
Abstract
There is a high prevalence of traumatic events in our society and the number of trauma sufferers in the general population is significant, with lasting adverse impacts on health, including oral health. Despite the high likelihood of oral health practitioners encountering patients with trauma, trauma history may not be disclosed or evident. In healthcare, trauma-informed care is a comprehensive and multi-level approach to patient care based on the understanding of the widespread nature and the impact of trauma. Trauma-informed care has not been widely implemented in oral health and multiple yet limited definitions of trauma could be further impeding implementation of trauma-informed care in oral health. To respond to these issues, we propose a definition of trauma in trauma-informed care which directly relates to the oral healthcare setting. We also propose a model – ‘Safe haven – a trauma-informed care model for oral health practitioners' – which aims to encourage oral health practitioners to practise trauma-informed care as a universal precaution for all patients in everyday practice.
Key points
-
Trauma-informed care in healthcare is a patient care approach to support patients with trauma.
-
A definition of trauma in trauma-informed care for oral health is proposed as a patient's personal response to experiencing distressing life events which has lasting adverse effects on all aspects of a patient's life, including oral health and access to oral healthcare.
-
‘Safe haven – a trauma-informed care model for oral health practitioners' is presented, enabling oral health practitioners to provide oral healthcare which is sensitive to trauma.
Similar content being viewed by others

Introduction
Trauma is common.1 Studies have found that 70–90% of the general population have experienced at least one traumatic life event, such as war, disasters and violence,2,3 and individuals can respond to the traumatic experience as trauma. While traumatic events were once considered as an extreme abnormality outside of usual life experiences,4 relatively common distressing life events can also be traumatic, for example, illness, bullying, loss of a loved one, family dysfunction, and medical treatments,5 including distressing dental treatments and dental trauma. The high prevalence of traumatic events in our society means anyone could be suffering trauma knowingly or unknowingly and may be impacted by its effect.
Trauma can have a profound impact on oral health and patients with trauma can present with various challenges in oral healthcare. Patients commonly suffer orofacial injuries from domestic violence6 and child abuse7 and oral health practitioners may be the first point of care for the injuries. In addition to the physical injuries, the patients in this situation may also be suffering trauma from experiencing the traumatic event(s). Patients with trauma have the tendency to avoid preventive treatments, with frequent rescheduled, missed and cancelled appointments in the oral health setting.8,9,10 Lying down under an authoritative figure, the smell of the latex and many other common settings in oral health can trigger flashbacks of past traumatic events, such as sexual abuse.10,11 Receiving treatment from a practitioner wearing a white coat, the use of sharp and metallic instruments and bright head lights have also been shown to provoke trauma reactions for some patients with trauma history.12,13 In addition to many challenging situations, physical closeness between the oral health practitioner and the patient, which is unavoidable in oral healthcare, has the potential to make the patient feel vulnerable and unsafe, triggering past traumatic memories and potentially re-traumatising the patient in the oral health setting. Patients with trauma have shown dental fear and anxiety, increased gagging,14,15,16,17 high rates of various co-morbid mental illnesses, and significant disruption in body systems with chronic inflammation,15,18,19,20 which can all compromise provision of optimal oral health services. Common trauma-coping strategies, such as smoking, substance use, and poor diet can result in long-term negative oral health consequences, such as periodontitis, dental caries and oral infections.8,21,22,23 Difficulty to trust and self-regulate in patients with trauma can also adversely affect the therapeutic relationship between the oral health practitioner and the patient, which can compromise the quality of care and the treatment outcome.24
Treating patients with trauma can also place practitioners at risk of secondary traumatic distress where the practitioners are indirectly affected by the impact of trauma with similar symptoms as patients with trauma. Secondary traumatic distress can lead to chronic fatigue, disturbing thoughts, poor concentration, emotional detachment, exhaustion, avoidance and physical illnesses, and practitioners may struggle to provide high-quality care, even leading to mental health issues and burnout,25,26,27 having lasting adverse psychological impact.
