
Abstract
Given the heterogeneity of acute myeloid leukemia patients, it is necessary to identify patients considered fit for intensive therapy but who will perform poorly, and in whom alternative approaches deserve investigation. We analyzed 1034 fit adults ≤70 years intensively treated between 2012 and 2022 in the CETLAM group. Young adults ( ≤ 60 years) presented higher remission rates and improved survival than older adults above that age (CR 79% vs. 73%; p = 0.03 and 4-yr OS 53% vs. 33%; p < 0.001). Remission and survival outcomes varied among different genetic subsets. An especially adverse genetic group included complex, monosomal karyotype, TP53 alterations (deleted/mutated), and MECOMr. Transplant feasibility in this very adverse risk group was low, and OS and EFS at 4 years were 14% and 12%, in contrast to 70% and 57% in the favorable group and 38% and 32% in all other patients. We integrated clinical and genetic data into the Intensive Chemotherapy Score for AML (ICSA) with 6-risk categories with significantly different remission rates and OS, validated in another cohort of 581 AML patients from a previous CETLAM protocol. In summary, we identified groups of fit patients that benefit differently from an intensive approach which may be helpful in future treatment decisions.
Similar content being viewed by others

Introduction
Acute myeloid leukemia (AML) is clinically and genetically heterogeneous, and the prognosis is variable. Leukemia progression or relapse is the major drawback for long-term survival. Median age at diagnosis of AML is 64–67 years [1, 2]. Older AML patients frequently present with the higher number of comorbidities, adverse genetic lesions, and worse response to treatment [3,4,5].
The treatment approach varies according to the patient’s fitness to tolerate the toxicities of intensive chemotherapy (CT) regimens and allogeneic stem cell transplant (alloHCT) [6,7,8]. Age per se is not a criterion of unfitness [9,10,11]. The advent of venetoclax plus hypomethylating (HMA) combination has improved the survival of patients not candidates for CT [12, 13]. The remarkable proportion of complete remissions (CR) achieved and, in a proportion of patients, the subsequent feasibility of alloHCT is challenging the indication of front-line intensive CT even in fit older adults ( > 55–60 years old) [14,15,16,17]. In this regard, prospective randomized trials comparing CT vs. venetoclax-azacitidine are ongoing (#NCT04801797, #NCT03573024). Awaiting these results, it is of interest to investigate the factors that impact the outcome of patients that were considered fit for CT to identify those with good survival perspectives and others that are poor candidates in which less intensive and novel approaches may be justified.
The present work reflects the outcome of intensive therapy in more than 1000 AML patients uniformly treated and gives information on the feasibility of the treatment plan in a multicenter experience.
Methods
Patients with newly diagnosed AML aged 18 to 70 who were fit for intensive CT were consecutively enrolled into the AML-12 protocol, a prospective post-approval study of the Spanish CETLAM group fully described in the supplementary file and available at www.clinicaltrials.gov (NCT04687098).
Ethics approval and consent to participate
The present study was reviewed and approved by the ethics committee of the Hospital de la Santa Creu i Sant Pau (Comité ètic d’Investigació Clínica, registration number 11/2012). All methods were performed in accordance with the relevant guidelines and regulations. Informed consent for both bone marrow analysis and treatment was obtained in all cases according to the Declaration of Helsinki.
Treatment description
Induction CT included idarubicin 12 mg/m2 IV, days 1,2,3 and cytarabine 200 mg/m2 days 1 to 7. Since 2017, 45% of patients with FLT3 mutation also received midostaurin as in the RATIFY trial [18]. A second induction was administered in patients not in CR after the first CT course who showed chemo-sensitivity. Patients with less than 50% blast reduction after first induction or without a CR after two induction courses were considered refractory. Death during induction was the event when occurred regardless of the bone marrow status. If CR was achieved, the patient received consolidation therapy with high-dose cytarabine at (HDAC) 3 g/m2/12 h IV, days 1,3,5 [19]. Genetic risk was established throughout the protocol according to the European LeukemiaNet (ELN) 2010, and 2017 criteria [20, 21]. Since 2013, we included NPM1mutation with a low FLT3-ITD allelic ratio ( < 0.5; FLT3low) into the favorable category [22, 23]. In the current report, patients have been retrospectively classified according to the ELN-2022 risk stratification, with the limitation that until 2017 Next Generation Sequencing was not available routinely, and several patients from this series who are allocated to the intermediate risk category lacked studies on dysplasia-related mutations, and TP53 mutations. In patients with favorable genetics, after the first consolidation (Cons-1) two additional HDAC courses were planned, and alloHCT in first complete remission (CR1) was avoided unless MRD persisted or reappeared. In the remaining patients, the intention was alloHCT in CR1 after Cons-1, with a second consolidation allowed when required due to transplantation delay.
Laboratory testing
Diagnostic tests were performed on bone marrow (BM) samples. Centralized molecular characterization included polymerase chain reaction studies of mutations needed to classify the leukemia into risk groups, as described in the supplementary material. Since 2017, the diagnostic workup incorporated next-generation sequencing (NGS) with a targeted panel of 42 genes. BM MRD was assessed by multiparameter flow cytometry or molecular monitoring of NPM1 transcripts (as described by Gorello et al. and reported in our group by Bataller et al. [24].), rearrangements RUNX1::RUNX1T1 and CBFB::MYH11. MFC studies were not centralized, although standard protocols were recommended to the participating laboratories.
