
Abstract
Aim To examine whether there are ethnic inequalities in child oral health behaviours and the role of parental socioeconomic status (SES) in explaining them.
Methods Data from 2,186 five- and eight-year-olds of white, Asian, Black and other ethnicity, who participated in the 2013 Children's Dental Health Survey, were analysed. Parents reported their children's toothbrushing and dental attendance. Logistic regression was used to explore ethnic inequalities in child behaviours, adjusting for demographic factors and parental SES.
Results Children of Asian ethnicity were less likely to start brushing early in life (odds ratio [OR]: 0.25; 95% confidence interval [CI]: 0.15-0.43), brush regularly (OR: 0.56; 95% CI: 0.32-0.97) and have a check-up last year (OR: 0.28; 95% CI: 0.16-0.49) than those of white ethnicity. Children of Black ethnicity were less likely to have a check-up last year (OR: 0.39; 95% CI 0.17-0.89) than those of white ethnicity. Children of other ethnicity were less likely to start brushing early in life (OR: 0.41; 95% CI: 0.23-0.77) and brush regularly (OR: 0.45; 95% CI: 0.23-0.87) than children of white ethnicity. Inequalities in toothbrushing frequency and regular dental attendance between children of Black and white ethnicity were fully attenuated after adjustment for parental SES.
Conclusion There were ethnic inequalities in child toothbrushing and dental visiting, with children of Asian ethnicity being the most affected. Parental SES only explained part of these inequalities.
Key points
-
Healthy behaviours, including toothbrushing and dental attendance, start early in life.
-
This paper summarises current recommendations for toothbrushing and dental attendance behaviour from national and international organisations.
-
It discusses potential explanations for ethnic inequalities in child oral health behaviours.
Similar content being viewed by others
Introduction
Dental caries is a very common childhood disease that causes pain, eating difficulties and sleep disturbances, leading to low school performance, reduced growth and poor wellbeing in children.1,2 Dental caries is strongly influenced by behaviour.3 Regular toothbrushing with fluoride toothpaste is important to prevent dental caries.4 National and international organisations recommend that parents brush their child's teeth twice a day as soon as they erupt, which commonly occurs at around six months of age.5,6,7 Regular dental check-ups are also considered valuable for maintaining good oral health through the provision of primary and secondary prevention.8,9,10 It is generally recommended to have a first dental check-up no later than the child's first birthday and visits to the dentist every 3-12 months thereafter, depending on oral health needs and disease risk.5,6,7,11,12,13
Families play a pivotal role in the upbringing and development of children.14,15 They constitute the immediate social environment that provides children with values and beliefs, standards and the care they need for survival and maintenance within society.16 The family environment, in which children develop and thrive, plays an important role in the establishment of health behaviours early in life, as well as on children's health and wellbeing across the life course.17,18 There is also evidence that the care and socialisation of children vary depending on the ethnic background of families.19,20
Few studies have looked at ethnic inequalities in child oral health behaviours.21,22,23,24 Most of these studies reported no ethnic differences in the age when children started brushing,21 the age when children had their first dental visit,22 or child dental attendance.23 On the contrary, a study in Canada showed marked ethnic inequalities in regular toothbrushing (twice or more daily) between children of Arab (32.9%), Indonesian (36.7%) and white ethnicity (62.8%).24 Whether these differences are due to confounding factors, which are associated with both ethnicity and child behaviour, remains unclear. Previous studies have shown that socioeconomic circumstances entirely accounted for oral health disparities between Black and white ethnic groups in the United States.25,26 However, other studies have shown that ethnic inequalities in child oral health persist despite the fact ethnic groups are disproportionately overrepresented in the lower socioeconomic groups.27,28 Consequently, it is crucial to establish to what extent socioeconomic factors might explain ethnic differences in child oral health behaviours, as this might depend on the setting. No similar evaluation has been carried out in relation to child oral health behaviours. To fill these gaps in knowledge, a study was planned to examine whether there are ethnic inequalities in child oral health behaviours and the role of parental socioeconomic status (SES) in explaining those inequalities.
