43 KD activates the innate immune response and increases the number of T helper cells.44 However, related animal experiments have shown that mice lacking T cells still have moderate to severe cardiac inflammation, suggesting that T cells may not be necessary in the development of KD vasculitis.45 The autopsy of several KD patients in the United States showed that the amount of IgA produced in the tissue and coronary artery wall of KD patients was higher than that of other patients. However, our research results have no relevant support.46 Regarding the mechanism of coronary artery disease in KD, platelet-derived growth factor is released into the vascular wall when endothelial cells are damaged, which may lead to changes in coronary inflammation.47 In the early stage of KD, NEUT can express inducible nitric oxide synthase(iNOs), which synthesizes vasodilator factors and leads to early coronary endothelial dysfunction in children with KD.48,49 The results of this study show that PLT and NEUT have significant direct and indirect mediating effects.
Another population-based cohort study in Taiwan found that the incidence of KD in children increased after infection with enterovirus.50 A clinical study in China showed that the increase of Fusobacterium, Shigella and Streptococcus may increase the incidence of KD. Bifidobacterium, Lactobacillus and Roseburia may help to alleviate the incidence of KD.51 The results of sensitivity analysis in this paper also showed that infection may lead to an increase in the incidence of KD, similar to our findings. Cohort studies in Japan and China showed that SO2 was significantly associated with increased KD incidence.2,30 However, another study of 3009 KD cases in seven major cities in North America observed that the effect of PM2.5 exposure on KD was not statistically significant.52 From 2013 to 2020, a cohort study in eastern China showed that there was a significant correlation between O3 exposure and KD incidence at lag 0 days, while lag 1 days and lag 2 days became statistically insignificant.53 In our study, after expanding the lag time, the results showed that O3 had different degrees of influence on KD in lag 2–5 days, and it was statistically significant.
Conclusions
In this study, we found that exposure to O3 was associated with an increased risk of KD. On the 4th day of lag, O3 led to the highest risk of KD, RR = 1.09(95%CI = 1.008,1.19). Further stratified analysis confirmed that a stronger positive correlation was observed in males, living in urban areas, and children with previous medical history. The relationship between O3 exposure and KD is mainly mediated by clinical indicators such as WBC, NEUT, PLT and CRP. Our results suggest that controlling industrial air pollutants, especially O3 emissions, may help to curb the disease burden of KD.
Importance and limitations
This study has some advantages. First of all, our professional doctors use relevant scales to diagnose and classify diseases, and regular follow-up questionnaires are conducted by specialized nurses.54 Inspection and analysis were carried out by relevant statisticians. Secondly, we used artificial intelligence technology and large data model technology to accurately expose O3 to the residential address of each participant, providing the accuracy of the air pollution exposure value of the child.14 In the sensitivity analysis, the confounding factors of infectious diseases and pathogenic microorganisms were excluded, and the date of onset was inferred through the chief complaint of the child, which increased the reliability of the results. Finally, this study shows that the relationship between O3 and KD is mainly mediated by WBC, NEUT, PLT and CRP, which is helpful for our further research.
Of course, our current research also has some limitations. First of all, our research is based on the residential address of the participants, but some participants may participate in outdoor sports, which may affect the accuracy of the results.55 Secondly, due to differences in geographical location, target population and research design, the validity or universality of our results may be another major issue. Our study did not exclude medical records during the novel coronavirus epidemic. Relevant studies have shown that the novel coronavirus may increase the incidence of KD, which may also lead to deviations in the results.56,57 Finally, this epidemiological study cannot answer the molecular mechanism of KD caused by O3 exposure, so further toxicological studies are needed to confirm our preliminary findings.
Data availability
The datasets generated and analysed during the current study are not publicly available due patient privacy but are available from the corresponding author on reasonable request.
References
Kawasaki, T. Acute febrile mucocutaneous syndrome with lymphoid involvement with specific desquamation of the fingers and toes in children]. Arerugi 16, 178–222 (1967).
Lin, Z. et al. Ambient air pollution, temperature and kawasaki disease in Shanghai, China. Chemosphere 186, 817–822 (2017).
Tanaka, N. Kawasaki disease (acute febrile infantile muco-cutaneous lymph node syndrome) in Japan; relationship with infantile periarteritis nodosa. Pathol. Microbiol. (Basel 43, 204–218 (1975).