Trauma-informed care is an evidence-based approach to patient care which incorporates understanding of trauma into all practices, thus minimising the risk of harm and re-traumatisation while providing care.1 Trauma-informed care can also improve the health and wellbeing of practitioners by reducing the risk of secondary traumatic distress. Studies in emergency medicine,28 paediatrics29 and nursing11,30 have all shown a positive impact of trauma-informed care on both practitioners and patients with increased quality of care while treating patients with trauma. Despite its profound importance, trauma-informed care has not been widely implemented in oral health.31 This paper aims to raise awareness among oral health practitioners to the universality of trauma and describe approaches to patient care which can promote the wellbeing of patients with trauma and of practitioners treating patients with trauma.
Defining trauma for oral health
In oral health, the word ‘trauma' is commonly used for orofacial injuries. Among oral health practitioners, the term dental trauma is often used to describe the experience of past distressing dental treatments. In oral health, without broader understanding of trauma, trauma-informed care can be easily misinterpreted as treatment for orofacial injuries or caring for patients who have experience of past traumatic dental treatments. Trauma-informed care could also be considered as management of patients who have experienced specific traumatic events, such as domestic violence, or regarded as a mental health intervention for psychological trauma outside of the usual scope of oral health services. Such misunderstandings can diminish the awareness and implementation of trauma-informed care in oral health and lead to compromised care when treating patients with trauma.
Defining the word ‘trauma' could assist in better understanding trauma-informed care in oral health. Yet, there is no consensus on a common definition of trauma and its definition tends to be dependent upon the discipline which defines it. According to the American Psychiatric Association,32 trauma involves ‘actual or threatened death, serious injury, or sexual violence/violation'. In medicine, trauma can be defined as physical injuries,33 traumatic events/circumstances,34 or an individual's psychological response to events or injuries.35 In contemporary behavioural science, definition of trauma is limited as ‘an emotional response to a terrible event'.
According to the Substance Abuse and Mental Health Service Administration (SAMHSA),1 trauma can result from, ‘an event, series of events, or set of circumstances that is experienced by an individual as physically or emotionally harmful or life-threatening and that has lasting adverse effects on the individual's functioning and mental, physical, social, emotional, or spiritual wellbeing'.
While this most commonly accepted definition of trauma by SAMHSA is broader and more inclusive, it describes what trauma results from, not what trauma actually is. Such multiple and limited definitions of trauma can lead to confusion and compromise the understanding of trauma-informed care in oral health. To respond to the issue, we propose a definition of trauma in trauma-informed care for oral health which could, as a result, improve the understanding of trauma-informed care in oral health.
Table 1 defines ‘trauma' in trauma-informed care for oral health based on the three Es of trauma by SAMHSA,1 and the recognition that trauma is an integrated response of a whole person. For a clinical diagnosis of trauma, three Es of trauma are identified: traumatic Events, individual's Experience of the event as traumatic, and lasting adverse Effects of trauma. Trauma is a personalised experience of the event which is actual or threatened physical or psychological harm. Whether an individual interprets the experience as traumatic or not would depend on how the individual attributes meaning to, and how much they are physically and psychologically affected by, the event.1 How an individual experiences the event can also be influenced by a range of factors, such as cultural beliefs, life history, resilience, guilt, responsibility the individual imposes on the event, availability of social support, and the developmental stage.1,36,37 Trauma has lasting adverse impacts on all aspects of life, including mental, physical, social, emotional and spiritual wellbeing, and the effect can be immediate or delayed, with fear, anxiety, helplessness, horror, inability to cope with normal stress levels and difficulty in trusting others. Previously discussed oral health impacts of trauma are also summarised in Table 1.
The individual's experience of a traumatic event would be personal and internal.38 Characterising an abstract concept which cannot be measured or quantified presents inherent challenges and defining trauma is no exception. Its challenge stems from the subjective nature of human responses and diverse interpretation across individuals. With this in mind, a definition of trauma in trauma-informed care is proposed for oral health. For oral health, trauma in trauma-informed care is defined as a patient's personal response to experiencing distressing life events which has lasting adverse effects on all aspects of life. including oral health and access to oral healthcare.
