
Abstract
Continuous kinematic biofeedback during exercise interventions can lead to improved therapeutic outcomes in hand and wrist rehabilitation. Conventional methods for measuring joint kinematics typically allow only static measurements performed by specially trained therapists. This paper introduces skin-conformal, wearable wireless systems designed to continuously and accurately capture the angles of target joints, specifically in hand and wrist. Supported by a computer vision-based calibration protocol run on a smart device, these magnetometer-based standalone systems provide patients and clinicians with continuous, real-time data on joint angles and ranges of motion through an intuitive graphical interface. Human trials in healthy volunteers demonstrate the accuracy and precision of the electrogoniometry system, as well as its compatibility with simulated hand therapy. We have also demonstrated the electrogoniometry system is suitable for tracking complex and rapid movements and for deployment during occupational tasks where it could serve as a biofeedback device to warn against excessive and clinically contraindicated motion.
Similar content being viewed by others

Introduction
Impairment in the upper extremity, including the arm, forearm, wrist, and hand, can significantly reduce independence in activities of daily living as well as quality of life1,2,3, while also incurring substantial financial costs4. Although the causes of such impairments vary—ranging from stroke5 to spinal injury6 and trauma7,8—ensuring optimal recovery through proper rehabilitation is crucial; inadequate rehabilitation can lead to impaired recovery, often resulting in a permanent loss of range of motion (ROM) and motor skills9,10,11. However, fewer than 55% of patients typically comply with their rehabilitation programs12,13, missing the critical window for optimal recovery. Biofeedback that incorporates quantitative measurements of joint kinematics has proven to be a valuable tool for both patients and clinicians during rehabilitation, as it provides real-time biological information that would otherwise be inaccessible14. This real-time data can enhance therapeutic outcomes by helping patients participate more effectively with their rehabilitation protocols, in both the supervised and unsupervised settings15.
In nearly all traumatic conditions of the hand, injury and treatment are associated with joint stiffness and lost range of motion. Rehabilitation from the injured state, as such, is highly focused upon the restoration of maximal ROM. Clinical assessment of ROM is a fundamental parameter used to evaluate joint movement functionality, mobility, and rehabilitation progress. Standard approaches to measuring hand ROM encompass visual estimation, goniometry, composite finger flexion to the distal palmar crease, torque range of motion, and wiregrams16. The most ubiquitous tool in clinical hand therapy is the hand-held analog goniometer. The accuracy and precision of this tool is inconsistent, and depends not only upon the type of goniometer used, but also upon the expertise of the therapist making the measurement17,18,19. Additionally, traditional goniometry provides only static measurements and continuous data cannot be gathered. This means that feedback is only offered at the beginning and end of a supervised therapy session, and no feedback is available during active exercise, or between sessions during execution of a home exercise program (HEP).
Existing strategies for continuous measurement of hand and wrist ROM that are both technically advanced and clinically sound include computer vision20,21,22,23, wearable sensors utilizing strain or bending sensors24,25,26,27 and magnetometers28,29, wrist motion sensing using electromyography30,31 or pressure sensor32, and inertial measurement units33,34. These advanced approaches, however, face practical challenges which limit adoption. These include occlusions and restricted workspace; the need for large training datasets; limited capabilities offering only gesture recognition rather than precise angle measurement; reliance on tethered systems with bulky benchtop electronics; the need for additional calibration equipment; and significant computational power requirements. A comparison of various technologies that can measure joint angles is presented in Supplementary Table 1, highlighting key characteristics such as sensor, targeted modality, uncertainty, calibration methods, connection type, and computing and data processing platform. These characteristics may serve as criteria for evaluating the feasibility of deploying these technologies in both in-clinic and at-home rehabilitation settings, where compatibility with current rehabilitation protocols is particularly important for enhancing therapeutic outcomes35.