Burns, J. C. et al. Seasonality of Kawasaki disease: a global perspective. PLoS One 8, e74529 (2013).
M. N. Y. M. K. Y. R. Y. H. J. P. i. Nationwide epidemiologic survey of Kawasaki disease in Japan, 2015–2016. 61 (2019).
Xie, L. P. et al. Epidemiologic Features of Kawasaki Disease in Shanghai From 2013 Through 2017. (2020).
Orru, H., Ebi, K. L. & Forsberg, B. The Interplay of Climate Change and Air Pollution on Health. Curr. Environ. Health Rep. 4, 504–513 (2017).
Song, J. et al. Mediating Role of TRPV1 Ion Channels in the Co-exposure to PM2.5 and Formaldehyde of Balb/c Mice Asthma Model. Sci. Rep. 7, 11926 (2017).
Kuo, N. C., Lin, C. H. & Lin, M. C. Prenatal and early life exposure to air pollution and the incidence of Kawasaki disease. Sci. Rep. 12, 3415 (2022).
Konkel, L. Up in the Air: Does Ground-Level Ozone Trigger Kawasaki Disease?. Environ. Health Perspect. 125, 064003 (2017).
McCrindle, B. W. et al. Diagnosis, Treatment, and Long-Term Management of Kawasaki Disease: A Scientific Statement for Health Professionals From the American Heart Association. Circulation 135, e927–e999 (2017).
Atolagbe, O. O., Romano, P. S., Southern, D. A., Wongtanasarasin, W. & Ghali, W. A. Coding rules for uncertain and “ruled out” diagnoses in ICD-10 and ICD-11. BMC Medical Informatics and Decision Making 21, https://doi.org/10.1186/s12911-024-02661-6 (2024).
Wei, J., Li, Z., Li, K., Dickerson, R. & Cribb, M. Full-coverage mapping and spatiotemporal variations of near-surface ozone pollution from 2013 to 2020 across China. (2021).
Wei, J. & Li, Z. ChinaHighO3: High-resolution and High-quality Ground-level MDA8 O3 Dataset for China (2000-2022). National Tibetan Plateau / Third Pole Environment Data Center. https://doi.org/10.5281/zenodo.10477125 (2023).
Janes, H., Sheppard, L. & Lumley, T. J. E. Case-crossover analyses of air pollution exposure data: referent selection strategies and their implications for bias. Epidemiology 16, 717–726 (2005).
Carracedo-Martínez, E., Taracido, M., Tobias, A. & Figueiras, S. A. J. E. H. P. Case-Crossover Analysis of Air Pollution Health Effects: A Systematic Review of Methodology and Application. Environ. Health Perspect. 118, 1173–1182 (2010).
Karr, C. et al. A Case–Crossover Study of Wintertime Ambient Air Pollution and Infant Bronchiolitis. Environ. Health Perspect. 114, 277–281 (2006).
Chen, R. et al. Association of Particulate Air Pollution With Daily Mortality: The China Air Pollution and Health Effects Study. Am. J. Epidemiol. 175, 1173–1181 (2012).
Wood, S. N. Generalized Additive Models: An Introduction With R. (Generalized Additive Models: An Introduction With R, 2017).
Oh, J. et al. Is Short-Term Exposure to PM2.5 Relevant to Childhood Kawasaki Disease?. Int J. Environ. Res Public Health 18, 924 (2021).
Digitale, J. C., Martin, J. N. & Glymour, M. M. Tutorial on directed acyclic graphs. J. Clin. Epidemiol. 142, 264–267 (2022).
Nilsson, A., Bonander, C., Strömberg, U. & Björk, J. A directed acyclic graph for interactions. Int. J. Epidemiol. 50, 613–619 (2021).
Kim, H. et al. Association between long-term PM2.5 exposure and risk of Kawasaki disease in children: A nationwide longitudinal cohort study. Environ. Res. 244, https://doi.org/10.1016/j.envres.2023.117823 (2024).
Zhao, N., Smargiassi, A., Chen, H., Widdifield, J. & Bernatsky, S. Systemic autoimmune rheumatic diseases and multiple industrial air pollutant emissions: A large general population Canadian cohort analysis. Environment Int. 174, https://doi.org/10.1016/j.envint.2023.107920 (2023).