Statistical analyses
Categoric variables were compared with Chi-square and Fisher exact tests, and the Student-T test or the Mann-Whitney method was used for numeric parameters. All tests were two-sided and considered significant if p < 0.05. Outcomes such as overall survival (OS), event-free survival (EFS), relapse, and non-leukemic death were defined per standard criteria [25]. Early leukemia relapse was AML recurrence before the intended treatment (CT or alloHCT). Survival probabilities were calculated according to the Kaplan-Meier method, and cumulative incidences were estimated considering the competing risks. Survival probabilities were compared using the log-rank test and cumulative incidences with the Gray method.
To develop a new scoring system, we performed an exploratory univariate analysis of the impact on OS of the main clinical and biological parameters at diagnosis (supplementary Table 1). We integrated those with p < 0.1 in multivariable Cox regression models. The variables that retained significance in the multivariable analysis were included in the model and were assigned integer scores of 0, 1, or 2 based on their hazard ratios, with higher scores indicating greater risk. To assess multicollinearity and verify the viability of the model, the variance inflation factor (VIF) was calculated using the vif() function in R. The discriminative power of the model was assessed using Harrell’s concordance index [26], calculated with the survConcordance function in R. To evaluate survival predictions based on MRD status or alloHCT, we included patients in CR1 at Cons-1 (second course of CT in most cases) and performed a landmark analysis censored at Cons-1 or at the time of transplantation, respectively. All statistical analyses were performed with SPSS (version 29) and R statistics version 4.4.0 (R core Team, R Foundation for Statistical Computing, Vienna, Austria).
Results
Patient characteristics
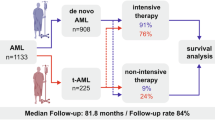
Between January 2012 and July 2022, 1054 patients were assessed, and 1034 received at least one dose of induction CT at 15 university hospitals; of them, 49% were women, the median age at diagnosis was 55 years (range 18–70). Other characteristics are described in Table 1. Patients above 60 years (from now considered the older cohort) presented a less proliferative disease (lower WBC, BM blasts, and LDH), and higher creatinine and bilirubin levels. Cytogenetic characterization was available in 95% of patients (n = 979); in the remaining 55 patients, metaphases were not optimal. According to the ELN-22 cytogenetic classification, 115 (12%) patients were favorable-risk, 657 (67%) intermediate-risk, and 207 (21%) cases had an adverse karyotype. Of the latter, 127 had a complex karyotype (CK), monosomal karyotype (MK) or both. Core binding factor (CBF) AML was two times more frequent in younger patients (14% vs. 7% for young and older groups, respectively, p < 0.001). NGS was performed in 296 patients, and the most frequently mutated genes were FLT3 (34%), NPM1 (34%), and DNMT3A (33%), followed by TET2 (16%), NRAS (14%), IDH2 (13%), and IDH1 (13%) (supplementary Fig. 1). TP53 alterations (deleted or mutated; TP53alt) were observed in 9% of cases analyzed. Patients above 60 years predominantly presented mutations in dysplasia-related genes and epigenetic regulators. Thus, the proportion of patients with either DNMT3A, TET2 or ASXL1, mutation (DTA) was 65% (71/109) in older adults vs. 42% (78/186) in younger patients (p < 0.001), and splicing mutations appeared in 22% of patients above 60 years of age in contrast to 11% of younger patients (p = 0.009). Further distribution of patients is depicted in the consort diagram (Fig. 1). According to the ELN-22 cytogenetic and molecular risk classification, 328 patients (32%) were considered favorable, while 405 (39%) were intermediate, and 301 (29%) adverse-risk with similar distribution in both age groups (p = 0.3).

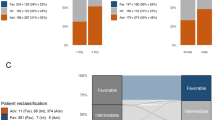
Each level represents a treatment cycle. Colors refer to ELN-22 risk category (blue: favorable, yellow: intermediate and red: adverse), and within them patients are distributed according to different genetic categories and age groups (n ≤ 60 | n > 60 years). Smaller squares between cycles show n of patients who discontinued protocol and their causes. CETLAM-fav includes ELN-22 favorable genetic categories plus NPM1mut/FLT3low. AlloHCT allogeneic stem cell transplant, CR1 first complete remission, CEBPAbi CEBPAbzip.
Induction therapy
CR was achieved in 792 (77%) of the 1034 patients. In 708 (89%) of the patients that achieved remission, only one course of induction CT was needed. A total of 124 (12%) patients were refractory, and 112 (11%) died due to complications during induction. Patients up to the age of 60 years presented a higher CR1 rate than those above that age (79% vs. 73%, respectively; p = 0.03) due to a higher induction death rate in the older cohort (8% in the young vs. 15% in the older cohort; p < 0.001). CR1 rates also differed according to genetics (Fig. 2 and supplementary Fig. 2) and ranged between 100% (17/17) in patients with biallelic CEBPA (CEBPAbi) mutation to 56% (74/132) and 33% (7/21) in patients with CK/MK/TP53alt and MECOM rearrangements (MECOMr), respectively.

Each bar shows the percentage of patients within a genetic category (legend on the left) who achieved complete remission (green), refractory disease (yellow) or induction death (red).
Post-remission therapy
Ninety-five percent of patients who achieved CR1 (751 out of 792) proceeded to Cons-1. The consort diagram illustrates the causes of protocol discontinuation before this point.
Death during Cons-1 occurred in 4 patients ( < 1%) and 718 (96%) patients remained in remission afterwards, whereas an early leukemia relapse was observed in 3% (7/282), 5% (13/289), and 5% (9/180) of favorable, intermediate, and adverse ELN-22 genetic risk patients respectively (p = 0.6) without significant differences among the two age groups. The outcome of patients in remission according to their ELN-22 genetic risk will be discussed next. Of note, given that our group considers NPM1mut/FLT3low patients as favorable-risk (thus not transplanted in CR1 but only in the case of a molecular relapse or in CR2), the outcome of NPM1mut/FLT3low cases will be described among the favorable category (from now CETLAM-fav) and not in the intermediate group, in all others, the ELN-22 classification was retrospectively applied.