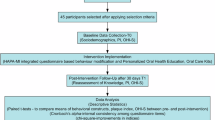
Many oral health practitioners work in solo or small practice settings with the most direct patient interactions compared to other support staff in the practice. While establishing trauma-informed care requires a multi-level approach of an organisation, trauma-informed care practices by the oral health practitioners at the clinician level would be an effective way to support patients with trauma and initiate implementation of trauma-informed care in oral health.
Figure 1 demonstrates an over-arching patient care approach to inform all interactions, decisions and treatments for oral health practitioners. The model features SAMHSA's four key competencies (the four Rs)1 of trauma-informed care: Realise the widespread impact of trauma; Recognise its signs and symptoms; Respond by trauma-informed care principles; and to Resist re-traumatisation. Trauma-informed care can protect everyone involved in the care from the adverse impacts of trauma and potential re-traumatisation.

Safe haven – trauma-informed care for oral health
Trauma-informed care practice by oral health practitioners begins by ‘Realising' that trauma is widespread and the impact of trauma is perverse. There is a high likelihood of oral health practitioners encountering patients with trauma and there is an increased awareness that everyone involved in the care may be affected by the impact of trauma, including the patient, their family members, the practitioner and other staff members, regardless of presence or absence of disclosure.9,39 Continuing education is an important and crucial element of trauma-informed care and common signs and symptoms of trauma should be learned and continually updated. However, challenging behaviours from patients with trauma may manifest in diverse and complex ways and it would be almost impossible to comprehend and interpret all the personal and individual signs and symptoms of trauma expressed by different patients. ‘Recognising' signs and symptoms of trauma in oral health means having an open and non-judgemental understanding that current behavioural challenges evident now may be a consequence of what has happened in the past. ‘Responding' means incorporating the principles of trauma-informed care – safety, trustworthiness, choice, collaboration and empowerment40 – into every aspect of care provided from the moment of first interaction. This means creating both a physically and psychologically safe and trusting environment by asking what can be done to make the patient more comfortable,9 informing the patient what will happen next,39 use of non-judgemental empathetic communication skills,41 asking for permission to touch or examine, and practising show-and-tell.9 Choice, collaboration and empowerment could be achieved by allowing additional appointment time to build rapport,42 or involving patients in the treatment planning process, where findings, options and recommendations are shared rather than imposed to provide a sense of control and ownership to build the patient's confidence.43 Addressing the practitioner's own history of trauma, discrimination and implicit biases are also very important in developing a non-judgemental outlook on patient behaviour and preventing re-traumatisation. ‘Resisting re-traumatisation' means for the practitioners to grow in awareness that any unexpected situations, for anyone in their care, can act as a trigger of past traumatic memories and has the potential to re-traumatise. Trauma-informed care requires active engagement by the oral health practitioner to resist harm by being committed to practising the principles of trauma-informed care throughout the entire encounter with the patient.
Infection control is practised in oral health for all patients as a universal precaution, regardless of the infection risk, history, or disclosure. This protects everyone involved in care from contagious and infectious diseases. Like infection control, trauma-informed care is recommended to be practised as a standard or universal precaution when treating all patients to create a sense of safety and to resist re-traumatisation. Just as there are patients with higher risk of infection and may require transmission-based precautions, patient populations with higher risk of trauma are also identified and more attention can be given to the need of trauma-informed care. While anyone is at risk of the exposure of traumatic events and trauma, patients with past traumatic dental treatments and patient populations suffering isolation and disadvantages, such as minority ethnic groups, women, children and young adults, refugees, First Nations people, and people in certain occupations, such as emergency service workers, are at higher risk of trauma, in ascending order, than the general population.2,44,45,46,47 Patients with physical injuries and disclosed trauma history have the highest risk of trauma. However, many patients do not feel the need to share their trauma history with oral health practitioners or are able to make connections between trauma and current challenges evident in oral healthcare.19 ‘Safe haven – a trauma-informed care model for oral health practitioners' acknowledges that trauma-informed care needs to be implemented for all patients, regardless of the risk, history or disclosure of trauma, to protect everyone from the impact of trauma, and aims to encourage oral health practitioners to practise trauma-informed care in everyday practice.