Jung, C.-R., Chen, W.-T., Lin, Y.-T. & Hwang, B.-F. Ambient Air Pollutant Exposures and Hospitalization for Kawasaki Disease in Taiwan: A Case-Crossover Study (2000–2010). Environ. Health Perspect. 125, 670–676 (2017).
Whittle, R., Mansell, G., Jellema, P. & van der Windt, D. Applying causal mediation methods to clinical trial data: What can we learn about why our interventions (don’t) work?. Eur. J. Pain. 21, 614–622 (2017).
Wu, G., Tian, W., Zhang, L. & Yang, H. The Chinese Spring Festival Impact on Air Quality in China: A Critical Review. Int. J. Environ. Res. Pub. Health 19, https://doi.org/10.3390/ijerph19159074 (2022).
Kwon, D., Choe, Y. J., Kim, S. Y., Chun, B. C. & Choe, S. A. Ambient Air Pollution and Kawasaki Disease in Korean Children: A Study of the National Health Insurance Claim Data. J. Am. Heart Assoc. 11, e024092 (2022).
Si, F., Zhou, C., Yang, Y. J. E. S. & Research, P. Study of the relationship between occurrence of Kawasaki disease and air pollution in Chengdu by parametric and semi-parametric models. Environ. Sci. Pollut. Res Int 30, 117706–117714 (2023).
Fujii, F., Egami, N., Inoue, M. & Koga, H. J. S.oT. T. E. Weather condition, air pollutants, and epidemics as factors that potentially influence the development of Kawasaki disease. Sci. Total Environ. 741, 140469 (2020).
Xue, W., Zhan, Q., Zhang, Q., Wu, Z. J. I. J. o. E. R. & Health, P. Spatiotemporal Variations of Particulate and Gaseous Pollutants and Their Relations to Meteorological Parameters: The Case of Xiangyang, China. Int. J. Environ. Res. Pub. Health 17 https://doi.org/10.3390/ijerph17010136 (2020).
Bayram, H. A.-O. X. et al. Impact of Global Climate Change on Pulmonary Health: Susceptible and Vulnerable Populations. Ann. Am. Thorac. Soc. https://doi.org/10.1513/AnnalsATS.202212-996CME (2023).
Wang, J. et al. Particle number size distribution and new particle formation in Xiamen, the coastal city of Southeast China in wintertime. Sci. Total Environ. 826, 154208 (2022).
Chen, C., Liu, J., Shi, W., Li, T. & Shi, X. J. Temperature-Modified Acute Effects of Ozone on Human Mortality-Beijing Municipality,Tianjin Municipality,Hebei Province,and Surrounding Areas,China,2013-2018. China CDC Wkly 3, 5 (2021).
Sylvia et al. Air pollution in autoimmune rheumatic diseases: A review. Autoimmun. Rev. 11, 14–21 (2011).
Kumarathasan, P. et al. Nitrative stress, oxidative stress and plasma endothelin levels after inhalation of particulate matter and ozone. Part Fibre Toxicol. 12, 28 (2015).
Tomoyo, Y. & Kenji, H. J. R. Oxidative stress and Kawasaki disease: how is oxidative stress involved from the acute stage to the chronic stage? Rheumatology (Oxford), 56 https://doi.org/10.1093/rheumatology/kew044 (2016).
Saundankar, J. et al. The Epidemiology and Clinical Features of Kawasaki Disease in Australia. Pediatrics 133, e1009–e1014 (2014).
Nielsen, T. M., Andersen, N. H., Torp-Pedersen, C., Sgaard, P. & Kragholm, K. H. J. E. J. O. P. Kawasaki disease, autoimmune disorders, and cancer: a register-based study. Eur. J. Pediatr. 180, https://doi.org/10.1007/s00431-020-03768-4 (2021).
Zhang, M., Wang, C., Li, Q., Wang, H. & Li, X. J. I. J. o. P. Risk factors and an early predictive model for Kawasaki disease shock syndrome in Chinese children. Ital. J. Pediatr. 50, https://doi.org/10.1186/s13052-024-01597-x (2024).
Sacco, K. et al. Immunopathological signatures in multisystem inflammatory syndrome in children and pediatric COVID-19. Nat. Med 28, 1050–1062 (2022).
Hoste, L. et al. TIM3+ TRBV11-2 T cells and IFNγ signature in patrolling monocytes and CD16+ NK cells delineate MIS-C J. Exp. Med. 219, https://doi.org/10.1084/jem.20211381 (2022).