Patients with favorable genetics
Two additional HDAC courses were feasible in 261 (68%) of the 383 initially diagnosed CETLAM-fav patients, 74% of the younger (187/252) and 57% (74/131) of the older adults (p < 0.001), and in 80% and 69% of the young and older patients in CR1 (p = 0.03).
Causes for protocol discontinuation during consolidations are described in the consort diagram. Among them, 18 patients in CR1 were bridged directly to alloHCT due to MRD positivity (n = 12), sustained aplasia (n = 3), or protocol deviation (n = 3). By the end of Cons-3, 218 (88%) of 249 patients with data available remained MRD negative and continued close monitoring [24].
Per protocol, in patients with MRD persistence after Cons-3, the intention was alloHCT in CR1. MRD positive status at this point was infrequent (n = 31, 12%), and alloHCT was performed in 17 (55%) of them.
Patients with intermediate and adverse genetics with indication of alloHCT in CR1
One-hundred seventy (49%) of the 350 initially diagnosed intermediate-risk AML and 66% of the patients in CR1 from this group completed the protocol from diagnosis to alloHCT in CR1. This procedure was performed in 71% (119/167) and 57% (51/89) of the patients in remission in the younger and older cohorts, respectively (p = 0.02). Forty-nine (21%) of 229 intermediate-risk patients in CR1 following Cons-1 did not reach alloHCT in CR1. This was mainly attributed to early leukemia relapse (41%; n = 20) or because they were considered unfit for the procedure due to CT toxicities (33%, n = 16). The latter was more frequent in the older adult cohort (n = 13) than in younger patients (n = 3).
Concerning the adverse category, 123 patients received an alloHCT in CR1. This represented 41% of the patients initially considered adverse-risk according to ELN-22 genetics and 64% of these patients in remission. When stratified by age, alloHCT in CR1 was achieved in 85 (47%) of 180 younger and 38 (31%) of 121 older adult adverse-risk patients (p = 0.006); if restricted to patients in CR1, this represented 72% (85/118) and 51% (38/75) of the young and older adults (p = 0.003). Different genetic subsets had an impact on the transplant feasibility: alloHCT was performed in CR1 in 3 (14%) of 21 MECOM-AML patients, 41 (31%) of 132 CK/MK/TP53alt cases, and 79 (53%) of 148 patients with other adverse genomic lesions (p < 0.001). Forty-six (27%) of the 170 adverse genetics patients in CR1 following Cons-1 were not transplanted in CR1; in 48% of these cases (n = 22), the reason was an early relapse, most of which happened in patients with CK/MK/TP53alt AML (50%, n = 11). Toxicities during CT precluded alloHCT in 10 cases, 7 of them older adults. Finally, 5 adverse-risk patients died during the Cons phase, and all but one belonged to the CK/MK/TP53alt category.
Time-dependent outcomes
After a median follow-up of 45 months (95%CI 40-50), the median OS of the whole cohort was 33 months, and the 4-year (4-yr) OS, cumulative incidence of relapse (CIR), and EFS were 46 ± 2%, 37 ± 3%, and 38 ± 2% respectively. Among each age group, 4-yr OS was 53 ± 2% vs 33 ± 3% for patients ≤ or > 60 years (p < 0.001, Fig. 3). Survival curves for other age subgroups are available in supplementary Fig. 3.

Overall survival (OS) and event-free survival (EFS) are shown on the left and middle figures, respectively. In these, the overall cohort outcome is shown in black, younger patients in red and older patients in blue. The right figure shows cumulative incidence of relapse (CIR) and non-relapse mortality (NRM) of the older (blue) and younger (red) patients.
Overall, patients ≤60 years had a lower relapse incidence; 4-yr CIR 34 ± 2% vs. 43 ± 3% for the young and older cohorts, respectively (p = 0.017), and older patients presented higher 4-yr non-leukemic death (NLD): 12 ± 2% vs 18 ± 3% in young and older adults, respectively (p = 0.024, Fig. 3).
Survival outcomes of each genetic subset and in the two age groups appear in Table 2. When stratified according to ELN-2022 classification, OS and EFS for each risk group was 68 ± 3% and 56 ± 3% in favorable patients, 41 ± 3% and 35 ± 3% for intermediate and 28 ± 3% and 24 ± 3% for the adverse-risk group, albeit with clear differences among younger and older patients (Fig. 4 and supplementary Fig. 4).

For the latter the favorable group includes ELN-22 favorable-risk genetics and NPM1mut/FLT3low, the very adverse group refers to CK/MK/TP53alt/MECOMr and the intermediate group contains all other patients.
Of note, in the series reported here, the three genetic groups showing the best clinical discrimination were favorable (as in CETLAM-fav, which included favorable genetics according to ELN-2022 plus patients with NPM1mut/FLT3low), adverse (with either CK/MK/TP53alt/MECOMr), and intermediate including the remaining patients. OS and EFS in these categories at 4-years were 70 ± 3% and 57 ± 3%; 15 ± 3% and 11 ± 3%; and 38 ± 3% and 32 ± 2%, respectively, (p < 0.001 for both OS and EFS, Fig. 4).
