
Abstract
The non-homologous end joining (NHEJ) pathway is essential to repair DNA double-strand breaks. XRCC4 acts as a stabilizer of the DNA ligase LIG4 in the NHEJ process. In humans, XRCC4 pathogenic variants are responsible for a microcephalic primordial dwarfism syndrome (MPD). Currently, 17 patients have been reported with XRCC4-related MPD and we report 7 new patients from 6 different families, including one fetus. The patients present with short stature, severe microcephaly, neurodevelopmental disorder and additional features, such as transient increase in nuchal translucency, congenital glaucoma, thumb anomalies, hepatic steatosis, seizures, essential tremor and oligodontia which have not been previously described. Hyper- and hypopigmented skin macules, dermatofibrosarcoma, mandibular osteoid osteoma and pancytopenia are also new features, reminiscent of cancer susceptibility syndromes. Functional studies were performed on two patients carrying the known pathogenic p.(Trp43Arg) variant in homozygous state, using a fast, cost-effective and non-invasive approach on PBMCs: (1) Survival analyses after ionizing radiation confirm important radiosensitivity. (2) Flow cytometry showed the lack of TCR-Va7+ T-lymphocytes, suggesting recombination defect of V(D)J coding segments. (3) This was confirmed by multiplexed RT-PCR (PROMIDISα biomarker), analyzing the diversity of V(D)J coding segments in a subset of the TCRα repertoire. We therefore extend the phenotype of XRCC4-related MPD and suggest a combination of three functional assays, based on radiosensitivity and V(D)J recombination defect, to improve the interpretation of XRCC4 variants in fast, cost-effective and non-invasive manner. These findings will improve the diagnosis, genetic counselling, follow-up and management of these patients.
Similar content being viewed by others

Introduction
Double-strand breaks (DSB) of DNA, caused by radiation, chemical agents or replication accidents [1], can be repaired through two main systems. Ideally, the Homology Directed Repair (HDR) system, accurate and precise, acts when strands are close together, for example during the early stages of mitosis. Alternatively, but more frequently, the Non-Homologous End Joining (NHEJ) repair system, erratic and inaccurate, repairs DSB by direct DNA end joining when there is no homologous template nearby [2].
The NHEJ system operates as follows: free DNA ends are bound by the Ku70-Ku80 heterodimer, which recruits the DNA-dependant protein kinase DNAPK (encoded by the PRKDC gene) and the nuclease Artemis (encoded by the DCLRE1C gene). Artemis processes damaged DNA ends when required, then polymerases μ and λ synthesize new extremities. The final ligation is performed by the DNA ligase LIG4, stabilized by XLF, XRCC4 and its paralogue PAXX [2].
Of note, the NHEJ system is also involved in the immune system in a tissue-specialized manner, playing an essential role in the somatic recombination process of the variable (V), diversity (D), and joining (J) segments. These V(D)J coding gene segments undergo programmed double-strand cleavage at the recombination signal sites by RAG1 and RAG2. Then the NHEJ components introduce random deletions and insertions before final ligation by the XRCC4-XLF-LIG4 complex. This ensures the diversification of the T-cell receptor (TCR) and immunoglobulin repertoires in T and B lymphocytes, respectively [3].
The NHEJ system is therefore essential in adaptive immunity, in protection against ionizing stress and tumorigenesis. Moreover, descriptions of cognitive impairment in patients with pathogenic variations in PRKDC [4] and in the three genes of the NHEJ ligation complex, NHEJ1/XLF [5], LIG4 [6] and XRCC4 [7] also revealed an essential role for the NHEJ complex in neurodevelopment [8].
Shaheen et al. first reported a XRCC4 (MIM*194363) homozygous variants in a patient presenting with microcephalic primordial dwarfism (MPD; MIM#616541) [9]. Since then, 17 patients were reported in 12 different families [7, 9,10,11,12,13,14]. The patients show extreme growth failure and microcephaly, varying degrees of developmental delay ranging from normal cognition to severe intellectual disability, urogenital malformations, dilated cardiomyopathy and endocrine dysfunction including type 2 diabetes or glucose intolerance, dyslipidemia, hypergonadotropic hypogonadism, hypothyroidism and multinodular goiter. Craniofacial abnormalities include triangular face, sloping forehead, deep-set eyes, prominent beaked nose and pointed chin. Surprisingly for NHEJ deficiency, these patients do not present with obvious immune deficiency [15].
Here, we describe 7 new patients with additional clinical features expanding the phenotype of XRCC4-related microcephalic primordial dwarfism (XRCC4-related MPD), and propose a combination of three functional assays to reclassify variants of uncertain significance (VUS) in XRCC4, in a fast, cost-effective and non-invasive way.
Material and methods
Data collection
Two siblings were diagnosed with XRCC4-related MPD by exome sequencing (ES) in Lyon university medical center. A call for collaboration was made through the French network AnDDI-Rares (developmental abnormalities and malformative syndromes), and the European Rare disease network ERN-ITHACA. The aim was to collect clinical and molecular data from patients with XRCC4 pathogenic variants, in order to better describe and diagnose this rare syndrome. We collected clinical and molecular data on 7 new patients from 6 unrelated families. All families were evaluated by a clinical geneticist.