Concluding remarks
According to Stalker et al.,48 patients with a trauma history are more likely to experience oral healthcare positively when practitioners have an understanding of trauma and how it can affect their interactions. With the high prevalence of traumatic events in our society, trauma-informed care should be practised by all oral health practitioners with the assumption of underlying trauma in everyone involved in oral healthcare. However, much of the current understanding of trauma-informed care is based on its principles and values rather than specific recommendations to guide clinical practice.9,31,49 The definition of trauma in trauma-informed care for oral health, and ‘Safe haven – a trauma-informed care model for oral health practitioners' in this commentary, aim to guide the oral health community towards a better understanding of trauma and trauma-informed care. Understanding trauma and implementations of trauma-informed care by oral health practitioners could avoid unnecessary stress and challenges for practitioners and prevent re-traumatisation of patients, enabling oral health practitioners to better respond to the needs of the individual patient and improve the general quality of care in oral health.
References
Substance Abuse and Mental Health Services Administration. SAMHSA's Concept of Trauma and Guidance for a Trauma-Informed Approach. 2014. Available at https://www.health.ny.gov/health_care/medicaid/program/medicaid_health_homes/docs/samhsa_trauma_concept_paper.pdf (accessed 1 October 2025).
Benjet C, Bromet E, Karam E G et al. The epidemiology of traumatic event exposure worldwide: results from the World Mental Health Survey Consortium. Psychol Med 2016; 46: 327–343.
Kilpatrick D G, Resnick H S, Milanak M E, Miller M W, Keyes K M, Friedman M J. National estimates of exposure to traumatic events and PTSD prevalence using DSM-IV and DSM-5 criteria. J Trauma Stress 2013; 26: 537–547.
American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. Washington DC: American Psychiatric Association, 1980.
Birkeland M, Skar A, Jensen T. Do different traumatic events invoke different kinds of post-traumatic stress symptoms? Eur J Psychotraumatol 2021; 12: 1866399.
De Souza Cantão A B C, da Silva Lima T C, Fernandes M I A P, Nagendrababu V, Bastos J V, Levin L. Prevalence of dental, oral, and maxillofacial traumatic injuries among domestic violence victims: A systematic review and meta-analysis. Dent Traumatol 2024; 40: 33–42.
Leeners B, Stiller R, Block E, Görres G, Imthurn B, Rath W. Consequences of childhood sexual abuse experiences on dental care. J Psychosom Res 2007; 62: 581–588.
Ford K, Brocklehurst P, Hughes K, Sharp C A, Bellis M A. Understanding the association between self-reported poor oral health and exposure to adverse childhood experiences: a retrospective study. BMC Oral Health 2020; 20: 51.
Raja S, Hoersch M, Rajagopalan C F, Chang P. Treating patients with traumatic life experiences: providing trauma-informed care. J Am Dent Assoc 2014; 145: 238–245.
Raja S, Rajagopalan C F, Kruthoff M, Kuperschmidt A, Chang P, Hoersch M. Teaching dental students to interact with survivors of traumatic events: development of a two-day module. J Dent Educ 2015; 79: 47–55.
Reeves E. A synthesis of the literature on trauma-informed care. Issues Ment Health Nurs 2015; 36: 698–709.
Fredriksen T V, Søftestad S, Kranstad V, Willumsen T. Preparing for attack and recovering from battle: understanding child sexual abuse survivors' experiences of dental treatment. Community Dent Oral Epidemiol 2020; 48: 317–327.
Høyvik A C, Woldstad M I. Providing dental care to torture survivors. In Willumsen T, Lein J P Å, Gorter R C, Myran L (eds) Oral Health Psychology: Psychological Aspects Related to Dentistry. pp 275–283. Cham: Springer, 2022.