Methods
Study population
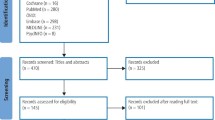
This study analysed existing data from the Children's Dental Health Survey (CDHS) 2013, which was a nationally representative survey of children aged 5, 8, 12 and 15 years, attending public schools in England, Wales and Northern Ireland. A total of 13,628 children were approached and invited to participate in the survey using multi-stage stratified sampling. Data were collected through clinical dental examinations for all children, parental questionnaires for primary school children (five- and eight-year-olds) and pupil questionnaires for secondary school children (12- and 15-year-olds). Of them, 9,866 children were clinically inspected (72%) and 4,214 of the parental questionnaires were returned (43%).29 The CDHS was ethically approved by the University College London ethics committee (ID: 2000/002). The present study did not require ethical approval or consent as it used anonymised, publicly available data.
Only data from primary schoolchildren (five- and eight-year-olds) were used because older children received a pupil questionnaire instead of a parental questionnaire and the set of items was different. Of the 2,423 primary schoolchildren who had clinical and questionnaire data, 237 were excluded because of missing data on ethnicity (n = 87), child oral health behaviours (n = 96), parental demographic factors (n = 60) and parental SES (n = 37). The study sample included 2,186 primary schoolchildren.
Measures
Child oral health behaviours were indicated by toothbrushing and dental attendance as reported by parents. For toothbrushing, parents were asked how old their child was when they started brushing their teeth or having them brushed for them (under six months; between six months and one year; between one and two years; between two and four years; between four and six years; six years of age or older; or my child does not brush their teeth) and how often the child usually brushed their teeth or had them brushed for them (more than three times a day; three times a day; twice a day; less than once a day; or never). Following international recommendations,5,6,7 the age when child brushing started was dichotomised as during the first year versus after the first year of life (reference category), whereas child toothbrushing frequency was dichotomised as twice or more per day versus once or fewer times per day (reference category). For dental visiting, parents were asked how old their child was when they first went to the dentist (answers were provided in years, and if the child was less than one year old, parents were asked to write a 0), when the child's last visit to the dentist was (in the last six months; in the last year; in the last two years; or more than two years ago) and whether the child went to the dentist for a check-up or for having trouble with their teeth. Following international recommendations,5,6,7,11,12,13 the age when the child had their first dental visit was dichotomised as during the first year versus after the first year of life (reference category), whereas information on time since last dental visit and reason for the visit were combined to generate a new variable with two categories: had a check-up in the past year versus did not have a check-up in the past year (reference category).
Child ethnicity was retrieved from school records according to the method used in the CDHS 2013 (Asian, Black, multiracial, white and other).29 For analysis, children of multiracial and other ethnicity were combined as 'other ethnic group' due to the small number of participants in these groups.
Parental and child demographic factors and parental SES were included in the analysis as confounders of the relationship between ethnicity and child oral health behaviours. Parental demographic factors were sex and age (in continuous years). Child demographic factors were sex, age (five- and eight-year-olds) and country of residency (England, Wales and Northern Ireland). Family SES was indicated by education and the National Statistics Socioeconomic Classification (NS-SEC). For education, parents reported their highest qualification for which they earned a certification (degree level or above; below degree level; and no qualifications). NS-SEC categories were created based on the self-coded method based on the current or most recent occupation, employment status, size of the organisation and supervisory status. The eight NS-SEC categories were combined into three groups, namely managerial and professional occupations, intermediate occupations and routine and manual occupations. For comprehensive coverage of the population, parents who had never worked, were unemployed for an extended period, or were not categorised for other causes were included as unclassified.30
Data analysis
Analysis was conducted in Stata/MP version 17 (StataCorp LLC, College Station, TX). Data were weighted to adjust for the unequal probability of selection, as well as non-response at school and student levels. Data analysis also considered the complex survey design (stratification and clustering) to generate valid standard errors and 95% confidence intervals (CIs). The characteristics of the study sample were first described in terms of child demographic factors (sex; age; ethnicity; and country of residence) and parental demographic factors (sex and age) and SES (education and NS-SEC groups). Ethnic inequalities in child oral health behaviours (age child started brushing; child toothbrushing frequency; age child had first dental visit; and child dental attendance) were evaluated in crude and adjusted survey logistic regression models because the four child oral health behaviours were binary outcomes. Odds ratios (OR) with 95% CIs were therefore reported as the measure of association. The modelling strategy was first to report crude associations of ethnicity with each child oral health behaviour (model 1), and gradually adjust for child and parental demographic factors (model 2) and additionally for parental SES (model 3). The attenuation in the estimates for the association of ethnicity with each child oral health behaviour was used to evaluate the role of SES in explaining ethnic inequalities in child oral health behaviours.
