
Abstract
Depression is highly prevalent among older people globally. It is well known that childhood trauma and loneliness are significant risk factors for depression, and neural alterations in the default mode network and immunological dysregulation (e.g., neutrophil-to-lymphocyte ratio) are factors significantly associated with loneliness and depression. This study examined the inter-relationships and interactions of these factors for translational insight into the pathophysiological underpinnings of late-life depression. Among ninety-two healthy older adults, we measured the leukocyte distribution as reflected by neutrophil-to-lymphocyte ratio, childhood trauma history, current feelings of loneliness, and levels of depressive symptoms. All participants underwent structural MRI scanning to acquire T1-weighted images, which were used to measure the grey matter volume within the default mode network and its key regions. We observed that loneliness as a significant mediator explained the positive relationship between childhood emotional neglect and the severity of depression in late life. The modulating effect of grey matter volume in the default mode network depends on the level of neutrophil-to-lymphocyte ratio. In sum, our findings indicated that the more severe the lonely feeling those older people with childhood emotional neglect felt, the more the depressive symptoms were, which was especially obvious among those with relatively higher neutrophil-to-lymphocyte ratio and with lower grey matter volume in the default mode network. The current findings inspire future preventive and interventional studies targeting loneliness and inflammation to promote mental wellness in older adults.
Similar content being viewed by others


Introduction
Late-life depression
Late-life depression (LLD) is a medical condition characterized by the occurrence of depression, as defined in the Diagnostic and Statistical Manual of Mental Disorders [1], among individuals aged 65 years and above [2]. It is highly prevalent in the aging population globally, with a prevalence of 29% in a population-based European sample [3], 8–16% of clinically significant depressive symptoms in the U.S. [4], and a pooled rate of 17.1% among older adults aged over 75, as reported in a meta-analysis [5]. Major depression in late life detrimentally affects individuals’ well-being by impairing social and cognitive functioning, increasing the risk of chronic diseases, disability, frailty, suicide, and mortality. It also places substantial caregiving burdens on families and society [6].
Childhood trauma and loneliness in depression
Childhood trauma and loneliness are significant risk factors for depression [7, 8]. The effect of childhood trauma is long-lasting, even in late life [9, 10]. Childhood emotional maltreatment, including abuse and neglect, shows the strongest association with depression among all types of trauma [8, 11]. Among different underlying mechanisms, it has been discovered that loneliness is one of the psychological pathways mediating the adverse effect of childhood trauma on the development of affective disorders [12, 13]. Loneliness is a subjective experience of unfulfilled social needs, even in the presence of objectively available social bonding. Its prevalence among middle-aged and older adults, especially during the COVID-19 pandemic, poses a significant public health issue [14]. Previous studies consistently demonstrated the bidirectional relationship between loneliness and depressive symptoms in middle-aged to elderly adults [7, 15,16,17]. Notably, individuals who experienced emotional maltreatment during childhood exhibit an increased vulnerability to experiencing loneliness across the lifespan, mirroring the pattern observed with depressive symptoms [18]. Therefore, individuals with a background of childhood trauma, especially emotional maltreatment, are more prone to developing depressive symptoms when experiencing profound feelings of loneliness.
The role of inflammation and the Social Signal Transduction Theory
Immunological dysregulation, including elevated inflammatory markers, weaker immune cell functioning, and changes in immune cell composition, were widely reported to be associated with perceived loneliness and depression [19,20,21,22,23]. For instance, a meta-analysis of 104 studies has found that patients with depression have a notably higher neutrophil-to-lymphocyte ratio (NLR), suggesting a potential abnormality in the dynamic interaction between the innate and adaptive cellular immune responses, when compared to healthy controls [24]. While inflammation in depression is prominent, the fuel of such long-lasting responses might be ignited since early life and stirred up throughout the life course. As postulated by the Social Signal Transduction Theory [25], early life stress contributes to the development of depression by sensitizing the immune system, provoking glucocorticoid resistance and pro-inflammatory responses, which further interfere with neuropsychological processes [26,27,28]. This theory has been supported by a recent prospective longitudinal study of over 1000 participants, in which adults with depression who had undergone severe types of early life stress (e.g., maternal rejection, harsh discipline, physical or sexual abuse) had a 1.48 times higher likelihood of having clinically elevated levels of C-reactive protein (CRP; 3 mg/L or higher) compared to individuals with depression with no such severe stressful early life experiences [29].
Default mode network, inflammation, and affective dysregulation
At the neural level, research suggests that structural and functional alterations in the default mode network (DMN), which primarily comprises brain areas of the dorsal medial prefrontal cortex, posterior cingulate cortex, precuneus, and angular gyrus, are particularly involved in the development and maintenance of loneliness and depression [30, 31]. The DMN is critical for self-referential processing and is the major neural substrate for rumination, a repetitive passive-thinking pattern that focuses on negative thoughts and distressing feelings related to past failures and perceived shortcomings, which plays a pivotal role in strengthening the link between loneliness and depression [32, 33]. Neuroimaging studies have revealed loneliness-related neural correlates, particularly concentrated in the default mode network, compared to other cortical networks [34]. Significantly, altered activation in the DMN is a well-established finding in major depressive disorder (MDD) [35, 36]. People with late-life depression experience volumetric reduction and asymmetry in DMN regions, especially in the frontal regions [37,38,39]. Overall, these findings highlight the critical involvement and unique role of the DMN in the intrinsic interaction between loneliness and depression.
Moreover, among different brain regions, the default mode network is relatively more susceptible to the effects of inflammation [40, 41] with a consistent association observed between peripheral inflammation and functional alterations in the DMN in middle-aged and older adults, and patients with depression [42]. Especially in patients with depression, the precuneus, posterior cingulate cortex (pC/pCC), and medial prefrontal cortex (mPFC) - vital nodes within the DMN - exhibit co-localization of reduced hubness and CRP-related increases in proton volume, as well as alterations in functional connectivity [43]. Functional connectivity within the DMN also exhibited a significantly negative association with levels of inflammatory markers among participants with depression [44].