Median OS was not reached in patients with RUNX1::RUNX1T1 or CEBPAbi, regardless of age (supplementary Fig. 5). Lower OS was observed in older adults with CBFB::MYH11 (4-yr OS 66 ± 8% vs 43 ± 13% for young and older, respectively; p = 0.016) due to the high toxic death rate in the older group (7 [50%] of 14 cases) compared to younger patients (4 [9%] out of 44 patients; p < 0.001), whereas no differences in relapse rates were found (4-yr CIR 33% vs 26% in the same groups respectively, p = 0.5). In NPM1mut/FLT3low patients, survival was high in both age groups and matched or even surpassed that of NPM1mut/FLT3wt patients. Patients older than 60 years with CETLAM-fav genetics had a remarkable 4-yr OS of 59 ± 5%, in contrast to the poor outcome of this age group in the presence of intermediate and adverse genetics (4-yr OS 23 ± 4% and 10 ± 3%, median OS of 16 and 9 months, respectively; p < 0.001). Older adults had worse survival in the presence of KMT2A rearrangements (median OS of 98 months in younger vs. 8 months in older patients p = 0.033) and in those with dysplasia-related mutations (median OS not reached vs 17 months, respectively, p = 0.009, Table 2). Finally, the survival of adverse-risk patients with either CK/MK/TP53alt/MECOMr was dismal for both age groups: 4-yr OS 18 ± 5% in younger vs 10 ± 4% in older adults (p = 0.2, median OS of 9 months for both groups). Further outcomes regarding EFS are shown in supplementary Fig. 5.
MRD
MRD data were available in 629 (88%) of 718 patients in CR1 following Cons-1. MRDneg status was achieved in 459 evaluable patients (73%), with no differences in rates of MRDneg in each age group (MRDneg in 314 (75%) patients ≤60 yrs and 145 (69%) in >60 years, p = 0.15). In the landmark analysis, MRDneg status was associated with improved OS compared to MRDpos patients (4-yr OS 64 ± 3% vs. 53 ± 4% in MRDneg and MRDpos; p = 0.015). MRDneg patients also presented with higher EFS (4-yr EFS 55 ± 3% vs. 48 ± 4%, p = 0.039) and lower CIR (4-yr CIR 32 ± 2% vs. 40 ± 2% for the same groups respectively, p = 0.029; supplementary Fig. 6).
Outcomes of alloHCT in CR1 for intermediate and adverse-risk patients
Among 293 non-favorable patients transplanted after consolidation as per protocol, 70% were ≤60 years old, and 30% were older adults (supplementary Table 2). Non-relapse mortality at 100 days, 6 months, and 1 year from transplant was 3%, 9%, and 14% in patients ≤ 60 years and 5%, 14%, and 15% in those >60 years (p = 0.3). There were no differences in outcome after alloHCT for intermediate risk-patients depending on age with a 4-yr OS from transplant of 58 ± 5% and 49 ± 8% in young and older groups, respectively (p = 0.1). Older adults with ELN2022 adverse genetics had a 4 yr OS from transplant of 34 ± 8%, compared to younger adults who presented 4-yr OS of 48 ± 6%, respectively (p = 0.06). In the most adverse subgroup (CK/MK/TP53alt/MECOMr), 4-yr OS from transplant was dismal regardless of age, in younger patients was 20 ± 8 (with identical 4-yr EFS) and older adults presented 4-yr OS and EFS of 18 ± 9%.
Prognostic factors and ICSA risk score
The variables that retained an independent prognostic impact in the multivariable analysis for OS were age ( ≤ 60 vs. >60 years), gender (female/male), ECOG (0–2, ≥3), WBC counts ( ≤ 20, 21-99, >99×109/L), increased creatinine ( > 1,2 mg/dL), bilirubin above average ( > 1.2 mg/dL), and genetic category (CETLAM-fav, CK/MK/TP53alt/MECOMr, other). Multicollinearity among these variables was minimal according to VIF values (range 1.05-2.11) hence they were integrated into a scoring system (ICSA: Intensive Chemotherapy Score for AML, Fig. 5). Each patient’s total score was calculated (range 0–9) and, based on their survival impact, six risk groups were defined: very low (0 points), low (1 points), intermediate-low (2 points), intermediate-high (3 points), high (4–5 points), and very high (6–9 points). The C-index for the model was 0.71, and the 4-yr OS for each risk category was 85 ± 6%, 70 ± 4%, 55 ± 4%, 36 ± 4%, 18 ± 4%, and 0%, respectively (p < 0.001). Regarding EFS, the score identified five groups since very-low and low categories had comparable outcomes. Of note, we confirmed that the score discriminated survival risk groups equally well for younger and older patients separately, and also that the ICSA risk groups correlated with induction results: very low risk patients had CR1 rates of 100% (46 out of 46 patients), that progressively decreased in each risk category. Similarly, the number of refractory patients and induction deaths ascended progressively as the patient risk increased (supplementary material).

WBC white blood cells, CK complex karyotype, MK monosomal karyotype.
Finally, this model was validated using an external retrospective cohort of 581 AML patients treated intensively within a previous CETLAM protocol (AML-03, NCT01723657). Patient characteristics from this series are available in supplementary Table 3; limited molecular analyses were available, and patients were mostly risk-stratified by cytogenetics, NPM1, and FLT3 mutations. In the validation cohort, ICSA segregated patients in 5 risk groups both for OS (4-yr OS in each risk category of 75%, 67%, 37%, 32%, 21%, and 0%; p < 0.001) and for EFS (p < 0.001; Fig. 6) and the model yielded a C-index of 0.66.

The table shows for each ICSA risk group the distribution of patients, the OS and the c-index for both the model-building cohort (AML-12 protocol) and the validation cohort (AML-03 protocol).
Discussion
Intensive CT, followed when possible by alloHCT, has remained the treatment of choice for adult AML in fit patients for more than 45 years. Recently, it has been demonstrated that specific subsets of patients benefit from the addition to CT of FLT3 inhibitors [18, 27], conjugated monoclonal antibodies [28], or the use of novel forms of chemotherapy delivery [29]. Retrospective studies and ongoing trials are exploring BCL2 inhibitors to further improve the results of intensive CT [15,16,17, 30, 31]. The field of alloHCT has also evolved with the increased availability of donors, stem cell sources and technique refinements improving their results.