Results
Data from 2,186 children (1,136 and 1,050 five- and eight-year-olds, respectively) were analysed. The sociodemographic characteristics of the participating children are described in Table 1. Almost one-fifth (18.9%) of children were from minority ethnic groups, with children of Asian (8.1%) and Black ethnicity (4.7%) representing the largest minority ethnic groups. In addition, 76.2% of children started brushing in the first year of life and 83.4% brush their teeth twice or more daily, whereas 12.8% of children had their first dental visit during the first year of life and 87.8% had a dental check-up in the previous year.
The proportions of children who started brushing their teeth during the first year of life and who brushed their teeth twice or more daily were lower in every minority ethnic group than in the white ethnic group (Table 2). However, these differences were significant for children of Asian ethnicity (OR: 0.23; 95% CI: 0.15-0.35) and children of other ethnicity (OR: 0.42; 95% CI: 0.24-0.75) but not for children of Black ethnicity (OR: 0.77; 95% CI: 0.35-1.69). These differences remained significant after adjusting for child and parental demographic factors (model 2). After further adjustment for parental SES (model 3), ethnic differences in the age when the child started brushing their teeth remained significant (OR: 0.27; 95% CI: 0.16-0.46) for children of Asian ethnicity and for children of other ethnicity (OR: 0.44; 95% CI: 0.24-0.81), but were fully attenuated for child toothbrushing frequency (OR: 0.66; 95% CI: 0.37-1.16) and for children of Asian and other ethnicity, respectively (OR: 0.51; 95% CI: 0.26-1.01).
Furthermore, the proportion of children who visited the dentist in their first year of life and who had a dental check-up in the past year were lower in every minority ethnic group than in the white ethnic group (Table 3). However, ethnic differences in the age when the child had their first dental visit were not significant in crude or adjusted models. Differences in child dental attendance were significant for children of Asian ethnicity (OR: 0.25; 95% CI: 0.15-0.43) and children of Black ethnicity (OR: 0.37; 95% CI: 0.16-0.85), but not for children of other ethnicity (OR: 0.53; 95% CI: 0.25-1.13). These differences remained significant after adjusting for child and parental demographic factors (model 2). After further adjustment for parental SES (model 3), ethnic differences in having had a dental check-up in the past year remained significant for children of Asian ethnicity (OR: 0.30; 95% CI: 0.17-0.55) but were fully attenuated for children of Black ethnicity (OR: 0.47; 95% CI: 0.21-1.16).
Discussion
There were clear ethnic inequalities in oral health behaviour among primary schoolchildren in England, Wales and Northern Ireland. Children of minority ethnic groups were less likely to start brushing during the first year of life, to brush their teeth twice or more daily, to have a first dental visit during the first year of life and to have a dental check-up in the past year than children of white ethnicity. Children of Asian ethnicity were at a particular disadvantage, as they were less likely to adhere to three of the four behaviours evaluated (that is, start brushing during the first year of life, brush twice or more daily and have a dental check-up in the past year) than children of white ethnicity. Children of Black ethnicity were less likely to have a dental check-up in the past year and children of other ethnicity were less likely to start brushing during the first year of life and to brush twice or more daily than children of white ethnicity.