In sum, previous work suggests that experiencing childhood emotional maltreatment is associated with profound feelings of loneliness and an increased vulnerability to developing depressive symptoms. Early-life stress sensitizes the immune system to a pro-inflammatory state, leading to depressive symptoms. DMN plays a critical role in the link between loneliness and depression and is highly sensitive to immune challenges. However, existing literature primarily focuses on individual relationships between pairs of concepts without an overarching interdisciplinary framework. The proposed interplay among psychosocial, immune, and neurobiological processes in depression under the Social Signal Transduction Theory of Depression [25] and the theoretical framework of the psychoneuroimmunology of mental health [45] is more intricate and complex than direct bivariate relationships can capture. Therefore, this study aims to elucidate the relationship between psychosocial factors (i.e., childhood emotional maltreatment and loneliness), immunological factors (i.e., NLR), and neural correlates (i.e., brain structure in DMN) in the development of depression. This interdisciplinary approach helps identify underlying multi-dimensional pathways that might be overlooked, outlining early detection markers and intervention targets for personalized treatments. Specifically, we hypothesized that childhood trauma, particularly emotional maltreatment, is associated with alterations in NLR, stronger feelings of loneliness, and late-life depressive symptoms. Moreover, considering the significant role of loneliness in mediating childhood trauma and depression [12, 13], we hypothesized that loneliness plays a significant mediating role in explaining the effect of childhood trauma on depressive symptoms in later life. Last but not least, we hypothesized that alterations in leukocyte distribution as reflected by NLR and grey matter (GM) volume in the DMN measured by Magnetic Resonance Imaging (MRI) modulate the association between loneliness and depressive symptoms.
Methods
Participants
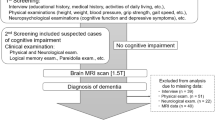
The current study is a secondary analysis under the project – “Integrating Systematic Data of Geriatric Medicine to Explore the Solution for Health Aging”, which has been registered on clinicaltrials.gov (ID: NCT04207502) [46]. The study has been approved by the Ethics Committee of the institutional review board of Chang Gung Medical Foundation of Taiwan (approval number 201900702A3). The target enrolment sample size was set at 100 participants, based on empirical and feasibility considerations. No formal statistical estimation was performed to determine the sample size. Finally, 112 healthy adult participants were recruited, including 49 men aged 60 to 92 years old. Participants who had (1) clinical evidence of major organ system abnormalities, (2) a history of severe autoimmune disorders, (3) cancer treatment at recruitment, (4) antibiotic treatment within one month of recruitment, (5) psychotropic medication use at recruitment, (6) gained a score of 2 or above in Ascertain Dementia 8, a score of 26 or less in Mini-Mental State Examination (MMSE) [47], a score of 5 or above in Geriatric Depression Scale, (7) outpatient follow-up for cognitive problems, (8) physician-diagnosed dementia or major depressive disorder, (9) significant hearing, visual, or cognitive impairments, or inability to participate in interviews in a meaningful manner were excluded from the current study. The inclusion and exclusion criteria were pre-established 48, with the addition of criteria (4) and (5) in the current study due to our primary focus. To ensure statistical validity and exclude participants with pathological conditions, we identified and excluded one participant whose Hamilton Rating Scale for Anxiety scores were over 25, which was considered a severe level of anxiety [48]. A final sample of 92 participants was included in the formal analyses. The experimental procedure adhered to the principles outlined in the Declaration of Helsinki. All participants gave their informed consent to participate in the study.
Assays and materials
Measurements of hematological markers
Blood samples were obtained from participants who had fasted for at least 8 h before the study. These samples were collected in EDTA tubes for further measurement of haematological indices with the Sysmex XE-5000 haematology analyser (Sysmex; Kobe, Japan) [49]. A complete blood count test and leukocyte distribution, including segmented neutrophils, lymphocytes, monocytes, eosinophils, and basophils, were measured in all subjects. The neutrophil-to-lymphocyte ratio was calculated by dividing the level of neutrophils by the level of lymphocytes.
Childhood Trauma Questionnaire (CTQ) – short form
The childhood trauma questionnaire is a 28-item retrospective, self-reported inventory assessing child abuse and neglect [50]. It has five clinical scales, each consisting of 5 items: physical abuse, sexual abuse, emotional abuse, physical neglect and emotional neglect. The answer was rated on a 5-point Likert-type scale based on the frequency of the experiences, with 1 indicating “never true” and 5 indicating “very often true.” A higher score indicates more frequent childhood maltreatment experiences. The 3-item Minimization/Denial scale was designed to detect the bias of minimizing and underreporting childhood maltreatment experiences [51]. Overall, this questionnaire demonstrated good reliability and validity [50].
UCLA Loneliness Scale (UCLA-LS)
Perceived loneliness was measured by the Chinese version of the UCLA-Loneliness Scale [52, 53]. It consists of 20 items on a 4-point Likert scale ranging from 1 = never to 4 = always. This scale is a sensitive measure of subjective loneliness and feelings of social isolation with high internal consistency (coefficient alpha ranging from 0.89 to 0.94) test–retest reliability (r = 0.73) [54, 55]. The Chinese version of the UCLA-LS has good internal consistency with an alpha coefficient of 0.88 [56] and test–retest reliability (r = 0.85) [57]. Higher scores indicate higher levels of perceived loneliness.
The Hamilton Rating Scale for Depression (HAM-D)
The severity of depression was measured by HAM-D [58] administered by a trained research assistant. It contains 17 items rated on a 3- or 5-point scale, with the sum of all items comprising the total score. Research showed that the cutoff scores maximizing sensitivity and specificity for mild, moderate and severe depression are 8, 17, and 24, respectively. It showed adequate reliability and validity [59]. The Chinese version of the HAM-D has been validated by Zheng et al. [60].
MRI processing
Image acquisition and pre-processing
MRI data were acquired using 8-channel head coils on 3 T MRI scanners (Discovery MR750w and Discovery MR750; GE Healthcare, Milwaukee, WI). We performed a 3D T1-weighted anatomical scan using an inversion-recovery fast spoiled gradient- echo sequence (axial 3D BRAVO [Brain Volume Imaging]; GE Healthcare) with the following parameters: repetition time (TR) = 8.58 ms, echo time (TE) = 3.23 ms, inversion time = 450 ms, flip angle = 12°, field-of-view (FOV) = 256 × 256 mm2, voxel size = 1 × 1 × 1 mm3, and number of averages = 1, and a total of 172 slices. The pre-processing was conducted using Data Processing & Analysis for Brain Imaging (DPABI) [61] and Statistical Parameter Mapping 12 (SPM12) toolboxes, including brain extraction, segmentation, normalization to Montreal Neurologic Institute (MNI) space, and smoothing (FWHM = 8 mm × 8 mm × 8 mm). After pre-processing, each participant’s grey matter volume map was extracted for subsequent analysis.