Genetic testing
Written consent for genetic testing was obtained for each patient. DNA was extracted from blood samples for all patients and their parents. ES and gene panel were performed following protocols described in Supplementary Data. Variant interpretation and classification were done according to American College of Medical Genetics guidelines. XRCC4 variants are annotated according to the NM_003401 reference transcript. The bi-parental inheritance of XRCC4 pathogenic variants was verified for each patient by Sanger sequencing in their parents, with the exception of P4 due to the unavailability of parental blood samples.
Functional studies
Three tests were carried out on PBMCs, isolated from heparinized blood of siblings P1 and P2, carrying the known pathogenic p.(Trp43Arg) variant in homozygous state [7], and of their healthy heterozygous parents. Given the small blood sample, functional tests were carried out once in each individual, with concordant results.
-
(i)
Cellular sensitivity to ionizing radiation. PBMCs were subjected to increasing doses of ionizing radiations. The test was performed in duplicate for each dose. After resting 4 h in complete culture medium (RPMI 10% FCS) to allow for DNA repair, T lymphocytes were activated with CD3/CD28 coated beads (Dynabeads) and cultured in the presence of IL2 (103 u/ml) in 48-well plates. After 6 days of culture, cells were recovered, washed, and counted through flow cytometry. The survival fraction represents the cell count of irradiated cells relative to untreated cells. Data were compared to the mean survival of PBMCs obtained from 17 healthy controls, 31 patients with ataxia telangiectasia carrying mutations in ATM, and 6 patients with DNA Lig4 mutations. The activation/proliferation of PBMC in the absence of irradiation was compared between the various samples and a healthy control (Supplementary Fig. 1).
-
(ii)
TCR-Vα7 dosage. After red cell lysis and wash, whole blood was incubated with a cocktail of fluorescently labelled antibodies as described previously [16]: APC-Cy7 anti-CD3, PE anti-TCR-Va7.2 (Sony), and PE-Vio770 anti-CD161 (Milteny). The proportion of CD3 + /CD161-/Vα7.2+ was determined by flow cytometry analysis. In this analysis, gating on CD161-/Va7.2 + T lymphocytes allows the exclusion of CD161+ clonal MAIT cells (Mucosal-Associated Invariant T-cells) which express an invariant TCR-Vα7 positive TCR, and the proportion of which can be highly variable depending on health status, causing a potential bias.
-
(iii)
PROMIDISα. The PROMIDISα signature was determined from whole PBMCs as previously described [16] and validated in several NHEJ-related disorders [17]. Briefly, RNA was purified from PBMC and reverse transcribed. A subset of TCR repertoire was then amplified by multiplex PCR using 8 forward Vα primers representing proximal (TRAV35, TRAV41), middle (TRAV20, TRAV21, TRAV23), and distal (TRAV1, TRAV5, TRAV10) Vα segments and a constant region (Cα) specific reverse primer. PCR products were further processed for NGS Illumina sequencing. TCR-Vα and Jα usage was assigned through IMGT/HighV-Quest [https://www.imgt.org/HighV-QUEST/home.action] [18] and quantified using custom R script. PROMIDISα signature was evaluated through hierarchical clustering using FactoMineR [19] against our in-house PROMIDISα database containing signatures for 24 healthy controls, 18 patients with various defects in V(D)J recombination and/or DNA repair (5 DCLRE1C, 3 LIG4, 4 Cernunnos/XLF, 2 PRKDC, 4 RAG1 patients), and 34 ataxia telangiectasia patients with ATM gene variants.
Results
Patients and families
We identified 7 new patients with XRCC4-related MPD, 4 males and 3 females from 6 different families, including one fetus. Clinical data are summarized in Table 1 and Fig. 1. Detailed medical history is provided for each patient in Supplementary Results and Table S1. Patients were aged from 14 WG to 22 years at last examination. All presented with pre- and postnatal growth retardation, microcephaly and intellectual disability when assessed. Genitourinary anomalies, glucose intolerance, dyslipidemia and hematological abnormalities were found in half of patients. Three patients had lymphopenia, which was progressive in one. Additional features are discussed below.

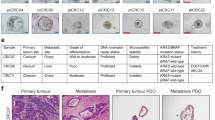
A, B P1 at 12 years 5 months. Note sloping forehead, deep set eyes, low-set, posteriorly rotated ears, beaked nose with sharp nasal root and broad tip, low columella with short philtrum, pointed chin giving a triangular face shape. C Dermatofibrosarcoma of the right foot in P1 at the age of 6, before surgical resection. D–F P2 at 11 years 3 months. Note facial dysmorphia similar to her brother P1 (D, E), broad thumbs with distal implantation (F). G P1 and P2 with their parents. H, I P3 at 4 years. Note the slightly beaked appearance of the nose, with a broad bulbous tip, and a thin upper lip. J–Q P4 at 6 months (J), 18 months (K), 3 years (M) and 22 years (L, N–Q). Note the hyper- and hypochromic macules (M, arrows), and the short broad appearance of the fingers (N, O), with a single left transverse palmar crease (O). On the feet, note partial syndactyly 2-3 with fourth/fifth brachymetatarsia (P). R–X P5 at 11 years and 3 months. Note the low posteriorly rotated ears with abnormal helix, a broad nose with bulbous and broad nasal tip with low columella, a short philtrum and a thin upper lip (R–T). Note also the presence of acanthosis nigricans on the neck (R) and the axilla (X). On the feet, a mild fourth/fifth brachymetatarsia is observed, with bilateral equinovarus (U, V) and nails deformities (W).