It is known that intensive therapy for AML leads to toxicity, requires prolonged hospitalization and a meaningful proportion of patients will die due to therapy-related complications. Treatment efficacy varies broadly, mainly depending on the patient’s age and genetic characteristics of the AML cells [32]. The study results reported here reflect the heterogeneity of fit patients with AML and how clinical and biological features impact on the outcome. Also, the current report shows in an extensive series over 10 years that the treatment plan is not always feasible, primarily due to toxicities, early leukemia recurrence, or even protocol deviations in real life. We also observed that a high proportion of patients with favorable features may be cured with CT only, without the need for an alloHCT. We, similarly to other groups [33,34,35,36], confirmed that MRD persistence after CT leads to increased relapse incidence and worse survival even when MRD assessment was not centralized. Since data on MRD just before alloHCT was unavailable, we could not analyze the impact of this feature on post-transplant outcomes.
Chronological age strongly impacted CR achievement, relapse, survival, and EFS. Sixty years is the most frequent cut-off for considering patients as “older fit” due to their higher prevalence of adverse-risk genetics, increased comorbidities and overall worse outcome to standard chemotherapy [3, 10]. In our cohort, patients under 60 years achieved a remarkable CR rate of 79%; only 8% died during induction, and their 4-year OS was 53%; in contrast, the values in the older adult group were 73%, 15%, and 33%, respectively. Hence, although all patients were initially considered fit, the likelihood of long-term survival for older adults was compromised in our series due to more frequent death during consolidation, early relapses, and less feasibility of allogeneic transplantation. Therefore, alternative approaches are needed to overcome these drawbacks.
Genetics of AML also had an evident influence on outcome. Our report provides a detailed description of response and evolution depending on genetic characterization at diagnosis and is shown in Table 2 and Figs. 1 and 2 and the additional material in the supplement; it is remarkable that patients with favorable genetics according to ELN-2022 had very low chemoresistance (less than 6%). In contrast, patients with AML and MECOMr or TP53alt, even in the absence of monosomal or complex karyotype, had low CR rates, which emphasizes that investigational approaches for first-line treatment are needed in this poor-risk population. One limitation of our study is that only 37% (378/1034) of patients had molecular TP53 testing. However, 73% of the 656 cases with unknown TP53 mutational status were genetically classified with either karyotype or ELN-22 risk mutations which allowed for 77% of the whole cohort to be comprehensively stratified.
Our report validated in a larger cohort of patients a previous observation made by our group [23] that the best prognostic discrimination in newly diagnosed AML appeared when grouping genetics as CETLAM-fav, very adverse as in CK/MK/TP53alt/MECOMr, and other genetics regardless of belonging to the intermediate or adverse ELN-2022. The 4-yr OS in these three groups was 70%, 15%, and 38%, respectively. Regarding the favorable genetics category, the results were very good in the whole cohort, including patients with NPM1 mutation and low allelic ratio of FLT3-ITD [37]. Remarkably, older adults with favorable genetics had a 4-year OS around 60%, supporting intensive CT in favorable patients up to the age of 70. In concordance with other groups, a dismal outcome was observed in patients with CK/MK/TP53alt/MECOMr [38,39,40,41,42,43]. In contrast to other reports, we were able to extensively compile causes that precluded alloHCT, mostly low CR rate, frequent early relapse, and treatment-related toxicities. For the time being, alloHCT remains the only option, supported by the fact that in our report, 44% of younger ELN-22 adverse-risk transplanted patients remained event-free at 4 years, albeit 4-yr EFS from transplant was only 20% in the younger most adverse subset (CK/MK/TP53alt/MECOMr). In-depth discussion with patients is recommended before performing alloHCT in this situation, and novel strategies are, therefore, needed in these very adverse patients.
Clinical status and laboratory findings at diagnosis impacted survival in the univariate and multivariate analyses; ECOG > 2, high leukocyte counts, creatinine and/or bilirubin above the normal value were associated with worse survival. Females had better outcomes than males due to less mortality and relapses; in fact, adverse clinical features such as age >60 years, elevated creatinine and/or bilirubin, and adverse genetics were more frequent in males (data not shown). The influence of gender on the results of treatment for AML has also been reported in other series [44, 45] and a recent report suggests that there may be sex-specific cell programs influencing leukemogenesis and leukemic cell responses [46].
Based on these baseline characteristics, it was possible to establish a score that defined risk groups regarding induction response, OS and EFS and was validated in an independent cohort. Although other scores have been described in AML, most of them focus on comorbidities to define fitness and estimate the mortality related to induction chemotherapy [9, 11, 47] but lack prediction on OS and EFS [48, 49]. Others are exclusively for older patients ( > 70 years) [50] or predict survival once CR1 is achieved [51]. In this regard, a recent score for patients above 60 years eligible for intensive CT has been developed which segregates patients into 4 risk groups according to genetics (AML60 + ) and improved the ELN-22 stratification in older patients [52]. In our cohort, the AML60+ score segregated patients >60 years into three risk groups, possibly because median age of this group was younger compared to the study by Versluis, and the proportion of adverse-risk cases was lower. Similarly to our study, MK and TP53mut conferred patients the highest risk and worse outcome independently of age (supplementary material).
ICSA applies to the adult population most frequently susceptible to receive intensive chemotherapy (18–70 years), it is easy to calculate, and gives simultaneous information of response rate, OS and EFS based on clinical and genetic diagnostic features, therefore orienting clinicians on which route of treatment to consider at initial diagnosis. Overall, the ICSA score identifies patients with a high likelihood of being cured with an intensive approach (CT +/- alloHCT) and, in contrast, others that despite being initially considered “fit for IC”, alternative strategies of treatment deserve investigation.