Extraction of the grey matter volume of default mode network
We followed the delineation of the default mode network as developed by Yeo et al. [62] to obtain the DMN mask. They employed a clustering approach to parcellate the cerebral cortex into seven functionally connected networks, based on data from 1000 participants. To gain a more detailed understanding of the regions within the network that play a more significant role, we identified 10 regions of interest (ROIs) using the Automated Anatomical Labeling (AAL) atlas [63] that are located within the DMN (i.e., bilateral dorsolateral superior frontal gyrus, bilateral orbital inferior frontal gyrus, etc., see Table 1 for details). Specifically, we created the individual mask for each ROI by extracting the overlapping area between the DMN mask defined by Yeo and colleagues [62] and the AAL regions using DPABI (Fig. 1). Then, we averaged the grey matter volume of all voxels within the ROI masks for statistical analysis. As five participants did not complete the MRI scanning, and two participants were excluded due to a history of stroke, a sample of 85 participants was thus included in the image processing and statistical analysis.

Overlapping regions between default mode network mask [62] and 10 identified regions of interest in the automated anatomical atlas (AAL).
Data collection procedures
Upon arriving at the research centre, participants completed questionnaires that collected their demographics (e.g., age, sex, education level, ethnicity, occupation) and medical histories (e.g., self-reported medical conditions, long-term medication intake, family medical history). Medical records were also retrieved and reviewed to confirm the self-reported medical history gathered from the interviews. Participants then completed the CTQ and UCLA-LS questionnaires following standardized instructions to ensure consistency. The HAM-D interviews were administered by a trained research assistant under the supervision of board-certified psychiatrists to maintain accuracy and reliability in scoring. To further enhance the quality control process, all assessments were double-scored to verify accuracy, and the data entry was double-checked to prevent any errors. Finally, a registered nurse performed the whole blood drawing (5 mL per person). All participants received the blood draw between 8:30 and 9:00 in the morning.
Statistical analysis
Statistical analysis was conducted using the Statistical Packages for Social Sciences (SPSS) version 23.0 [64]. We first applied a natural log transformation to CTQ, UCLA-LS, HAM-D, and levels of neutrophil and lymphocyte to correct for the skewness of the distribution. Bivariate Pearson correlation analysis (two-tailed) was used to explore the associations between NLR, loneliness, depressive symptoms, and childhood trauma. Multiple regression analysis (two-tailed) was applied to investigate the relationships between different types of childhood trauma, NLR, loneliness and depressive symptoms while controlling for age, sex, and CTQ denial. We tested the relationships and interactions between default mode network grey matter volume and NLR, childhood trauma, loneliness, and depressive symptoms in the participants who performed MRI scanning (N = 85) while controlling for age, sex, denial, and total volume. Lastly, we examined the conditional indirect effect of childhood trauma on depressive symptoms depending upon the interaction between DMN GM volume and NLR while controlling for age, sex, CTQ denial, and total volume and the conditional indirect effects driven by key ROIs within the DMN, while controlling for age, sex, CTQ denial, global average DMN GM volume, and total volume. The moderating effects and the conditional indirect effect of childhood trauma on depressive symptoms were tested by the Bootstrapping technique [65] in PROCESS macro 4.0 [66] with Model 3 and Model 18. Bootstrapping is a suitable tool for dealing with skewed or non-normally distributed data, as it does not rely on the assumption of normality and provides robust estimates through resampling. The total bootstrapping time was set at 10,000 to obtain the bias-corrected and accelerated (Bca) 95% confidence intervals (CI). The moderating effect was supported when the interaction term was significant at p < 0.05 (two-tailed), and the Bca 95% CI did not include zero. The conditional indirect effect was supported when the Bca 95% CI of the index of moderated mediation did not include zero. To control for the false discovery rate, we used the Benjamini-Hochberg procedures for multiple testing corrections in all applicable analyses.
Results
Characteristics of the participants
Ninety-two participants were included in this study. Table 2 presents the demographic information and descriptive statistics of levels of neutrophil and lymphocyte, NLR, childhood trauma, loneliness, and depressive symptoms in this sample.
Bivariate Pearson correlation analysis was conducted to investigate the relationships between neutrophil-to-lymphocyte ratio, loneliness, depressive symptoms, and childhood trauma. The uncorrected significance levels were marked with asterisks while the significant results after correction were bolded. Loneliness was significantly associated with emotional neglect (r = 0.45, p < 0.001, corrected p < 0.001), emotional abuse (r = 0.25, p = 0.02, corrected p = 0.04), and physical neglect (r = 0.44, p < 0.001, corrected p < 0.001). HAM-D was associated with emotional neglect (r = 0.30, p = 0.004, corrected p = 0.01), emotional abuse (r = 0.24, p = 0.02, corrected p = 0.05), and physical neglect (r = 0.33, p = 0.002, corrected p = 0.007). Table 3 presents the Pearson correlation between each pair of variables.
Relationships between different types of childhood trauma, neutrophil-to-lymphocyte ratio, loneliness and depressive symptoms
Multiple regression was conducted to elucidate further which types of childhood trauma were associated with neutrophil-to-lymphocyte ratio, loneliness and depressive symptoms in late life (N = 92). We controlled for age, sex and denial and applied 10,000 times bootstrapping.
First, none of the traumas or depressive symptoms was directly related to the neutrophil-to-lymphocyte ratio. Next, we included the five types of trauma as independent variables in the multiple regression model simultaneously to examine their relationship with loneliness. This approach allows us to test the unique contribution of each type of trauma in predicting the level of loneliness, while accounting for the presence and effects of other types of trauma. Only emotional neglect was a significant statistical predictor of loneliness, B = 0.189, p = 0.065, 95% Bca CI = [0.003, 0.392]. Finally, we treated the five types of trauma as independent variables simultaneously to further examine their relationship with depressive symptoms. None of them was related to depressive symptoms directly.
The role of default mode network grey matter volume
Following the behavioral findings, we have also investigated the role of DMN and its relationships with childhood trauma, neutrophil-to-lymphocyte ratio, loneliness, and depressive symptoms in the participants who performed MRI scanning (N = 85).
No significant relationship existed between neutrophil-to-lymphocyte ratio and DMN GM volume. Multiple regression analysis was conducted by simultaneously adding five types of traumas as independent variables to predict the GM volume in the DMN. Results revealed that none of the childhood trauma was associated with DMN GM volume.