Genetic results
The patients in our series were diagnosed by ES (6/7) or NGS gene panel (1/7). Age at diagnosis was highly variable, ranging from the prenatal period at 15 WG (P7) to adulthood (P4). Biallelic pathogenic XRCC4 variants, presented in Fig. 2, were found at homozygous state in patients P1-2, and at compound heterozygous state in patients P3-7. Among the 7 different variants including 2 missenses [p.(Trp43 Arg); p.(Arg161Gln)], 1 frameshift [p.(His9ThrfsTer8)] and 4 nonsense variants [p.(Glu13Ter); p.(Arg205Ter); p.(Arg225Ter); p.(Arg275Ter)], only the p.(Glu13Ter) and p.(Arg205Ter) variants have not been previously reported.

The schematic view of XRCC4 exons (NM_003401) and the amino-acid numbering are based on PeCan Data of Proteinpaint.
Functional investigations
Functional investigations have been performed on extracted cells from blood samples of P1 and P2. Cellular sensitivity to increasing doses of ionizing radiations (IR), causing DNA breaks, was evaluated on blood derived primary T-lymphocytes. The T cell activation/proliferation of P1 and P2 was slightly (2-fold) reduced as compared to both parents and a healthy control (Supplementary Fig. 1). In contrast, as shown in Fig. 3A, T-cells from both patients showed an important decrease in proliferation upon IR (up to 2 log-fold reduction at 1.5 Gy) as compared with that of cells from 17 healthy controls (HC), attesting a major defect in the DNA damage response. The increased sensitivity of P1 and P2 was even stronger than that of several patients with mutations in either ATM or Lig4 genes. IR sensitivity of cells from both heterozygous parents were comparable to HC. The DNA repair defect of P1 and P2 translated in typical signatures using the two previously described TCR repertoire-based biomarkers [16]. First the proportion of CD3 + /CD161- non-MAIT T-lymphocytes expressing TCR-Vα7.2 was strongly reduced in both patients (0.27% and 0.43%, respectively) as compared to the normal values in both parents (1.64% and 2.64% respectively) (Fig. 3B). Moreover, after multiplexed PCR and NGS sequencing to analyze a subset of the TCRα repertoire, principal component analysis revealed a PROMIDISα signature typical of VDJ/DNA repair defective conditions for both patients, characterized by a bias in T-cell repertoire towards T-lymphocytes expressing proximal Vα and Jα segments (Fig. 3C). Both parents presented a PROMIDISα signature that clustered with the group of healthy controls.

A Cellular sensitivity of peripheral T lymphocytes to increasing doses of ionizing radiations in patient 1 (P1), patient 2 (P2) and parents. Mean IR sensitivity of cells from 17 healthy controls (Ctl), 6 patients with LIG4 mutations, and 31 patients with ATM mutations are included for comparison. B Quantification of CD161 negative T lymphocytes expressing TCR-Vα7.2 through flow cytometry. C Hierarchical clustering of PROMIDISα signatures by principal component analysis (PCA). VDJ: patients with VDJ/DNA repair deficiency (n = 18, including 5 DCLRE1C, 3 LIG4, 4 Cernunnos/XLF, 2 PRKDC, 4 RAG1), HC: Healthy controls (n = 24), AT: Ataxia telangiectasia patients (n = 34). P1 and P2: red arrows. Mother and father: green arrows.
Discussion
Clinical spectrum of XRCC4-related MPD
17 XRCC4-related MPD patients from 12 families were previously reported [7, 10,11,12,13,14] and we report here 7 new patients from 6 different families, including one fetal case, the first antenatal diagnosis reported to our knowledge. We performed a literature review of the phenotype and genotype of all patients previously described, and reported here (Tables 1 and S1). All patients had a proportionate IUGR, sometimes as early as the first trimester of pregnancy, followed by severe postnatal growth retardation and microcephaly. Their height ranged from −0.5 to −7.5 SD at birth with relative stability in the postnatal period (−1.8 to −7 SD). In contrast, their OFC at birth ranged from −1.83 to −4.83 SD, and the microcephaly progressively worsened in the postnatal period, to become the most affected parameter (−2.9 to −11 SD) (Fig. 4). Some patients present the classical facial features described in some type of MPD like Seckel-syndrome, with a triangular shaped face, a slopping forehead, low set ears, deep-set eyes, a prominent beaked nose, a low columella with short philtrum, and micrognathia (Fig. 1A–I). However, other patients do not present these characteristics (Fig. 1J–X). Facial features changed with age in P4, becoming thicker and coarser in adulthood (Fig. 1J–Q), reminiscent of patient published by Guo et al. [12]. Most patients have developmental delay, particularly affecting language, and cognitive impairment of variable severity. Neurological abnormalities are sometimes observed, mostly in adulthood, including sensory neuropathy, progressive cerebellar and pyramidal syndrome, muscle weakness, and cognitive deterioration. We report new neurological features, namely seizures in 1 patient and essential tremor in 2 patients. Sensory involvement is also observed, with visual impairment in some patients due to cataract, bilateral glaucoma, strabismus, astigmatism, or hyperopia—while hearing loss appears to be rare. We confirm that feeding difficulties during infancy can be part of the syndrome and can be severe: in our series, 3 patients had such symptoms, and all of them required gastrostomy. Cardiac and renal involvement appear to be rare. Dilated cardiomyopathy has been reported in 3 cases, 2 of adult onset [10], and one from 2 months of age leading to early death [14], which could illustrate the wide variability in the expression of this disease, although a second event cannot be excluded in the context of consanguinity. Variation in genital development seems to be frequent in males (cryptorchidism in almost half of patients and micropenis in 2 patients). Metabolic and endocrine abnormalities appear to be frequent, namely type 2 diabetes or prediabetes, hypothyroidism, hypergonadotropic hypogonadism, dyslipidemia including hypercholesterolemia and hypertriglyceridemia. Dyslipidemia was severe and rapidly worsened in our patient P4 between 19 and 21 years of age, requiring triple treatment to limit hepatic steatosis and avoid acute pancreatitis. Finally, cytopenias are reported in almost half of patients, including lymphopenia. Although subclinical abnormalities in blood count have already been reported [7, 10, 11, 13], P3 was the first patient with severe pancytopenia, from which she probably died. Our findings also include significant immunodeficiency in P1 and P2 despite normal or subnormal blood count before immunophenotyping (Table S2). While the amount of polynuclear cells, monocytes, CD8 + T-lymphocytes and NK-cells, seems normal, we show in both patients a significantly low rate of B-lymphocytes and CD4 + T-lymphocytes, predominantly in the naive subpopulation (CD4 + CD45RA + ), with a CD4+ count below 500 cells/μL, theoretically compatible with opportunistic infections [20]. In addition to tremors and convulsions, we report new features that have not been previously described, namely transient increase in nuchal translucency, congenital glaucoma, thumb anomalies, hypoplastic labia minora, oligodontia, hepatic steatosis, café-au-lait and hypochromic macules and defective thermoregulation with multiple hypothermic episodes (see detailed medical history in Supplemental Results).