In summary, in a cohort of more than 1000 patients with AML receiving a homogeneous CT protocol, we identified a considerable proportion of patients with favorable outcomes who do not need an alloHCT in CR1. In contrast, there is another group of patients harboring very adverse genetic features with low CR rates, frequent chemoresistance, and early relapses in which transplantation was frequently not feasible where investigational approaches are needed. In between, a large proportion of patients benefit from an alloHCT that, in our hands, was performed in around 70% of patients that achieved remission. We observed that results were different depending on age, with poorer prognosis with CT in patients above 60 years of age. In this group, CT vs. less intensive treatment as the combination of venetoclax and hypomethylating agents deserves investigation in prospective randomized studies. Finally, a reproducible and simple scoring system was developed to predict survival based on the patient baseline characteristics, which may be useful in informing patients and supporting treatment decisions.
Data availability
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
References
Sant M, Allemani C, Tereanu C, De Angelis R, Capocaccia R, Visser O, et al. Incidence of hematologic malignancies in Europe by morphologic subtype: results of the HAEMACARE project. Blood. 2010;116:3724–34.
Juliusson G, Lazarevic V, Hörstedt AS, Hagberg O, Höglund M. Acute myeloid leukemia in the real world: why population-based registries are needed. Blood. 2012;119:3890–9.
Kantarjian H, Kadia T, DiNardo C, Daver N, Borthakur G, Jabbour E, et al. Acute myeloid leukemia: current progress and future directions. Blood Cancer J. 2021;11:41.
Ocias LF, Larsen TS, Vestergaard H, Friis LS, Abildgaard N, Frederiksen H, et al. Trends in hematological cancer in the elderly in Denmark, 1980-2012. Acta Oncol. 2016;55:98–107.
Visser O, Trama A, Maynadie M, Stiller C, Marcos-Gragera R, De Angelis R, et al. Incidence, survival and prevalence of myeloid malignancies in Europe. Eur J Cancer. 2012;48:3257–66.
Deschler B, de Witte T, Mertelsmann R, Lübbert M. Treatment decision-making for older patients with high-risk myelodysplastic syndrome or acute myeloid leukemia: problems and approaches. Haematologica. 2006;91:1513–22.
Fenwarth L, Thomas X, de Botton S, Duployez N, Bourhis JH, Lesieur A, et al. A personalized approach to guide allogeneic stem cell transplantation in younger adults with acute myeloid leukemia. Blood. 2021;137:524–32.
Malfuson JV, Etienne A, Turlure P, de Revel T, Thomas X, Contentin N, et al. Risk factors and decision criteria for intensive chemotherapy in older patients with acute myeloid leukemia. Haematologica. 2008;93:1806–13.
Walter RB, Othus M, Borthakur G, Ravandi F, Cortes JE, Pierce SA, et al. Prediction of early death after induction therapy for newly diagnosed acute myeloid leukemia with pretreatment risk scores: a novel paradigm for treatment assignment. J Clin Oncol. 2011;29:4417–23.
Oran B, Weisdorf DJ. Survival for older patients with acute myeloid leukemia: a population-based study. Haematologica. 2012;97:1916–24.
Ferrara F, Barosi G, Venditti A, Angelucci E, Gobbi M, Pane F, et al. Consensus-based definition of unfitness to intensive and non-intensive chemotherapy in acute myeloid leukemia: a project of SIE, SIES and GITMO group on a new tool for therapy decision making. Leukemia. 2013;27:997–9.
Pratz KW, Jonas BA, Pullarkat V, Thirman MJ, Garcia JS, Dohner H, et al. Long-term follow-up of VIALE-A: Venetoclax and azacitidine in chemotherapy-ineligible untreated acute myeloid leukemia. Am J Hematol. 2024;99:615–24.
Wei AH, Panayiotidis P, Montesinos P, Laribi K, Ivanov V, Kim I, et al. 6-month follow-up of VIALE-C demonstrates improved and durable efficacy in patients with untreated AML ineligible for intensive chemotherapy (141/150). Blood Cancer J. 2021;11:163.
Short NJ, Ong F, Ravandi F, Nogueras-Gonzalez G, Kadia TM, Daver N, et al. Impact of type of induction therapy on outcomes in older adults with AML after allogeneic stem cell transplantation. Blood Adv. 2023;7:3573–81.
Matthews AH, Perl AE, Luger SM, Gill SI, Lai C, Porter DL, et al. Real-world effectiveness of intensive chemotherapy with 7&3 versus venetoclax and hypomethylating agent in acute myeloid leukemia. Am J Hematol. 2023;98:1254–64.
Pollyea DA, Winters A, McMahon C, Schwartz M, Jordan CT, Rabinovitch R, et al. Venetoclax and azacitidine followed by allogeneic transplant results in excellent outcomes and may improve outcomes versus maintenance therapy among newly diagnosed AML patients older than 60. Bone Marrow Transpl. 2022;57:160–6.
Ossenkoppele G, Vyas P. BCL-2 Inhibitor and Conventional Chemotherapy Combinations for Acute Myeloid Leukemia: Shifting From the Unfit to the Fit Patient With AML. J Clin Oncol. 2020;38:3461–4.
Stone RM, Mandrekar SJ, Sanford BL, Laumann K, Geyer S, Bloomfield CD, et al. Midostaurin plus Chemotherapy for Acute Myeloid Leukemia with a FLT3 Mutation. N. Engl J Med. 2017;377:454–64.