We then tested the interactive effects between DMN and neutrophil-to-lymphocyte ratio on the relationship between loneliness and the severity of depression. We found a consistent pattern of significant three-way interactions between feelings of loneliness, DMN GM volume and neutrophil-to-lymphocyte ratio in relation to depressive symptoms. In specific, DMN GM volume moderated the relationship between loneliness and the severity of depression (R-squared change = 0.0665, p = 0.02, 95% bootstrapping CI = [−42.4170, −3.5483]), depending on neutrophil-to-lymphocyte ratio, while controlling for age, sex, and total volume. Only under the high neutrophil-to-lymphocyte ratio did DMN moderate the association between loneliness and depression (β = −18.6294, p = 0.01). No moderating effect was observed when the neutrophil-to-lymphocyte ratio was low (β = 15.9803, p = 0.14) or at the average level (β = −1.3245, p = 0.81). Furthermore, loneliness was positively associated with the severity of depression only when DMN GM volume was low. The neutrophil-to-lymphocyte ratio was high (β = 2.6976, 95% bootstrapping CI = [1.0207, 4.3746]), or when DMN GM volume was at the average and the neutrophil-to-lymphocyte ratio was at average (β = 0.7187, 95% bootstrapping CI = [0.0556, 1.0924]) or high (β = 1.2861, 95% bootstrapping CI = [0.2722, 2.3000]). When GM volume within DMN was large, no such association was observed, regardless of the neutrophil-to-lymphocyte ratio.
The moderated mediation model of the severity of depression
Based on the previous findings, we further conducted a moderated mediation analysis to explore the effect of childhood emotional neglect and feelings of loneliness on the severity of depression in late life and how DMN and alterations in leukocyte distribution might worsen the condition (N = 85). Results found that the indirect effect of childhood emotional neglect on late-life depressive symptoms was moderated by the interaction between neutrophil-to-lymphocyte ratio and DMN GM volume (95% CI of the index of moderated mediation = [−12.9811, −0.0335], Fig. 2). Specifically, loneliness positively mediated the association between childhood emotional neglect and the severity of depression only when DMN GM volume was low but the neutrophil-to-lymphocyte ratio was high (β = 0.5536, bootstrapping CI = [0.0559, 1.4165]). However, the indirect effect was nonsignificant when DMN GM volume was at the average or high level, regardless of the neutrophil-to-lymphocyte ratio, while controlling for age, sex, CTQ denial and total volume. No significant direct effect was detected (β = 0.3646, bootstrapping CI = [−0.2377, 0.9669]). In other words, childhood emotional neglect was associated with stronger feelings of loneliness and severe depression in late life only when the DMN GM volume was low, especially in individuals with higher neutrophil-to-lymphocyte ratios. However, in individuals without any changes in leukocyte distribution, childhood emotional neglect would not be indirectly related to the severity of depression unaffected by DMN grey matter volume (Fig. 2).

The conditional indirect effect of childhood emotional neglect on the severity of depression via loneliness depends on the interaction between default mode network grey matter volume and neutrophil-to-lymphocyte ratio (N = 85). Note. *p < 0.05 (2-tailed).
We conducted moderated mediation analysis with the above model to identify the key ROIs within DMN that play prominent roles in driving this relationship. We controlled for age, sex, overall DMN grey matter volume, and total volume. It was found that the neutrophil-to-lymphocyte ratio moderated the interaction between bilateral dorsolateral part of superior frontal gyrus, bilateral orbital part of inferior frontal gyrus, bilateral anterior cingulate and paracingulate gyri, and bilateral angular gyrus and loneliness in relation to the severity of depression. Nonetheless, these results did not survive the correction for multiple comparisons (Table 4). After bootstrapping, bilateral angular gyrus positively moderated the indirect effect of childhood emotional neglect on the severity of depression via feelings of loneliness when the neutrophil-to-lymphocyte ratio was low (β = 16.2794, p = 0.02) but negatively moderated this association when the neutrophil-to-lymphocyte ratio was high (β = −5.8790, p = 0.04). As a result, childhood emotional neglect was negatively associated with the severity of depression in late life when angular gyrus GM volume and neutrophil-to-lymphocyte ratio were both low (β = −0.7212, 95% CI = [−1.6485, −0.0088]) but positively associated with the severity of depression in late life when angular gyrus GM volume was high but neutrophil-to-lymphocyte ratio was low (β = 0.7989, 95% CI = [0.0686, 1.6050]). However, this result did not survive after correction for multiple comparisons (Table 4).
Discussion
Our findings highlight that the adverse impact of childhood emotional neglect on the severity of late-life depression can be explained by loneliness, particularly in individuals with lower grey matter volume within the default mode network and higher neutrophil-to-lymphocyte ratio. Our finding supports the Social Signal Transduction Theory [25], which proposed that social-environmental stress sensitizes the immune system and disturbs neuropsychological processes, explaining the pathogenesis of depression. Our findings provide new evidence to support this theory, revealing that altered leukocyte distribution, as indicated by a higher neutrophil-to-lymphocyte ratio, exacerbates the relationship between loneliness and depression severity by interacting with a crucial brain network – the default mode network.
We found emotional neglect and abuse and physical neglect were associated with loneliness and depression in bivariate correlation after correction, and only emotional neglect remained statistically significant in the regression model after bootstrapping. This finding is consistent with prior meta-analysis results and empirical findings suggesting that individuals with the experience of childhood emotional maltreatment tend to experience higher levels of loneliness [18, 67]. Childhood emotional neglect interferes with neuro-affective processing and is further associated with specific neural patterns, including reduced reward-related ventral striatum activation [68], heightened activity in the left amygdala and hippocampus when facing threatening stimuli [69], and impaired emotional clarity – defined as the ability to recognize and understand one’s emotions [70].
We did not detect any significant direct associations between neutrophil-to-lymphocyte ratio and childhood trauma, loneliness or depression, opposite to the previous observations on the positive relationship between inflammation (i.e., increases in CRP or white blood cell count), childhood maltreatment and loneliness and depression [71,72,73]. A possible explanation for the nonsignificant association between immune indices and negative psychological symptoms or adverse experiences in this sample was the ‘floor effect’ due to the high overall health status of the participants. Previous research has observed elevated inflammatory markers in patients suffering from MDD compared to healthy controls [74], as well as a significant association between CRP levels and the severity of depression in patients with MDD [75], but no direct association in participants showing depressive symptoms without diagnoses [76, 77]. At the neural level, we did not detect significant correlations between NLR and changes in DMN GM volume. The possible explanations for the discrepancies in results are that, compared to CRP, a widely clinically used marker of inflammation, leukocyte distribution is affected by more physiological factors, being more dynamic and fluctuating [78]. Moreover, the older adults in our sample are generally healthy, which may have produced a floor effect, making it challenging to detect the effects.