For each patient newly or previously reported, weight, height and OFC are represented in standard deviations compared with WHO standards, at birth (blue spots) and at last evaluation (orange spots). It should be noted that while the IUGR is present in most patients, there is also a postnatal worsening in growth retardation, with a predominant impact on the OFC. The means are also represented by a slashed dot.
Tumor susceptibility
Only two patients in the literature have been reported with tumors [11, 12], and we report two other cases with new types of tumors. So, four types of tumor have been now reported in patients with XRCC4-related MPD, namely dermatofibrosarcoma, mandibular osteoid osteoma, thalamic glioma, and jejunal gastrointestinal stromal tumor (GIST), respectively at 5, 20, 19 and 30-years-old. These tumors seem more differentiated and with a lower malignant grade than those in other DNA repair deficiencies (i.e sarcoma, leukemia, lymphoma or adenocarcinoma) [21]. Dermatofibrosarcoma protuberans is a low-grade malignant tumor with aggressive local infiltration, usually diagnosed between 30 and 50-years-old [22], and rarely observed in children [23]. Its association with tumor predisposing disorders is not classic, but it has exceptionally been reported in Li-Fraumeni syndrome [24] and interestingly, Fanconi anemia [25]. Osteoid osteomas are benign tumors, common before 30-years-old [26]. However, localization in the mandible is observed in less than 1% of cases [27] and may suggest Gardner tumor predisposing syndrome [MIM#175100]. GIST represents less than 1% of all gastrointestinal tumors and only 10% originate in the jejunum. 10–30% progress to malignancy [28]. Rarely, these tumors are associated with germline variants in PDGFRA (MIM*173490), SDHB (MIM*185470), SDHC (MIM*602413), and KIT (MIM*164920). Finally, thalamic gliomas represent less than 1% of brain tumors [29] and may exceptionally be associated with tumor predisposition syndromes such as Li-Fraumeni [MIM#151623], type-1 neurofibromatosis [MIM#162200], or Constitutional Mismatch Repair Deficiency Syndrome impacting the DNA mismatch repair system [MIM:PS276300]. Thus, although these tumors do not appear to be classically associated with any known tumor predisposition syndromes, their rarity, their atypical location and early onset make the hypothesis of a chance association with XRCC4-related MPD unlikely. Pancytopenia in P3, increased chromosomal breakage under mitomycin-C, café-au-lait and hypopigmented macules in P4, also reinforce the hypothesis of a tumor susceptibility in these patients, reminiscent of other DNA repair disorders such as Fanconi anemia (see below). Importantly, although the types of tumor observed does not make it possible to suggest organ-specific monitoring at the present time, the radiosensitivity in these patients prompts us to formally recommend limiting exposure to radiation, particularly in the context of medical care, where a large number of x-ray images tends to be performed in the context of short stature. Likewise, should a tumor develop in XRCC4 patient, therapy must be extremely cautious to avoid the morbidity associated with the acute toxicity of genotoxic treatments, as previously documented in a LIG4 patient [30].
Differential diagnosis
The main differential diagnoses include other MPD, especially Seckel (MIM:PS210600), Majewski (MIM#210720) or Taybi-Linder syndromes (MIM#210710), due to severe growth retardation and overlapping facial features such as triangular face and prominent beaked nose. Like XRCC4, other DNA maintenance genes are involved in MPD, including ATR [MIM*601215], TRAIP [MIM*605958], RBBP8 [MIM*604124], RECQL3 [MIM*604610], NBN [MIM*602667], DDX11 [MIM*601150], ERCC6 [MIM*609413], ERCC8 [MIM*609412], and LIG4 [MIM*601837]. Other disorders involving the NHEJ system also can be considered as differential diagnoses, since pathogenic variations impacting PRKDC [MIM*600899], NHEJ1 [MIM*611290], and LIG4 [MIM*601837] can manifest as MPD with neurodevelopmental disorder, but in these syndromes, severe combined immunodeficiency (SCID) is at the forefront, in contrast to XRCC4-related MPD. More rarely, Fanconi anaemia can also manifest as MPD [9], suggesting a phenotypic continuum within these syndromes.