The explanations for the disproportionately unfavourable behaviours seen among children of Asian ethnicity are unclear but their size demands additional investigation. These differences could be attributed to socioeconomic circumstances (discussed below), which also varied among ethnic groups. Moreover, access to dental services could be a significant barrier to access preventive advice and care. Because any child under the age of 18 years is eligible for free dental care in the UK, we need to look at factors beyond affordability. Some of these barriers might tap into availability (difficulty finding a dental practice taking new child patients), accessibility (difficulty reaching the dental practice's location), accommodation (difficulty to find and make convenient appointments, such as outside school or work hours to accompany the child, or use of translators to overcome linguistic barriers) and acceptability (patients' preferences). It must also be noted that this study found no differences in age at first dental visit between ethnic groups, which could be explained by the low percentage of children who visited the dentist in their first year of life in the sample (12.8%), suggesting a general lack of awareness for the need to attend dental services for a check-up.
Previous studies have shown that socioeconomic variables might explain oral health inequalities among Black and white ethnic groups.25,26 In this study, the two SES indicators used (education and NS-SEC) explained part, but not all, of the differences in child oral health behaviours by ethnicity. Inequalities in toothbrushing frequency between children of Asian and other ethnicity compared to children of white ethnicity, and inequalities in regular dental attendance between children of Black and white ethnicity, were fully attenuated after accounting for parental SES. In contrast, inequalities in the age when the child started brushing between children of Asian and other ethnicity compared to children of white ethnicity, and in regular dental attendance between children of Asian and white ethnicity, were only partially attenuated after accounting for parental SES. Minority ethnic groups were in lower SES than the white ethnic group in this sample. However, most of the ethnic inequalities in child oral health behaviours remained even after accounting for parental education and NS-SEC. These findings suggest that ethnic inequalities in child oral health behaviours are caused by other, more complex causes, and further study is required to identify these determinants, which may be a mix of environmental, cultural, biological and health-system-related factors.
The study findings reveal considerable ethnic inequalities in child oral health behaviours, which were reduced but not eliminated after accounting for family socioeconomic circumstances. These findings highlight the role of parents in setting up and maintaining health promoting behaviours in the family environment.31 Children are dependent on their parents for their health behaviours and access to dental services (acting as a caregiver).32 Parents perform an essential role in instilling favourable behaviours in their children as role models for their children.33 Future studies should look at the characteristics of the family environment that are conducive to the establishment of favourable parental and child oral health behaviours. Quantitative studies can confirm the present findings and expand on the list of child oral health behaviours investigated, whereas qualitative studies could help identify common features among families of different ethnic groups which can inform universal family interventions (that is, to increase early registration with the oral health care team for instance); features that are specific for families belonging to an minority ethnic group (that is, Asian ethnicity) can inform the design of targeted family interventions.
This study has some limitations. First is the cross-sectional nature of the data. Although we can eliminate the possibility that child behaviour influenced their ethnicity (reverse causation), causal explanations cannot be made. Secondly, the parental questionnaire had a low response rate, which could have introduced bias. However, survey weights were used to account for non-response bias. Third, despite using national survey data, several minority ethnic groups had few participants and were combined into a single category (labelled as other ethnicity) to produce reliable estimates. Using broad ethnic groups, such as children of Asian and Black ethnicity, masks some of the variability that exists within these groups (Indian, Pakistani, Bangladeshi, Black Caribbean, Black African, etc). It is also worth mentioning that the five ethnic groups used in the CDHS 2013 have been superseded by a comprehensive list of minority ethnic groups in more recent national surveys. Finally, child behaviours were indicated by parental reports, which might introduce measurement bias. Although it is conventional to use parents as proxies for their children health data in national surveys, validating some of these responses with medical records or even child reports would increase the credibility of the findings.