To the best of our knowledge, no other paper has explored the complex interaction between early life stress, loneliness and depressive symptoms from the perspective of psychoneuroimmunology by integrating both neural and immunological data. Our finding supports the a priori hypothesis that childhood emotional neglect is indirectly positively associated with the severity of depression, fully explained by feelings of loneliness. Remarkably, we found that the interaction between the neutrophil-to-lymphocyte ratio and GM volume within the DMN modulates the association between loneliness and depressive symptoms. The co-presence of low DMN GM volume and high neutrophil-to-lymphocyte ratio exacerbates the effect of childhood emotional neglect on loneliness and the severity of depression. In contrast, when the volume of GM in the DMN is high, there is no such relationship, even if the neutrophil-to-lymphocyte ratio is high, suggesting that preserving a higher DMN GM volume might be a compelling protective factor mitigating the strong association between loneliness and affective symptoms, particularly among healthy older adults. Studies have demonstrated that the volume of GM is indicative of alterations in physical tissue volume at the cellular level and is also linked to nuclear volume, the number of local cells, and the characteristics of spatial cell clustering [79]. These indices are essential biological bases for its functional integration. Overall, our discoveries provide a more profound understanding of the existing knowledge that loneliness mediates the association between childhood maltreatment and adult depression [13, 80], highlighting that DMN structural changes and alteration in leukocyte distribution worsen the circumstances.
In further exploration of this phenomenon, we have conducted a detailed investigation of the key regions of the DMN. We found that the bilateral dorsolateral part of the superior frontal gyrus, the orbital inferior part of the frontal gyrus, the anterior cingulate and paracingulate gyri, and the angular gyrus were critical regions driving the modulating effects of the DMN. Notably, abnormal structural and functional changes in these above-mentioned regions have been widely recognized as the underlying pathophysiology of depression [81]. They are also reported to be vulnerable to the effect of inflammation, exhibiting inflammation-associated cortical thinning [82]. Therefore, the interconnection between feelings of loneliness and depression is closely tied to atrophy in those regions under the attack of inflammation.
This study has both theoretical and translational implications. It supports the Social Signal Transduction Theory by showing that early-life and interpersonal stress interact with the sensitized immune system and neural networks to contribute to depressive symptoms. The current findings underscore the need for tailored psychological and medical support for at-risk older adults with a systemic pro-inflammatory status who are particularly vulnerable to current and past emotional stress. Furthermore, our findings suggest that the enriched brain tissues within the DMN buffer against the self-reinforcing loop between loneliness and depressive symptoms, highlighting the necessity of protecting brain health, especially targeting the DMN, for promoting mental well-being in late life.
Despite the promising findings, several limitations must be acknowledged. First, we should exercise caution when inferring causality due to the cross-sectional nature of this study. However, we can reasonably interpret the results by considering the temporal order between the variables, suggesting that early-life stress may primarily impact late-life mental wellness through current feelings of loneliness and current inflammation status. Meanwhile, a relatively small sample size, due to feasibility constraints, also limits the statistical power, which can be verified by replicating the study in larger samples. Second, it can be challenging to assess childhood trauma history in older individuals; thus the results should be interpreted with caution. Given the considerable time interval between the participants’ childhood and the time of the present study, memory decay and retrospective bias might hinder the accurate recall of personal experience. Meanwhile, social desirability, stigma, and cultural differences may potentially impact the accuracy of the reports [83]. Asian samples report lower CTQ estimates compared to the worldwide average [84], but this might be due to a lower willingness to self-disclose in a collectivist culture than in individualistic cultures [85]. Nevertheless, 12 and 13% of the participants in this sample experienced low-to-moderate levels of childhood emotional and physical neglect, respectively, reflecting a common feature of this sample despite the influence of the above factors. Third, our study only measured structural changes within the DMN, which limits our ability to generalize the interpretations to neural functional changes. However, volumetric characteristics are more stable in revealing the long-lasting accumulative effect of inflammatory and immune responses on the brain, providing additional information beyond other functional connectivity approaches. Future multimodal neuroimaging studies examining both volumetric and functional changes in various brain networks may unravel more detailed effects of inflammation on neuro-affective processing.
In conclusion, our research offers sophisticated insights into the psychoneuroimmunological mechanisms entangling childhood trauma, loneliness, and depressive symptoms in older adults. Our findings demonstrate that loneliness mediates the association between childhood emotional neglect and the severity of depression modulated by default mode network grey matter volume and the neutrophil-to-lymphocyte ratio in late life, enriching the Social Signal Transduction Theory. These results underscore the importance of alleviating perceived loneliness, enhancing robust immune functioning, and maintaining brain health to mitigate depressive symptoms in the older population, especially among those with a history of childhood emotional neglect. The insights gained in this study pointed out the critical directions for designing early prevention and timely intervention to ameliorate depressive symptoms and promote mental wellness in the aging population.
Data availability
The data are part of the project “Integrating Systematic Data of Geriatric Medicine to Explore Solutions for Healthy Aging”. The data are not publicly available due to privacy and ethical restrictions. Deidentified data related to the findings of this study are available upon request from the corresponding authors.
References
American Psychiatric Association (5th ed.) Diagnostic and statistical manual of mental disorders: DSM-5. (Washington, DC, American Psychiatric Publishing, 2013).
Alexopoulos GS. Depression in the elderly. Lancet. 2005;365:1961–70.
Horackova K, Kopecek M, Machů V, Kagstrom A, Aarsland D, Motlova LB, et al. Prevalence of late-life depression and gap in mental health service use across European regions. Eur Psychiatry. 2019;57:19–25.
Blazer DG. Depression in late life: review and commentary. J Gerontol A Biol Sci Med Sci. 2003;58:M249–M265.
Luppa M, Sikorski C, Luck T, Ehreke L, Konnopka A, Wiese B, et al. Age- and gender-specific prevalence of depression in latest-life-systematic review and meta-analysis. J Affect Disord. 2012;136:212–21. https://doi.org/10.1016/j.jad.2010.11.033.
Patten SB. Long-term medical conditions and major depression in a Canadian population study at waves 1 and 2. J Affect Disord. 2001;63:35–41.