Other DNA repair deficiencies may also be reminiscent of XRCC4-related MPD owing to cancer susceptibility, cytopenia, hyper/hypopigmented macules, radial/thumb anomalies, neurodegenerescence and endocrine dysfunction. Indeed, tumors and cytopenia observed in some XRCC4 patients also remind cancer susceptibility in LIG4 deficiency [31], Fanconi anemia [MIM:PS227650], Ataxia-Teleangiectasia [MIM#208900], and more broadly, genomic instability syndromes such as Mosaic Variegated Aneuploidy [PS257300]. The co-occurrence of hypochromic and café-au-lait spots as described in P4 also reminds Fanconi anaemia, Bloom, or Nijmegen syndromes [32]. Likewise, radial/thumb anomalies observed in P2 are also reminiscent of Fanconi anaemia [MIM:PS227650] and ATR-related Seckel syndrome [MIM#210600], more rarely observed in LIG4-related MPD [31], Nijmegen [33] and Bloom syndromes [34]. Neurodegenerescence, reported in two adults with XRCC4-related MPD [10], and suspected in P1 based on progressive pyramidal signs and tremor, is a main feature in Ataxia-Teleangiectasia [MIM#208900], well-reported in Cockayne [MIM#133540, MIM#216400] and Nijmegen syndromes [MIM#251260]. Endocrine dysfunction, well reported in XRCC4-related MPD, is also observed in other DNA repair defects, including DNA2, BLM, NSMCE2-related MPD [MIM#615807, MIM#210900, MIM#617253], but also in other MPD such as Majewski syndrome [35]. Finally, the abnormal mitomycin-C chromosome breakage test observed on P4 also reinforces the overlap with Fanconi anaemia.
XRCC4 pathogenic variants
In our series, the p.(Glu13Ter) and p.(Arg205Ter) variants (in P6 and P7 respectively) were not previously reported, but some variants appear to be recurrent (Fig. 2). The p.(His9ThrfsTer8) variant, in particular, was found in 9 patients from 8 different families. It is present in the heterozygous state 673 times in the control database gnomAD (v4.1.0), including 624 European individuals, strongly suggesting a founder effect. Likewise, the p.(Arg225Ter) and p.(Arg275Ter) variants are each found in 5 different families and are present respectively 32 and 10 times in the heterozygous state in European population. The p.(Trp43Arg) variant, homozygous in 4 patients from 3 families, is present 11 times in gnomAD, in the heterozygous state, exclusively in the South Asian population. This suggests a founder effect in this population, given that our patients P1 and P2 are known to originate from Georgia. No variant in our series is present in the homozygous state in gnomAD (v4.1.0).
Of the 24 patients now reported, 11 carry pathogenic variants in the homozygous state and 13 in the compound heterozygous state. The 13 different variants now reported are mainly truncating variants (8/13; nonsense or frameshift) but also missense (3/13) and splicing variants (2/13). Of note, no genotype-phenotype correlation emerges from these data, and patients with biallelic truncating variants in XRCC4 do not appear to have a more severe phenotype (P4,5,6). Missense variants also have a loss-of-function effect, with aberrant splicing and synthesis of a truncated protein (p.Asp82Glu [11]; p.Arg161Gln [13]), or a reduction in protein stability (p.Trp43Arg) [7]. Likewise, the c.-10-1G > T variant induces aberrant splicing, leading to a major reduction in XRCC4 protein level, even with a transcript that remains detectable [7]. These results all point to a biallelic loss-of-function of XRCC4 as a common pathomechanism.
Pathomechanisms
Most MPDs are caused by cell cycle abnormalities in progenitor cells, at early stages of embryogenesis [36]. Several MPDs are due to DNA repair defects, which represent an indirect mechanism of “Cell Cycle-opathies”, causing early apoptosis and cell cycle arrest [37]. Interestingly, residual LIG4 ligase activity remains detectable in XRCC4 patients [7], and could explain viability in humans but not in complete KO mice [38]. Unlike XRCC4-patients, true biallelic KOs are less likely in patients with LIG4 deficiency, as this gene consists of a single coding exon. It is likely that truncating variations result in a truncated protein rather than mRNA degradation by NMD, explaining why a continuum of severity correlated with the position of the truncating variants is observed in LIG4 deficiency [31]. LIG4 is therefore partially destabilized by XRCC4 deficiency, but it has recently been shown that other factors (PAXX, ATM) may play a compensatory role in the stabilizing function of LIG4 in mice [39], and other XRCC4 paralogs (including PAXX, XLF) could have the same role in humans [40]. It has been previously noted that XRCC4-patients have usually no clinical immunodeficiency, unlike in the other syndromes affecting the NHEJ system [15]. However, and as reported in some patients [7, 10, 11], we found quantitative abnormalities of B- and T-lymphocytes in P1 and P2, subclinical but possibly progressive. In contrast, XRCC4 deficient mice showed a marked defective lymphogenesis with hypotrophic thymi, B and T-cell development arrest in early stages [38]. LIG4 residual activity in humans could provide a sufficient level of V(D)J coding segments recombination in B and T lymphocytes to ensure maturation of these immune cells despite subclinical defects in the diversity of immune repertoires [41]. Thus, the residual activity of LIG4 in context of complete XRCC4 deficiency could explain viability and the absence of clinical immunodeficiency in humans, due to a sufficient level of V(D)J recombination to maintain the diversity of the immune repertoire, but with MPD due to a lack of DSB repair in progenitor cells, leading to cycle cell arrest during embryogenesis.