Conclusion
This study found ethnic inequalities in toothbrushing and dental visiting behaviour among primary schoolchildren in England, Wales and Northern Ireland. Accounting for parental socioeconomic status reduced but did not eliminate the observed differences by ethnicity.
References
Tinanoff N, Baez R J, Diaz Guillory C et al. Early childhood caries epidemiology, aetiology, risk assessment, societal burden, management, education, and policy: Global perspective. Int J Paediatr Dent 2019; 29: 238-248.
Bernabe E, Marcenes W, Hernandez C R et al. Global, Regional, and National Levels and Trends in Burden of Oral Conditions from 1990 to 2017: A Systematic Analysis for the Global Burden of Disease 2017 Study. J Dent Res 2020; 99: 362-373.
Sabbah W, Suominen A L, Vehkalahti M M, Aromaa A, Bernabé E. The role of behaviour in inequality in increments of dental caries among Finnish adults. Caries Res 2015; 49: 34-40.
Marinho V C, Higgins J P, Sheiham A, Logan S. Fluoride toothpastes for preventing dental caries in children and adolescents. Cochrane Database Syst Rev 2003; DOI: 10.1002/14651858.CD002278.
American Dental Association. Cleaning Your Child's Teeth. Available at https://www.mouthhealthy.org/all-topics-a-z/baby-teeth (accessed February 2023).
UK Government. Delivering better oral health: an evidence-based toolkit for prevention. 2021. Available at https://www.gov.uk/government/publications/delivering-better-oral-health-an-evidence-based-toolkit-for-prevention (accessed February 2023).
American Academy of Paediatric Dentistry. Frequently asked questions. Available at https://www.aapd.org/resources/parent/faq/ (accessed February 2023).
Davenport C F, Elley K M, Fry-Smith A, Taylor-Weetman C L, Taylor R S. The effectiveness of routine dental checks: a systematic review of the evidence base. Br Dent J 2003; 195: 87-98.
Patel S, Bay R C, Glick M. A systematic review of dental recall intervals and incidence of dental caries. J Am Dent Assoc 2010; 141: 527-539.
Clarkson J E, Pitts N B, Goulao B et al. Risk-based, 6-monthly and 24-monthly dental check-ups for adults: the INTERVAL three-arm RCT. Health Technol Assess 2020; 24: 1-138.
National Institute for Health and Care Excellence. Dental checks: intervals between oral health reviews - Clinical guidance G19. 2004. Available at https://www.nice.org.uk/guidance/cg19 (accessed February 2023).
NHS. Children's teeth. 2022. Available at https://www.nhs.uk/live-well/healthy-teeth-and-gums/taking-care-of-childrens-teeth/ (accessed September 2022).
British Society of Paediatric Dentistry. Dental check by one. Available at https://www.bspd.co.uk/patients/dental-check-by-one (accessed November 2022).
Blair M, Stewart-Brown S, Waterston T, Crowther R. Child Public Health. Oxford: Oxford University Press, 2010.
Schoon I. The well-being of children in the face of socio-economic deprivation and family instability. Revue des Politiques Sociales et Familiales 2019; 131: 189-202.
Parke R D, Leidy M S, Schofield T J et al. Socialization. In Haith M M, Benson J B (eds) Encyclopaedia of Infant and Early Childhood Development. pp 224-235. San Diego: Academic Press, 2008.
Komro K A, Flay B R, Biglan A, Promise Neighborhoods Research Consortium. Creating nurturing environments: a science-based framework for promoting child health and development within high-poverty neighborhoods. Clin Child Fam Psych 2011; 14: 111-134.
Bush N R, Wakschlag L S, LeWinn K Z et al. Family Environment, Neurodevelopmental Risk, and the Environmental Influences on Child Health Outcomes (ECHO) Initiative: Looking Back and Moving Forward. Front Psychiatry 2020; 11: 547.
Umaña-Taylor A J, Hill N E. Ethnic-Racial Socialization in the Family: A Decade's Advance on Precursors and Outcomes. J Marriage Fam 2020; 82: 244-271.