Cacioppo JT, Hughes ME, Waite LJ, Hawkley LC, Thisted RA. Loneliness as a specific risk factor for the severity of depression: cross-sectional and longitudinal analyses. Psychol Aging. 2006;21:140.
Mandelli L, Petrelli C, Serretti A. The role of specific early trauma in adult depression: a meta-analysis of published literature. Childhood trauma and adult depression. Eur Psychiatry. 2015;30:665–80.
Comijs HC, Van Exel E, van der Mast RC, Paauw A, Voshaar RO, Stek ML. Childhood abuse in late-life depression. J Affect Disord. 2013;147:241–6.
Wielaard I, Hoyer M, Rhebergen D, Stek ML, Comijs HC. Childhood abuse and late‐life depression: mediating effects of psychosocial factors for early‐and late‐onset depression. Int J Geriatr Psychiatry. 2018;33:537–45.
Humphreys KL, LeMoult J, Wear JG, Piersiak HA, Lee A, Gotlib IH. Child maltreatment and depression: a meta-analysis of studies using the Childhood Trauma Questionnaire. Child Abuse Negl. 2020;102:104361. https://doi.org/10.1016/j.chiabu.2020.104361.
Fan L, Chen Y, Zhu M, Mao Z, Li N. Correlation between childhood trauma experience and depressive symptoms among young adults: the potential mediating role of loneliness. Child Abuse Negl. 2023;144:106358.
Shevlin M, McElroy E, Murphy J. Loneliness mediates the relationship between childhood trauma and adult psychopathology: evidence from the adult psychiatric morbidity survey. Soc Psychiatry Psychiatr Epidemiol. 2015;50:591–601.
Surkalim DL, Luo M, Eres R, Gebel K, van Buskirk J, Bauman A, et al. The prevalence of loneliness across 113 countries: systematic review and meta-analysis. BMJ. 2022;376:e067068.
Lee SL, Pearce E, Ajnakina O, Johnson S, Lewis G, Mann F, et al. The association between loneliness and the severity of depression among adults aged 50 years and older: a 12-year population-based cohort study. Lancet Psychiatry. 2021;8:48–57.
McHugh Power J, Hannigan C, Hyland P, Brennan S, Kee F, Lawlor BA. The severity of depression predict increased social and emotional loneliness in older adults. Aging Ment Health. 2020;24:110–8.
Steiner JF, Ross C, Stiefel M, Mosen D, Banegas MP, Wall AE, et al. Association between changes in loneliness identified through screening and changes in depression or anxiety in older adults. J Am Geriatr Soc. 2022;70:3458–68.
de Heer C, Bi S, Finkenauer C, Alink L, Maes M. The association between child maltreatment and loneliness across the lifespan: a systematic review and multilevel meta-analysis. Child Maltreat. 2024;29:388–404. https://doi.org/10.1177/10775595221103420.
Balter LJT, Hulsken S, Aldred S, Drayson MT, Higgs S, Veldhuijzen van Zanten JJC, et al. Low-grade inflammation decreases emotion recognition - evidence from the vaccination model of inflammation. Brain Behav Immun. 2018;73:216–21.
Bhikram T, Sandor P. Neutrophil-lymphocyte ratios as inflammatory biomarkers in psychiatric patients. Brain Behav Immun. 2022;105:237–46.
Brinn A, Stone J. Neutrophil-lymphocyte ratio across psychiatric diagnoses: a cross-sectional study using electronic health records. BMJ open. 2020;10:e036859.
Hawkley LC, Cacioppo JT. Loneliness matters: a theoretical and empirical review of consequences and mechanisms. Ann Behav Med. 2010;40:218–27.
Singh D, Guest PC, Dobrowolny H, Vasilevska V, Meyer-Lotz G, Bernstein HG, et al. Changes in leukocytes and CRP in different stages of major depression. J Neuroinflammation. 2022;19:74.
Sørensen NV, Frandsen BH, Orlovska-Waast S, Buus TB, Ødum N, Christensen RH, et al. Immune cell composition in unipolar depression: a comprehensive systematic review and meta-analysis. Mol Psychiatry. 2023;28:391–401.
Slavich GM, Irwin MR. From stress to inflammation and major depressive disorder: a social signal transduction theory of depression. Psychol Bull. 2014;140:774–815. https://doi.org/10.1037/a0035302.
Carpenter LL, Gawuga CE, Tyrka AR, Lee JK, Anderson GM, Price LH. Association between plasma IL-6 response to acute stress and early-life adversity in healthy adults. Neuropsychopharmacology. 2010;35:2617–23.
Fagundes CP, Glaser R, Kiecolt-Glaser JK. Stressful early life experiences and immune dysregulation across the lifespan. Brain Behav Immun. 2013;27:8–12.
Irwin MR, Cole SW. Reciprocal regulation of the neural and innate immune systems. Nat Rev Immunol. 2011;11:625–32.
Danese A, Moffitt TE, Pariante CM, Ambler A, Poulton R, Caspi A. Elevated inflammation levels in depressed adults with a history of childhood maltreatment. Arch Gen Psychiatry. 2008;65:409–15.
Cacioppo JT, Fowler JH, Christakis NA. Alone in the crowd: the structure and spread of loneliness in a large social network. J Pers Soc Psychol. 2009;97:977–91.
Sheline YI, Barch DM, Price JL, Rundle MM, Vaishnavi SN, Snyder AZ, et al. The default mode network and self-referential processes in depression. Proc Natl Acad Sci USA. 2009;106:1942–7.
Nolen-Hoeksema S, Wisco BE, Lyubomirsky S. Rethinking rumination. Perspect Psychol Sci. 2008;3:400–24.
Zhou HX, Chen X, Shen YQ, Li L, Chen NX, Zhu ZC, et al. Rumination and the default mode network: meta-analysis of brain imaging studies and implications for depression. NeuroImage. 2020;206:116287.
Spreng RN, Dimas E, Mwilambwe-Tshilobo L, Dagher A, Koellinger P, Nave G, et al. The default network of the human brain is associated with perceived social isolation. Nat Commun. 2020;11:6393. https://doi.org/10.1038/s41467-020-20039-w.
Mulders PC, van Eijndhoven PF, Schene AH, Beckmann CF, Tendolkar I. Resting-state functional connectivity in major depressive disorder: a review. Neurosci Biobehav Rev. 2015;56:330–44.
Sun S, Yan C, Qu S, Luo G, Liu X, Tian F, et al. Resting-state dynamic functional connectivity in major depressive disorder: a systematic review. Prog Neuropsychopharmacol Biol Psychiatry. 2024;135:111076.