Gruber, C., Patel, R., Trachman, R., Lepow, L. & Bogunovic, D. Mapping Systemic Inflammation and Antibody Responses in Multisystem Inflammatory Syndrome in Children (MIS-C). Cell, https://doi.org/10.1016/j.cell.2023.06.012 (2020).
Tremoulet, A. H., Shimizu, C., Franco, A. & Burns, J. C. Memory T-cells and characterization of peripheral T-cell clones in acute Kawasaki disease. Autoimmunity, https://doi.org/10.3109/08916930903405891 (2013).
Noval Rivas, M. & Arditi, M. Kawasaki disease: pathophysiology and insights from mouse models. Nat. Rev. Rheumatol. 16, 391–405 (2020).
Rowley, A. H. et al. IgA Plasma Cell Infiltration of Proximal Respiratory Tract, Pancreas, Kidney, and Coronary Artery in Acute Kawasaki Disease. J. Infect. Dis. 1183, https://doi.org/10.1086/315832 (2000).
Ross, R. Atherosclerosis-an inflammatory disease. N. Engl. J. Med 340, 115 (1999).
Yu, X. et al. Enhanced iNOS expression in leukocytes and circulating endothelial cells is associated with the progression of coronary artery lesions in acute Kawasaki disease. Pediatr. Res. 55, 688–694 (2004).
Yoshida, Y. et al. Enhanced formation of neutrophil extracellular traps in Kawasaki disease. Pediatric research, https://doi.org/10.1038/s41390-019-0710-3 (2020).
Weng et al. Enterovirus Infection and Subsequent Risk of Kawasaki Disease: A Population-based Cohort Study. Pediatr. Infect Dis. J. https://doi.org/10.1097/INF.0000000000001748 (2018).
Khan, I. et al. Correlation of gut microbial compositions to the development of Kawasaki disease vasculitis in children. Future Microbiol 15, 591–600 (2020).
Zeft, A. S. et al. Kawasaki Disease and Exposure to Fine Particulate Air Pollution. J. Pediatr. 177, 179–183.e171 (2016).
Zhu, Y. et al. Short-term exposure to ozone may trigger the onset of Kawasaki disease: An individual-level, case-crossover study in East China. Chemosphere 349, https://doi.org/10.1016/j.chemosphere.2023.140828 (2024).
Ecclestone, T. & Watts, R. A. Classification and epidemiology of vasculitis: Emerging concepts. Best Pract. Res. Clin. Rheumatol. https://doi.org/10.1016/j.berh.2023.101845 (2023).
Yoo, G. Real-time information on air pollution and avoidance behavior: evidence from South Korea. Popul. Environ. 42, 406–424 (2020).
Wang, Q. & Huang, L. China’s “dynamic clearing” epidemic prevention policy: Achievements, challenges, and prospects. Front Public Health 10, 978944 (2022).
Ae, R., Shibata, Y., Kosami, K., Nakamura, Y. & Hamada, H. Kawasaki Disease and Pediatric Infectious Diseases During the Coronavirus Disease 2019 Pandemic. J. Pediatrics 239, 50–58.e52 (2021).
Acknowledgements
We are very grateful for the hard work of all clinicians and the valuable contributions of all participants in the study.
Funding
This work was supported by nicotine induces congenital heart disease by inhibiting KCTD10 expression through Notch1 signaling pathway, (project number: 3502Z20224ZD1235).
Author information
Authors and Affiliations
Contributions
SHH and ZMH proposed the study and wrote the first draft. JZW and LLZ analyzed the data. YXL, JXF and RQC collected the data. WXG, XQY and HFZ contributed to the design.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
This study was approved by the Medical Ethics Committee of Xiamen University Women’s and Children’s Hospital. Informed consent obtained from a parent and/or legal guardian under the ethical approval and consent to participate section.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
ShuHan, H., ZhiMeng, H., YaXuan, L. et al. Ozone exposure is positively correlated with the occurrence of Kawasaki disease in Chinese children. Pediatr Res (2025). https://doi.org/10.1038/s41390-025-04116-8
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41390-025-04116-8
This article is cited by
-
Ozone exposure and pediatric health: interpreting the evidence on Kawasaki disease
Pediatric Research (2025)