Wang Y, Benner A D, Boyle A E. Family cultural socialization in childhood: Navigating ethnic/racial diversity and numeric marginalization in school and neighborhood settings. Cultur Divers Ethnic Minor Psychol 2022; 28: 449-459.
Sun X, Bernabé E, Liu X, Gallagher J E, Zheng S. Early life factors and dental caries in 5-year-old children in China. J Dent 2017; 64: 73-79.
Ardenghi T M, Vargas-Ferreira F, Piovesan C, Mendes F M. Age of first dental visit and predictors for oral healthcare utilisation in preschool children. Oral Health Prev Dent 2012; 10: 17-27.
Isong I A, Soobader M J, Fisher-Owens S A et al. Racial disparity trends in children's dental visits: US National Health Interview Survey, 1964-2010. Paediatrics 2012; 130: 306-314.
Martin M, Pugach O, Avenetti D et al. Oral Health Behaviours in Very Young Children in Low-Income Urban Areas in Chicago, Illinois, 2018-2019. Prev Chronic Dis 2020; DOI: 10.5888/pcd17.200213.
Guarnizo-Herreño C C, Wehby G L. Explaining racial/ethnic disparities in children's dental health: a decomposition analysis. Am J Public Health 2012; 102: 859-866.
Fisher-Owens S A, Isong I A, Soobader M J et al. An examination of racial/ethnic disparities in children's oral health in the United States. J Public Health Dent 2013; 73: 166-174.
Rouxel P, Chandola T. Socioeconomic and ethnic inequalities in oral health among children and adolescents living in England, Wales and Northern Ireland. Community Dent Oral Epidemiol 2018; 46: 426-434.
Rodriguez-Alvarez E, Borrell L N, Marañon E, Lanborena N. Immigrant Status and Ethnic Inequities in Dental Caries in Children: Bilbao, Spain. Int J Environ Res Public Health 2022; 19: 4487.
Health and Social Care Information Centre. Children's Dental Health Survey 2013. Technical Report: England, Wales and Northern Ireland. 2015. Available at https://doc.ukdataservice.ac.uk/doc/7774/mrdoc/pdf/7774_cdhs_2013_technical_report.pdf (accessed February 2023).
Office for National Statistics. Ethnicity and National Identity in England and Wales: 2011. 2012. Available at https://www.ons.gov.uk/peoplepopulationandcommunity/culturalidentity/ethnicity/articles/ethnicityandnationalidentityinenglandandwales/2012-12-11 (accessed February 2023).
Michaelson V, Pilato K A, Davison C M. Family as a health promotion setting: A scoping review of conceptual models of the health-promoting family. PLoS One 2021; DOI: 10.1371/journal.pone.0249707.
Van Spreuwel P, Jerković-Ćosić K, van Loveren C, van der Heijden G J M G. Parents' Willingness to Invest in Primary Oral Health Prevention for Their Preschool Children. Int J Environ Res Public Health 2021; 18: 11437.
Nepaul P, Mahomed O. Influence of Parents' Oral Health Knowledge and Attitudes on Oral Health Practices of Children (5-12 Years) in a Rural School in KwaZulu-Natal, South Africa. J Int Soc Prev Community Dent 2020; 10: 605-612.
Author information
Authors and Affiliations
Contributions
Faisal M. F. bin Hayyan carried out data analysis and drafted the first version of the manuscript. Ellie Heidari and Eduardo Bernabé conceived the study, supervised the work and critically read the manuscript.
Corresponding author
Ethics declarations
The authors declare no conflicts of interest.
Rights and permissions
Open Access. This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0.© The Author(s) 2023
About this article

Cite this article
bin Hayyan, F., Heidari, E. & Bernabé, E. Ethnic inequalities in child oral health behaviours among five- and eight-year-old children from England, Wales and Northern Ireland. Br Dent J (2023). https://doi.org/10.1038/s41415-023-5577-3
Received:
Revised:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41415-023-5577-3