Kumar A, Bilker W, Jin Z, Udupa J. Atrophy and high intensity lesions: complementary neurobiological mechanisms in late-life major depression. Neuropsychopharmacology. 2000;22:264–74.
Kumar A, Bilker W, Lavretsky H, Gottlieb G. Volumetric asymmetries in late-onset mood disorders: an attenuation of frontal asymmetry with depression severity. Psychiatry Res. 2000;100:41–47.
Shao R, Gao M, Lin C, Huang CM, Liu HL, Toh CH, et al. Multimodal neural evidence on the corticostriatal underpinning of suicidality in late-life depression. Biol Psychiatry Cogn Neurosci Neuroimaging. 2022;7:905–15. https://doi.org/10.1016/j.bpsc.2021.11.011.
Bradley KA, Stern ER, Alonso CM, Xie H, Kim-Schulze S, Gabbay V. Relationships between neural activation during a reward task and peripheral cytokine levels in youth with diverse psychiatric symptoms. Brain Behav Immun. 2019;80:374–83.
Walker KA, Gross AL, Moghekar AR, Soldan A, Pettigrew C, Hou X, et al. Association of peripheral inflammatory markers with connectivity in large-scale functional brain networks of non-demented older adults. Brain Behav Immun. 2020;87:388–96.
Kraynak TE, Marsland AL, Wager TD, Gianaros PJ. Functional neuroanatomy of peripheral inflammatory physiology: a meta-analysis of human neuroimaging studies. Neurosci Biobehav Rev. 2018;94:76–92.
Kitzbichler MG, Aruldass AR, Barker GJ, Wood TC, Dowell NG, Hurley SA, et al. Peripheral inflammation is associated with micro-structural and functional connectivity changes in depression-related brain networks. Mol psychiatry. 2021;26:7346–54.
Aruldass AR, Kitzbichler MG, Morgan SE, Lim S, Lynall ME, Turner L, et al. Dysconnectivity of a brain functional network associated with blood inflammatory markers in depression. Brain Behav Immun. 2021;98:299–309.
Slavich GM Psychoneuroimmunology of stress and mental health. in The Oxford handbook of stress and mental health (eds Harkness KL & Hayden EP). Oxford University Press; 2020. p. 519-45.
Siow TY, Toh CH, Hsu JL, Liu GH, Lee SH, Chen NH, et al. Association of sleep, neuropsychological performance, and gray matter volume with glymphatic function in community-dwelling older adults. Neurology. 2022;98:e829–e838.
Folstein MF, Folstein SE, McHugh PR. “Mini-mental state”: a practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. 1975;12:189–98.
Rabinowitz J, Williams JBW, Hefting N, Anderson A, Brown B, Fu DJ, et al. Consistency checks to improve measurement with the Hamilton Rating Scale for Anxiety (HAM-A). J Affect Disord. 2023;325:429–36. https://doi.org/10.1016/j.jad.2023.01.029.
Furundarena JR, Sainz M, Uranga A, Cuevas L, Lopez I, Zubicaray J, et al. Comparison of abnormal cell flagging of the hematology analyzers Sysmex XN and Sysmex XE-5000 in oncohematologic patients. Int J Lab Hematol. 2017;39:58–67. https://doi.org/10.1111/ijlh.12575.
Bernstein DP, Fink L, Handelsman L, Foote J, Lovejoy M, Wenzel K, et al. Initial reliability and validity of a new retrospective measure of child abuse and neglect. Am J Psychiatry. 1994;151:1132–6.
Bernstein DP, Fink L. Childhood trauma questionnaire: a retrospective self-report manual. San Antonio, TX: The Psychological Corporation; 1998.
Chou KL, Jun LW, Chi I. Assessing Chinese older adults’ suicidal ideation: chinese version of the geriatric suicide ideation scale. Aging Ment Health. 2005;9:167–71.
Russell DW. UCLA loneliness Scale (Version 3): reliability, validity, and factor structure. J Pers Assess. 1996;66:20–40.
Cacioppo JT, Hawkley LC, Thisted RA. Perceived social isolation makes me sad: 5-year cross-lagged analyses of loneliness and depressive symptomatology in the Chicago Health, Aging, and Social Relations Study. Psychol Aging. 2010;25:453.
Hawkley LC, Thisted RA, Cacioppo JT. Loneliness predicts reduced physical activity: cross-sectional & longitudinal analyses. Health Psychol. 2009;28:354.
Wu ZQ, Sun L, Sun YH, Zhang XJ, Tao FB, Cui GH. Correlation between loneliness and social relationship among empty nest elderly in Anhui rural area, China. Aging Ment Health. 2010;14:108–12.
Chen LJ, Chung SK. Loneliness, social connectedness, and family income among undergraduate females and males in Taiwan. Soc Behav Pers. 2007;35:1353–64.
Hamilton M. A rating scale for depression. J Neurol Neurosurg Psychiatry. 1960;23:56.
Bagby RM, Ryder AG, Schuller DR, Marshall MB. The hamilton depression rating scale: has the gold standard become a lead weight? Am J Psychiatry. 2004;161:2163–77.
Zheng Y, Zhao J, Phillips M, Liu J, Cai M, Sun S, et al. Validity and reliability of the Chinese Hamilton depression rating scale. Br J Psychiatry. 1988;152:660–4.
Yan CG, Wang XD, Zuo XN, Zang YF. DPABI: data processing & analysis for (Resting-State) brain imaging. Neuroinformatics. 2016;14:339–51.
Yeo BT, Krienen FM, Sepulcre J, Sabuncu MR, Lashkari D, Hollinshead M, et al. The organization of the human cerebral cortex estimated by intrinsic functional connectivity. J Neurophysiol. 2011;106:1125–65.
Tzourio-Mazoyer N, Landeau B, Papathanassiou D, Crivello F, Etard O, Delcroix N, et al. Automated anatomical labeling of activations in SPM using a macroscopic anatomical parcellation of the MNI MRI single-subject brain. Neuroimage. 2002;15:273–89.
IBM Corp. Released 2020. IBM SPSS statistics for windows, version 27.0. Armonk, NY: IBM Corp.
Shrout PE, Bolger N. Mediation in experimental and nonexperimental studies: new procedures and recommendations. Psychol Methods. 2002;7:422.
Hayes AF, Rockwood NJ. Regression-based statistical mediation and moderation analysis in clinical research: observations, recommendations, and implementation. Behav Res Ther. 2017;98:39–57.