Functional investigations: towards standardized tests to reclassify VUS in XRCC4
Ionizing radiation is the main cause of DSBs [1], and patients with NHEJ defects logically presents an elevated cellular radiosensitivity, as demonstrated in vitro in XRCC4 patients’ skin derived fibroblasts [7, 10, 12, 13, 40, 42]. Instead of skin fibroblasts, we reproduced these results for P1 and P2, carrying the known pathogenic p.(Trp43 Arg) variant in homozygous state [7, 9], with a survival assay on peripheral T lymphocytes, exposed to increasing doses of ionizing radiations (Fig. 3A). Moreover, although patients with biallelic pathogenic variants in XRCC4 appear to be immunocompetent, 3/6 patients of our series show biological immune abnormalities, and subclinical but significant abnormalities in the diversification of the immune repertoire have been demonstrated previously, such as reduced competence for V(D)J recombination [7]. We reproduced this observation in P1 and P2 with new techniques: using flow cytometry, we showed that the proportion of TCR-Va7 expressing T-cells is decreased in non-MAIT T-lymphocytes (Fig. 3B), while multiplexed PCR and sequencing of coding segments (PROMIDISα) revealed a signature compatible with patients suffering from other V(D)J recombination defect (Fig. 3C). Together, these results corroborate a V(D)J recombination defect in XRCC4-patients. It is still not clear whether these anomalies have a clinical significance, but they could represent a useful biomarker for diagnosis. Indeed, while XRCC4 loss-of-function variants are straightforward to interpret, new missense or splicing variants will require proof of their effect. The combination of these three tests demonstrating increased radiosensitivity and impaired V(D)J recombination will be of great help in reclassifying VUS. In particular, this PBMC-based approach has the significant advantage of rapid response (7 days), and is therefore less expensive than studies on fibroblasts which require several weeks of culture. This approach is also more acceptable, as a single blood sampling is required, without the need for invasive sampling such as skin biopsies.
Conclusion
We present here clinical and molecular data for 7 new patients with XRCC4-related MPD, including the first antenatal diagnosis reported to our knowledge. This work extends the phenotype with novel features including transient increase in nuchal translucency, congenital glaucoma, oligodontia, hepatic steatosis, seizures, essential tremor, thumb abnormalities, café-au-lait and hypochromic macules, dermatofibrosarcoma, mandibular osteoid osteoma, and pancytopenia. We provide new evidence supporting tumor susceptibility in these patients, radiosensitivity, and subclinical but significant immune abnormalities. We recommend that these patients be carefully monitored for psychomotor development and nutrition in childhood, with screening for renal, sensory and urogenital abnormalities and neurological, endocrinological, cardiac and hematological monitoring adapted to the clinical and biological signs. Biological monitoring of blood count, glycaemia, liver and renal function tests, lipid and thyroid screening should be performed regularly, as well as immunophenotyping at less frequent intervals. We recommend avoiding exposure to ionising radiation in the context of medical care, and recommend special precautions regarding the use of genotoxic treatments in these patients. We also propose the combination of three PBMC-based functional assays, highlighting radiosensitivity and V(D)J recombination defect as a result of the NHEJ system impairment, that could contribute to the diagnosis of patients with VUS in XRCC4, using a fast, cost-effective and non-invasive approach. Together, these data will contribute to adapt the diagnosis, genetic counselling, follow-up and management of these patients.
Data availability
The data that support the findings of this study are available upon request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions. The newly identified p.(Glu13Ter) and p.(Arg205Ter) variants have been added as pathogenic in the ClinVar database (RCV004798185.1 and RCV004798186.1, respectively).
References
Mehta A, Haber JE. Sources of DNA Double-Strand Breaks and Models of Recombinational DNA Repair. Cold Spring Harb Perspect Biol. 2014;6:a016428.
Scully R, Panday A, Elango R, Willis NA. DNA double-strand break repair-pathway choice in somatic mammalian cells. Nat Rev Mol Cell Biol. 2019;20:698–714.
Jung D, Alt FW. Unraveling V(D)J Recombination: Insights into Gene Regulation. Cell 2004 ;116:299–311.
Woodbine L, Neal JA, Sasi NK, Shimada M, Deem K, Coleman H, et al. PRKDC mutations in a SCID patient with profound neurological abnormalities. J Clin Investig. 2013;123:2969–80.
Buck D, Malivert L, De Chasseval R, Barraud A, Fondanèche MC, Sanal O, et al. Cernunnos, a Novel Nonhomologous End-Joining Factor, Is Mutated in Human Immunodeficiency with Microcephaly. Cell 2006;124:287–99.
O’Driscoll M, Cerosaletti KM, Girard PM, Dai Y, Stumm M, Kysela B, et al. DNA Ligase IV Mutations Identified in Patients Exhibiting Developmental Delay and Immunodeficiency. Mol Cell. 2001;8:1175–85.
Murray JE, van der Burg M, IJspeert H, Carroll P, Wu Q, Ochi T, et al. Mutations in the NHEJ Component XRCC4 Cause Primordial Dwarfism. Am J Hum Genet. 2015;96:412–24.