Mayer RJ, Davis RB, Schiffer CA, Berg DT, Powell BL, Schulman P, et al. Intensive postremission chemotherapy in adults with acute myeloid leukemia. Cancer and Leukemia Group B. N. Engl J Med. 1994;331:896–903.
Dohner H, Estey EH, Amadori S, Appelbaum FR, Buchner T, Burnett AK, et al. Diagnosis and management of acute myeloid leukemia in adults: recommendations from an international expert panel, on behalf of the European LeukemiaNet. Blood. 2010;115:453–74.
Döhner H, Estey E, Grimwade D, Amadori S, Appelbaum FR, Büchner T, et al. Diagnosis and management of AML in adults: 2017 ELN recommendations from an international expert panel. Blood. 2017;129:424–47.
Pratcorona M, Brunet S, Nomdedeu J, Ribera JM, Tormo M, Duarte R, et al. Favorable outcome of patients with acute myeloid leukemia harboring a low-allelic burden FLT3-ITD mutation and concomitant NPM1 mutation: relevance to post-remission therapy. Blood. 2013;121:2734–8.
Bataller A, Garrido A, Guijarro F, Onate G, Diaz-Beya M, Arnan M, et al. European LeukemiaNet 2017 risk stratification for acute myeloid leukemia: validation in a risk-adapted protocol. Blood Adv. 2022;6:1193–206.
Bataller A, Onate G, Diaz-Beya M, Guijarro F, Garrido A, Vives S, et al. Acute myeloid leukemia with NPM1 mutation and favorable European LeukemiaNet category: outcome after preemptive intervention based on measurable residual disease. Br J Haematol 2020.
Cheson BD, Bennett JM, Kopecky KJ, Buchner T, Willman CL, Estey EH, et al. Revised recommendations of the International Working Group for Diagnosis, Standardization of Response Criteria, Treatment Outcomes, and Reporting Standards for Therapeutic Trials in Acute Myeloid Leukemia. J Clin Oncol. 2003;21:4642–9.
Harrell FE Jr, Califf RM, Pryor DB, Lee KL, Rosati RA. Evaluating the yield of medical tests. JAMA. 1982;247:2543–6.
Erba HP, Montesinos P, Kim HJ, Patkowska E, Vrhovac R, Zak P, et al. Quizartinib plus chemotherapy in newly diagnosed patients with FLT3-internal-tandem-duplication-positive acute myeloid leukaemia (QuANTUM-First): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet. 2023;401:1571–83.
Castaigne S, Pautas C, Terre C, Raffoux E, Bordessoule D, Bastie JN, et al. Effect of gemtuzumab ozogamicin on survival of adult patients with de-novo acute myeloid leukaemia (ALFA-0701): a randomised, open-label, phase 3 study. Lancet. 2012;379:1508–16.
Lancet JE, Cortes JE, Hogge DE, Tallman MS, Kovacsovics TJ, Damon LE, et al. Phase 2 trial of CPX-351, a fixed 5:1 molar ratio of cytarabine/daunorubicin, vs cytarabine/daunorubicin in older adults with untreated AML. Blood. 2014;123:3239–46.
DiNardo CD, Lachowiez CA, Takahashi K, Loghavi S, Xiao L, Kadia T, et al. Venetoclax Combined With FLAG-IDA Induction and Consolidation in Newly Diagnosed and Relapsed or Refractory Acute Myeloid Leukemia. J Clin Oncol. 2021;39:2768–78.
Cherry EM, Abbott D, Amaya M, McMahon C, Schwartz M, Rosser J, et al. Venetoclax and azacitidine compared with induction chemotherapy for newly diagnosed patients with acute myeloid leukemia. Blood Adv. 2021;5:5565–73.
Dohner H, Wei AH, Appelbaum FR, Craddock C, DiNardo CD, Dombret H, et al. Diagnosis and management of AML in adults: 2022 recommendations from an international expert panel on behalf of the ELN. Blood. 2022;140:1345–77.
Dillon R, Potter N, Freeman S, Russell N. How we use molecular minimal residual disease (MRD) testing in acute myeloid leukaemia (AML). Br J Haematol. 2021;193:231–44.
Heuser M, Freeman SD, Ossenkoppele GJ, Buccisano F, Hourigan CS, Ngai LL, et al. 2021 Update on MRD in acute myeloid leukemia: a consensus document from the European LeukemiaNet MRD Working Party. Blood. 2021;138:2753–67.
Short NJ, Zhou S, Fu C, Berry DA, Walter RB, Freeman SD, et al. Association of Measurable Residual Disease With Survival Outcomes in Patients With Acute Myeloid Leukemia: A Systematic Review and Meta-analysis. JAMA Oncol. 2020;6:1890–9.
Othman J, Potter N, Ivey A, Jovanovic J, Runglall M, Freeman SD, et al. Postinduction molecular MRD identifies patients with NPM1 AML who benefit from allogeneic transplant in first remission. Blood. 2024;143:1931–6.
Onate G, Pratcorona M, Garrido A, Artigas-Baleri A, Bataller A, Tormo M, et al. Survival improvement of patients with FLT3 mutated acute myeloid leukemia: results from a prospective 9 years cohort. Blood Cancer J. 2023;13:69.
Papaemmanuil E, Gerstung M, Bullinger L, Gaidzik VI, Paschka P, Roberts ND, et al. Genomic Classification and Prognosis in Acute Myeloid Leukemia. N. Engl J Med. 2016;374:2209–21.
Middeke JM, Herold S, Rucker-Braun E, Berdel WE, Stelljes M, Kaufmann M, et al. TP53 mutation in patients with high-risk acute myeloid leukaemia treated with allogeneic haematopoietic stem cell transplantation. Br J Haematol. 2016;172:914–22.