Reinhard MA, Rek SV, Nenov-Matt T, Barton BB, Dewald-Kaufmann J, Merz K, et al. Association of loneliness and social network size in adulthood with childhood maltreatment: analyses of a population-based and a clinical sample. Eur Psychiatry. 2022;65:e55.
Hanson JL, Hariri AR, Williamson DE. Blunted ventral striatum development in adolescence reflects emotional neglect and predicts depressive symptoms. Biol Psychiatry. 2015;78:598–605.
Maheu FS, Dozier M, Guyer AE, Mandell D, Peloso E, Poeth K, et al. A preliminary study of medial temporal lobe function in youths with a history of caregiver deprivation and emotional neglect. Cogn Affect Behav Neurosci. 2010;10:34–49.
Jessar AJ, Hamilton JL, Flynn M, Abramson LY, Alloy LB. Emotional clarity as a mechanism linking emotional neglect and depressive symptoms during early adolescence. J Early Adolesc. 2017;37:414–32.
Danese A, Pariante CM, Caspi A, Taylor A, Poulton R. Childhood maltreatment predicts adult inflammation in a life-course study. Proc Natl Acad Sci USA. 2007;104:1319–24.
Yuan B, Li W, Liu H, Cai X, Song S, Zhao J, et al. Correlation between immune response and self-reported depression during convalescence from COVID-19. Brain Behav Immun. 2020;88:39–43.
Sun W, Miao J, Song Y, Wang Y, Pan C, Li G, et al. Systemic low-grade inflammation and depressive symptomology at chronic phase of ischemic stroke: the chain mediating role of fibrinogen and neutrophil counts. Brain Behav Immun. 2022;100:332–41.
Osimo EF, Baxter LJ, Lewis G, Jones PB, Khandaker GM. Prevalence of low-grade inflammation in depression: a systematic review and meta-analysis of CRP levels. Psychol Med. 2019;49:1958–70.
Köhler-Forsberg O, Buttenschøn HN, Tansey KE, Maier W, Hauser J, Dernovsek MZ, et al. Association between C-reactive protein (CRP) with depression symptom severity and specific depressive symptoms in major depression. Brain Behav Immun. 2017;62:344–50.
Steptoe A, Kunz-Ebrecht SR, Owen N. Lack of association between depressive symptoms and markers of immune and vascular inflammation in middle-aged men and women. Psychol Med. 2003;33:667–74.
Zalli A, Jovanova O, Hoogendijk WJG, Tiemeier H, Carvalho LA. Low-grade inflammation predicts persistence of depressive symptoms. Psychopharmacology. 2016;233:1669–78.
Bali R, Sharma P, Ghanghas P, Gupta N, Tiwari JD, Singh A, et al. To compare the efficacy of C-reactive protein and total leucocyte count as markers for monitoring the course of odontogenic space infections. J Maxillofac Oral Surg. 2017;16:322–7.
Asan L, Falfán-Melgoza C, Beretta CA, Sack M, Zheng L, Weber-Fahr W, et al. Cellular correlates of gray matter volume changes in magnetic resonance morphometry identified by two-photon microscopy. Sci Rep. 2021;11:4234.
Wielaard I, Comijs HC, Stek ML, Rhebergen D. Childhood abuse and the two-year course of late-life depression. Am J Geriatr Psychiatry. 2017;25:633–43.
Frodl T, Scheuerecker J, Albrecht J, Kleemann AM, Müller-Schunk S, Koutsouleris N, et al. Neuronal correlates of emotional processing in patients with major depression. World J Biol Psychiatry. 2009;10:202–8.
Han KM, Ham BJ. How inflammation affects the brain in depression: a review of functional and structural MRI studies. J Clin Neurol. 2021;17:503–15.
DeVylder JE, Hilimire MR. Screening for psychotic experiences: social desirability biases in a non‐clinical sample. Early Interv Psychiatry. 2015;9:331–4.
Viola TW, Salum GA, Kluwe-Schiavon B, Sanvicente-Vieira B, Levandowski ML, Grassi-Oliveira R. The influence of geographical and economic factors in estimates of childhood abuse and neglect using the Childhood Trauma Questionnaire: a worldwide meta-regression analysis. Child Abuse Negl. 2016;51:1–11.
Stoltenborgh M, Van Ijzendoorn MH, Euser EM, Bakermans-Kranenburg MJ. A global perspective on child sexual abuse: meta-analysis of prevalence around the world. Child Maltreat. 2011;16:79–101.
Acknowledgements
The authors acknowledge the data collection, data management, and information technology services, based on the Structured Research and Medical Informatics Cloud (SRMIC) platform system, provided by the Clinical Trial Center, Chang Gung Memorial Hospital, Linkou, Taiwan, with support by the Ministry of Health and Welfare under Grant No. MOHW110-TDU-B-212-124005. We thank the Genomic and Proteomic Core Laboratory of Chang Gung Memorial Hospital for the assistance of experiment conduction.
Funding
This study was supported by grant CORPG3J0371 from Chang Gung Memorial Hospital, The University of Hong Kong May Endowed Professorship, and the Hong Kong Research Grants Council General Research Fund (Ref: 17600522).
Author information
Authors and Affiliations
Contributions
RRJ: Conceptualization, Methodology, Software, Formal analysis, Investigation, Visualization, Writing - Original Draft; NMLW: Conceptualization, Methodology, Writing - Review & Editing; JJM: Methodology, Software, Writing - Review & Editing; J-TF: Investigation, Data Curation; C-ML: Investigation, Data Curation; CHT: Investigation, Data Curation; K-YW: Investigation, Data Curation; JLH: Investigation, Data Curation; C-MH: Investigation, Data Curation; SHL: Conceptualization, Investigation, Resources, Data Curation, Supervision, Project administration, Writing - Review & Editing; TMCL: Conceptualization, Investigation, Resources, Supervision, Funding acquisition, Writing - Review & Editing.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
All methods were performed in accordance with the relevant guidelines and regulations. The study has been approved by the Ethics Committee of the institutional review board of Chang Gung Medical Foundation of Taiwan (approval number 201900702A3). Informed consent was obtained from all participants.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Jin, R.R., Wong, N.M.L., Ma, J. et al. A psychoneuroimmunological underpinnings of the relationship between childhood trauma, loneliness, and depression in older adults. Transl Psychiatry 15, 328 (2025). https://doi.org/10.1038/s41398-025-03547-5
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41398-025-03547-5