Folayan M O, El Tantawi M, Aly N M et al. Associations between a history of sexual abuse and dental anxiety, caries experience and oral hygiene status among adolescents in sub-urban South West Nigeria. BMC Oral Health 2021; 21: 196.
Nermo H, Willumsen T, Rognmo K, Thimm J C, Wang C E A, Johnsen J-A K. Dental anxiety and potentially traumatic events: a cross-sectional study based on the Tromsø Study – Tromsø 7. BMC Oral Health 2021; 21: 600.
Uziel N, Bronner G, Elran E, Eli I. Sexual correlates of gagging and dental anxiety. Community Dent Health 2012; 29: 243–247.
Willumsen T. Dental fear in sexually abused women. Eur J Oral Sci 2001; 109: 291–296.
Felitti V J, Anda R F, Nordenberg D et al. Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults. The Adverse Childhood Experiences (ACE) Study. Am J Prev Med 2019; 14: 245–258.
Phipps M, Molloy L, Visentin D. Prevalence of trauma in an Australian inner city mental health service consumer population. Community Ment Health J 2019; 55: 487–492.
Herrera-Escobar J P, Osman S Y, Das S et al. Long-term patient-reported outcomes and patient-reported outcome measures after injury: the National Trauma Research Action Plan (NTRAP) scoping review. J Trauma Acute Care Surg 2021; 90: 891–900.
Akinkugbe A A, Hood K B, Brickhouse T H. Exposure to adverse childhood experiences and oral health measures in adulthood: findings from the 2010 Behavioral Risk Factor Surveillance System. JDR Clin Transl Res 2019; 4: 116–125.
Sartori L R M, Pereira D H, Baker S R, Correa M B. Association between adverse childhood experiences and oral health in adulthood: a systematic scoping review. J Fam Violence 2023; 38: 1607–1624.
Simon A, Cage J, Akinkugbe A A. Adverse childhood experiences and oral health outcomes in US children and adolescents: A cross-sectional study of the 2016 national survey of children's health. Int J Environ Res Public Health 2021; 18: 12313.
Song Y, Luzzi L, Chrisopoulos S, Brennan D. Dentist-patient relationships and oral health impact in Australian adults. Community Dent Oral Epidemiol 2020; 48: 309–316.
Damian A J, Gallo J, Leaf P, Mendelson T. Organizational and provider level factors in implementation of trauma-informed care after a city-wide training: an explanatory mixed methods assessment. BMC Health Serv Res 2017; 17: 750.
McCann I L, Pearlman L A. Vicarious traumatization: a framework for understanding the psychological effects of working with victims. J Trauma Stress 1990; 3: 131–149.
Clark C, Classen C C, Fourt A, Shetty M. Treating the Trauma Survivor: An Essential Guide to Trauma-Informed Care. New York: Routledge, 2014.
Brown T, Ashworth H, Bass M et al. Trauma-informed care interventions in emergency medicine: a systematic review. West J Emerg Med 2022; 23: 334–344.
Marsac M L, Kassam-Adams N, Hildenbrand A K et al. Implementing a trauma-informed approach in pediatric health care networks. JAMA Pediatr 2016; 170: 70–77.
Kamsky H. Trauma-informed nursing practice. Online J Issues Nurs 2019; DOI: 10.3912/OJIN.Vol24No02Man03.
Mahood E, Shahid M, Gavin N, Rahmann A, Tadakamadla S K, Kroon J. Theories, models, frameworks, guidelines, and recommendations for trauma-informed oral healthcare services: a scoping review. Trauma Violence Abuse 2024; 25: 869–884.
American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5). 5th ed. Washington DC: American Psychiatric Publishing, 2013.
Coalition for National Trauma Research. CNTR Information. 2021. Available at https://www.east.org/content/documents/cntr_infopiece.pdf (accessed 1 October 2025).
Ervin K, Reid C, Podubinski T, Phillips J. Trauma-informed knowledge, awareness, practice, competence and confidence of rural health staff: a descriptive study. J Nurs Educ Pract 2021; DOI: 10.5430/jnep.v11n9p1.