Zhao D, Zarif M, Zhou Q, Capo-Chichi JM, Schuh A, Minden MD, et al. TP53 Mutations in AML Patients Are Associated with Dismal Clinical Outcome Irrespective of Frontline Induction Regimen and Allogeneic Hematopoietic Cell Transplantation. Cancers (Basel) 2023;15.
Nawas MT, Kosuri S. Utility or futility? A contemporary approach to allogeneic hematopoietic cell transplantation for TP53-mutated MDS/AML. Blood Adv. 2024;8:553–61.
Badar T, Atallah E, Shallis R, Saliba AN, Patel A, Bewersdorf JP, et al. Survival of TP53-mutated acute myeloid leukemia patients receiving allogeneic stem cell transplantation after first induction or salvage therapy: results from the Consortium on Myeloid Malignancies and Neoplastic Diseases (COMMAND). Leukemia. 2023;37:799–806.
Caiado F, Maia-Silva D, Jardim C, Schmolka N, Carvalho T, Reforco C, et al. Lineage tracing of acute myeloid leukemia reveals the impact of hypomethylating agents on chemoresistance selection. Nat Commun. 2019;10:4986.
Acharya UH, Halpern AB, Wu QV, Voutsinas JM, Walter RB, Yun S, et al. Impact of region of diagnosis, ethnicity, age, and gender on survival in acute myeloid leukemia (AML). J Drug Assess. 2018;7:51–53.
Linet MS, Curtis RE, Schonfeld SJ, Vo JB, Morton LM, Dores GM. Survival of adult AML patients treated with chemotherapy in the U.S. population by age, race and ethnicity, sex, calendar-year period, and AML subgroup, 2001-2019. EClinicalMedicine. 2024;71:102549.
Ozga M, Nicolet D, Mrozek K, Yilmaz AS, Kohlschmidt J, Larkin KT, et al. Sex-associated differences in frequencies and prognostic impact of recurrent genetic alterations in adult acute myeloid leukemia (Alliance, AMLCG). Leukemia. 2024;38:45–57.
Sorror ML, Storer BE, Fathi AT, Gerds AT, Medeiros BC, Shami P, et al. Development and Validation of a Novel Acute Myeloid Leukemia-Composite Model to Estimate Risks of Mortality. JAMA Oncol. 2017;3:1675–82.
Palmieri R, Othus M, Halpern AB, Percival MM, Godwin CD, Becker PS, et al. Accuracy of SIE/SIES/GITMO Consensus Criteria for Unfitness to Predict Early Mortality After Intensive Chemotherapy in Adults With AML or Other High-Grade Myeloid Neoplasm. J Clin Oncol. 2020;38:4163–74.
Desprez C, Riou J, Peterlin P, Marchand T, Couturier MA, Villate A, et al. Comparison of scoring systems evaluating suitability for intensive chemotherapy in adults with acute myeloid leukemia-a Grand Ouest Against Leukemia (GOAL) study. Leukemia. 2022;36:2408–17.
Berard E, Rollig C, Bertoli S, Pigneux A, Tavitian S, Kramer M, et al. A scoring system for AML patients aged 70 years or older, eligible for intensive chemotherapy: a study based on a large European data set using the DATAML, SAL, and PETHEMA registries. Blood Cancer J. 2022;12:107.
Pfirrmann M, Ehninger G, Thiede C, Bornhauser M, Kramer M, Rollig C, et al. Prediction of post-remission survival in acute myeloid leukaemia: a post-hoc analysis of the AML96 trial. Lancet Oncol. 2012;13:207–14.
Versluis J, Metzner M, Wang A, Gradowska P, Thomas A, Jakobsen NA, et al. Risk Stratification in Older Intensively Treated Patients With AML. J Clin Oncol 2024; JCO2302631.
Acknowledgements
This work was supported in part by the Institut d’Investigació Biomèdica Sant Pau (IIB SANT PAU), the Jose Carreras Leukemia Research Foundation, the CERCA Programme/Generalitat de Catalunya (PERIS SLT00433 and 2021 SGR 01139 2021) and the Instituto de Salud Carlos III, Ministerio de Economía y Competitividad, Spain (PI17/01246,PI20/01621 and PI24/00013). The CETLAM Group receives unrestricted grant support from Jazz Pharmaceuticals (AMLDIAG_20 project), Novartis and Pfizer.
Author information
Authors and Affiliations
Contributions
JS designed the study, GO analyzed data and wrote the paper, EI performed statistical analysis and figures, JE supervised research and wrote the paper, AG coordinated the cooperative database and extracted data, the following authors treated patients, collected and provided data (MA, HP, EA, MT, MDB, SV, FVLL, AS, RC, OS, MC, AG, SGA, JB, XO), FG performed flow cytometry tests, LZ performed genetic analysis, MP performed next-generation analysis, JFN coordinated laboratory analysis and all authors revised the final manuscript.
Corresponding author
Ethics declarations
Competing interests
JS is member of the speaker bureau and advisory board of Jazz Pharmaceuticals, Astellas, Abbvie and Pfizer. JE reports participation in Advisory Boards of Abbvie, Novartis, Astellas, Jazz Pharmaceuticals, BMS-Celgene, Pfizer, Amgen and research grants from Novartis, Jazz Pharmaceuticals and Pfizer. The remaining authors declare no competing financial interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Oñate, G., Garrido, A., Arnan, M. et al. Diverse real-life outcomes after intensive risk-adapted therapy for 1034 AML patients from the CETLAM Group. Blood Cancer J. 15, 4 (2025). https://doi.org/10.1038/s41408-024-01205-5
Received:
Revised:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41408-024-01205-5