Alt FW, Schwer B. DNA double-strand breaks as drivers of neural genomic change, function, and disease. DNA Repair. 2018;71:158–63.
Shaheen R, Faqeih E, Ansari S, Abdel-Salam G, Al-Hassnan ZN, Al-Shidi T, et al. Genomic analysis of primordial dwarfism reveals novel disease genes. Genome Res. 2014;24:291–9.
Bee L, Nasca A, Zanolini A, Cendron F, d’Adamo P, Costa R, et al. A nonsense mutation of human XRCC4 is associated with adult-onset progressive encephalocardiomyopathy. EMBO Mol Med. 2015;7:918–29.
de Bruin C, Mericq V, Andrew SF, van Duyvenvoorde HA, Verkaik NS, Losekoot M, et al. An XRCC4 Splice Mutation Associated With Severe Short Stature, Gonadal Failure, and Early-Onset Metabolic Syndrome. J Clin Endocrinol Metab. 2015;100:E789–98.
Guo C, Nakazawa Y, Woodbine L, Björkman A, Shimada M, Fawcett H, et al. XRCC4 deficiency in human subjects causes a marked neurological phenotype but no overt immunodeficiency. J Allergy Clin Immunol. 2015;136:1007–17.
Rosin N, Elcioglu NH, Beleggia F, Isguven P, Altmuller J, Thiele H, et al. Mutations in XRCC4 cause primary microcephaly, short stature and increased genomic instability. Hum Mol Genet. 2015;24:3708–17.
Fredette ME, Lombardi KC, Duker AL, Buck CO, Phornphutkul C, Bober MB, et al. Novel XRCC4 Mutations in an Infant With Microcephalic Primordial Dwarfism, Dilated Cardiomyopathy, Subclinical Hypothyroidism, and Early Death: Expanding the Phenotype Of XRCC4 Mutations. AACE. Clin Case Rep. 2020;6:e1–4.
Villartay J. When natural mutants do not fit our expectations: the intriguing case of patients with XRCC 4 mutations revealed by whole‐exome sequencing. EMBO Mol Med. 2015;7:862–4.
Berland A, Rosain J, Kaltenbach S, Allain V, Mahlaoui N, Melki I, et al. PROMIDISα: A T-cell receptor α signature associated with immunodeficiencies caused by V(D)J recombination defects. J Allergy Clin Immunol. 2019;143:325–334.e2.
Fournier B, Mahlaoui N, Moshous D, de Villartay JP. Inborn errors of immunity caused by defects in the DNA damage response pathways: Importance of minimizing treatment-related genotoxicity. Pediatr Allergy Immunol. 2022;33:e13820.
Li S, Lefranc MP, Miles JJ, Alamyar E, Giudicelli V, Duroux P, et al. IMGT/HighV QUEST paradigm for T cell receptor IMGT clonotype diversity and next generation repertoire immunoprofiling. Nat Commun. 2013;4:2333.
Lê S, Josse J, Husson F. FactoMineR: An R Package for Multivariate Analysis. J Stat Softw. 2008;25:1–18.
Vergis EN, Mellors JW. Natural history of HIV-1 infection. Infect Dis Clin North Am. 2000;14:809–25.
Garutti M, Foffano L, Mazzeo R, Michelotti A, Da Ros L, Viel A, et al. Hereditary Cancer Syndromes: A Comprehensive Review with a Visual Tool. Genes 2023;14:1025.
Shah KK, McHugh JB, Folpe AL, Patel RM. Dermatofibrosarcoma Protuberans of Distal Extremities and Acral Sites: A Clinicopathologic Analysis of 27 Cases. Am J Surg Pathol. 2018;42:413.
Tsai YJ, Lin PY, Chew KY, Chiang YC. Dermatofibrosarcoma protuberans in children and adolescents: Clinical presentation, histology, treatment, and review of the literature. J Plast Reconstr Aesthet Surg. 2014;67:1222–9.
Ku I, Park JU. Dermatofibrosarcoma in Li–Fraumeni syndrome with early-onset multiple primary tumors. J Dermatol. 2020;47:e333–5.
Lee DW, Yang JH, Won CH, Chang SE, Lee MW, Choi JH, et al. A Case of Congenital Pigmented Dermatofibrosarcoma Protuberans (Bednar Tumor) in a Patient with Fanconi Anemia. Pediatr Dermatol. 2011;28:583–5.
Tepelenis K, Skandalakis GP, Papathanakos G, Alexandra Kefala M, Kitsouli A, Barbouti A, et al. Osteoid Osteoma: An Updated Review of Epidemiology, Pathogenesis, Clinical Presentation, Radiological Features, and Treatment Option. Vivo. 2021;35:1929–38.
Singh A, Solomon MC. Osteoid osteoma of the mandible: A case report with review of the literature. J Dent Sci. 2017;12:185–9.
Sankey RE, Maatouk M, Mahmood A, Raja M. Case Report: Jejunal gastrointestinal stromal tumour, a rare tumour, with a challenging diagnosis and a successful treatment. J Surg Case Rep. 2015;2015:rjv050.
Gupta A, Shaller N, McFadden KA. Pediatric Thalamic Gliomas: An Updated Review. Arch Pathol Lab Med. 2017;141:1316–23.
Plowman PN, Bridges BA, Arlett CF, Hinney A, Kingston JE. An instance of clinical radiation morbidity and cellular radiosensitivity, not associated with ataxia-telangiectasia. Br J Radiol. 1990;63:624–8.