Oral R, Coohey C, Zarei K et al. Nationwide efforts for trauma-informed care implementation and workforce development in healthcare and related fields: a systematic review. Turk J Pediatr 2020; 62: 906–920.
Anstorp T, Nupen Å, Willumsen, T. The importance of trauma-sensitive care. In Willumsen T, Lein J P Å, Gorter R C, Myran L (eds) Oral Health Psychology Textbooks in Contemporary Dentistry. pp 25–37. Cham: Springer, 2022.
Wilson C, Pence D M, Conradi L. Trauma-informed care. Encyclopedia Soc Work 2013; DOI: 10.1093/acrefore/9780199975839.013.1063.
Borghi A, Falcinelli I, Fini C, Gervasi A, Mazzuca C. How do we learn and why do we use abstract concepts and words. Front Young Minds 2023; DOI: 10.3389/frym.2023.1138574.
Swarthout K. Trauma-Informed Approach to Care in the Dental Setting. Dental Academy of Continuing Education, 2022.
Fallot R, Harris M. Creating Cultures of Trauma-Informed Care: A Self-Assessment and Planning Protocol. 2015. Available at https://children.wi.gov/Documents/CCTICSelf-AssessmentandPlanningProtocol0709.pdf (accessed 1 October 2025).
Heaton L J, Cheung H J. Trauma-Informed Care in Oral Health Care: the role of dental hygienists. J Dent Hyg 2024; 98: 50–55.
Blair A, Seeballuck C, McCann C, Heffernan A. Top tips: adult and child support and protection for the dental practice. Br Dent J 2024; 236: 235–239.
Magee J. A trauma-informed approach to dental care. J Massachusetts Dent Soc 2019; 68: 12–15.
Orygen. Trauma and young people: moving toward trauma-informed services and systems. 2018. Available at https://www.orygen.org.au/Orygen-Institute/Policy-Reports/Trauma-and-young-people-Moving-toward-trauma-info/Orygen_trauma_and_young_people_policy_report (accessed 1 October 2025).
Im H, Swan L E T. Working towards culturally responsive trauma-informed care in the refugee resettlement process: qualitative inquiry with refugee-serving professionals in the United States. Behav Sci 2021; 11: 155.
Nasir B F, Black E, Toombs M et al. Traumatic life events and risk of post-traumatic stress disorder among the Indigenous population of regional, remote and metropolitan Central-Eastern Australia: a cross-sectional study. BMJ Open 2021; DOI: 10.1136/bmjopen-2020-040875.
Australian Centre for Posttraumatic Mental Health. Australian Guidelines for the Treatment of Acute Stress Disorder and Posttraumatic Stress Disorder. 2013.
Stalker C A, Russell B D C, Teram E, Schachter C L. Providing dental care to survivors of childhood sexual abuse: treatment considerations for the practitioner. J Am Dent Assoc 2005; 136: 1277–1281.
Wolf E, Grinneby D, Nilsson P, Priebe G. Dental care of patients exposed to sexual abuse: Need for alliance between staff and patients. Eur J Oral Sci 2021; DOI: 10.1111/eos.12782.
Funding
University of Sydney Open Access funding enabled and organized by CAUL and its Member Institutions.
Author information
Authors and Affiliations
Contributions
WS conceived the paper and KSC drafted the initial and revised manuscripts. DL commented on and edited all the versions of the manuscripts and KSC, WS and DL have all agreed to submitting the paper for publication.
Corresponding author
Ethics declarations
The authors declare no conflicts of interest.
Rights and permissions
Open Access. This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0.© The Author(s) 2025.
About this article

Cite this article
Choi, K., Sohn, W. & Leadbeatter, D. Safe haven – a trauma-informed care model for oral health practitioners: a commentary. Br Dent J 239, 717–721 (2025). https://doi.org/10.1038/s41415-025-8862-5
Received:
Revised:
Accepted:
Published:
Version of record:
Issue date:
DOI: https://doi.org/10.1038/s41415-025-8862-5