Murray JE, Bicknell LS, Yigit G, Duker AL, van Kogelenberg M, Haghayegh S, et al. Extreme Growth Failure is a Common Presentation of Ligase IV Deficiency. Hum Mutat. 2014;35:76–85.
Taylor AMR, Rothblum-Oviatt C, Ellis NA, Hickson ID, Meyer S, Crawford TO, et al. Chromosome instability syndromes. Nat Rev Dis Primer. 2019;5:1–20.
Chrzanowska KH, Stumm M, Bekiesińska-Figatowska M, Varon R, Białecka M, Gregorek H, et al. Atypical clinical picture of the Nijmegen breakage syndrome associated with developmental abnormalities of the brain. J Med Genet. 2001;38:e3.
Langer K, Cunniff CM, Kucine N Bloom Syndrome. In: GeneReviews® [Internet] [Internet]. University of Washington, Seattle; 2023 [cited 2024 Nov 22]. https://www.ncbi.nlm.nih.gov/sites/books/NBK1398/.
Huang-Doran I, Bicknell LS, Finucane FM, Rocha N, Porter KM, Tung YCL, et al. Genetic Defects in Human Pericentrin Are Associated With Severe Insulin Resistance and Diabetes. Diabetes 2011;60:925–35.
Phan TP, Holland AJ. Time is of the essence: the molecular mechanisms of primary microcephaly. Genes Dev. 2021;35:1551–78.
Sadoughi F, Hallajzadeh J, Asemi Z, Mansournia MA, Alemi F, Yousefi B. Signaling pathways involved in cell cycle arrest during the DNA breaks. DNA Repair. 2021;98:103047.
Gao Y, Sun Y, Frank KM, Dikkes P, Fujiwara Y, Seidl KJ, et al. A Critical Role for DNA End-Joining Proteins in Both Lymphogenesis and Neurogenesis. Cell 1998;95:891–902.
Roch B, Abramowski V, Etienne O, Musilli S, David P, Charbonnier JB, et al. An XRCC4 mutant mouse, a model for human X4 syndrome, reveals interplays with Xlf, PAXX, and ATM in lymphoid development. eLife 2021;10:e69353.
Ruis B, Molan A, Takasugi T, Hendrickson EA. Absence of XRCC4 and its paralogs in human cells reveal differences in outcomes for DNA repair and V(D)J recombination. DNA Repair. 2020;85:102738.
de Villartay JP, Fischer A, Durandy A. The mechanisms of immune diversification and their disorders. Nat Rev Immunol. 2003;3:962–72.
Asa ADDC, Wanotayan R, Sharma MK, Tsukada K, Shimada M, Matsumoto Y. Functional analysis of XRCC4 mutations in reported microcephaly and growth defect patients in terms of radiosensitivity. J Radiat Res (Tokyo). 2021;62:380–9.
Acknowledgements
The authors are sincerely grateful to the families for participating in this study. We would also like to thank Dr Marianne Till and Dr Valérie Bonadona for their expertise in cytogenetics and oncopaediatrics, respectively, Marion Delous and Sylvie Mazoyer for their suggestions during the course of this work, the AnDDi-Rares collaborative platform and the European Reference Network on Rare Congenital Malformations and Rare Intellectual Disability ERN-ITHACA for having allowed the calls for collaboration within the framework of this manuscript. Several authors of this publication are members of the ERN-ITHACA [EU Framework Partnership Agreement ID: 3HP-HP-FPA ERN-01-2016/739516]. ERN-ITHACA is funded by the European Union, under the grant agreement N°101156387. Sequencing of patient 6 was supported by the Neurological Foundation of New Zealand, awarded to LSB.
Funding
This work was carried out within the framework of Lyon University Hospital activity with additional funding for Open Access publication. Funding bodies did not have any influence on study design, results, and data interpretation or final manuscript.
Author information
Authors and Affiliations
Contributions
Silvestre Cuinat and Audrey Putoux designed the study and wrote the manuscript. Nicolas Chatron, Gaetan Lesca, Silke Kaulfuß, Gökhan Yigit and Bernd Wollnik performed the genetic studies. Audrey Putoux, Florence Petit, Marion Aubert Mucca, Eric Bieth, Harald Rieder, Ariane Schmetz, Colina McKeown and Tim Savage performed the clinical examinations and were involved in the follow-up of the families. Jean-Pierre de Villartay and Etienne Dincuff performed the functional investigations. Patrick Edery made substantial contributions to conception of the study. All authors discussed the results and commented on the manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics declaration
According to the principles outlined in the Helsinki Declaration, written consent for genetic testing was obtained for all the parents of the patients included in this study. Genetic tests were all performed in the context of diagnosis and care in each university medical center. Additional written consents for the publication of photographs were obtained for patients 1, 2, 3, 4, 5. Specific written consent for functional studies were obtained for patients 1, 2.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Cuinat, S., Chatron, N., Petit, F. et al. XRCC4-related microcephalic primordial dwarfism: description of a clinical series of 7 cases, phenotype expansion and new diagnostic approaches. Eur J Hum Genet 33, 842–851 (2025). https://doi.org/10.1038/s41431-025-01821-0
Received:
Revised:
Accepted:
Published:
Issue date:
DOI: https://doi.org/10.1038/s41431-025-01821-0
This article is cited by
-
Summer reading 2025 in EJHG
European Journal of Human Genetics (2025)