The ability to continuously track joint angles in hand and wrist using a wireless, wearable system that conforms to the surroundings of a target joint would address such challenges in ROM biofeedback for rehabilitation. Reliable and instant reporting of this kinematic biofeedback to clinicians and patients, whether in-clinic or at-home physical therapy settings, benefits both parties and may enhance rehabilitation outcomes. This paper introduces wireless, wearable electrogoniometry systems that provide continuous, real-time measurements of joint angles in hand and wrist, displayed through a graphical user interface (GUI) on a smart device. The unique design of the device, equipped with optimized data flow, facilitates seamless integration of computer vision with a magnetometer, effectively overcoming obstacles commonly encountered in wearable goniometers, such as the need for motion capture systems for per-use calibration, being tethered to benchtop electronics, and significant computational power. Importantly, the calibration methodology developed in this work formulates the relationship between local orientation of a magnet and target joint angles in a simple polynomial function, thereby avoiding iterative solvers, machine learning, or kinematic modeling typically required in magnet-based tracking of hand motions (see Supplementary Table 2). Additionally, this methodology customizes the calibration function for each use, enabling the electrogoniometry system to be highly adaptable across trials and users. Once calibrated, the system relies solely on magnetometer data, thus addressing typical limitation of vision-based system, such as occlusions and restricted workspace. Results from physical simulations and comparisons with two different ground truth methods—3D marker tracking under a multi-camera setup and 2D markerless tracking from fluoroscopy videos—demonstrate the favorable characteristics of the proposed systems, including high accuracy and precision (error <5°) which is clinically acceptable. Human trials in ten healthy volunteers confirm that these systems perform well in the setting of clinically relevant hand therapy exercises. The wearable devices are operated using only a standard smart device, and requires no additional equipment for calibration. Furthermore, experiments with vigorous activities and daily tasks over the long term (7 hours) highlight the potential of the systems for applications beyond the primary clinical use.
Results
Soft, wireless electrogoniometry systems for monitoring human joint range of motions
Figure 1 illustrates soft, wireless electrogoniometry systems capable of continuous monitoring of the joints in the fingers or wrists. The discrete design, soft mechanical properties, and wireless operational capabilities facilitate ergonomic wear without mechanically loading or constraining natural motions of targeted joints, a common issue with alternatives that use strain gauges. Figure 1a, b illustrates mounting on a user, with configurations for measuring the proximal interphalangeal (PIP) or wrist joints, respectively. The finger goniometer (FG) features a strap band with a pin-and-hole design, allowing users to wear the device without the need for adhesives or additional straps (Fig. 1a), essential for many post-surgical patients. For the wrist goniometer (WG), a pin and a hole (Fig. 1b) allow two separate segments to be connected or disconnected as needed. The pin and hole also serve as a fiducial to facilitate initial positioning of the device on the wrist while the two segments are connected. Similar to the fulcrum of an analog goniometer used in standard clinical practice36, this fiducial, placed over the capitate on the dorsal aspect of the wrist joint, ensures proper alignment of the magnet and magnetometer. The magnet is positioned on the dorsal aspect of the hand along the third metacarpal, while the magnetometer is placed on the distal forearm, aligning with the dorsal midline of the forearm.

Exploded-view schematic illustrations (top) of the finger goniometer (a) and the wrist goniometer (b). Photographs (bottom-left) show the devices and their placement on the targeted joints (bottom-right). c A graphical user interface on a smart device that supports vision-based calibration and captures angles and the range of angular motions in real-time during a trial. d Measurement configuration for monitoring proximal interphalangeal joint motions of the left index finger, illustrated with an actual user.
The schematic illustrations in Fig. 1a, b highlight additional features of the two segments of the FG and WG, both encapsulated in a soft silicone enclosure. A thin, flexible printed circuit board (fPCB) and a 3.7-V lithium polymer battery (45 mAh; dimensions: 15 mm length, 12 mm width, and 4 mm thickness) encased in medical-grade silicone shells (thickness: 0.5 mm; Silbione RTV 4420, Elkem), form one segment. The other includes a stack of four rectangular neodymium magnets (grade N50; dimensions: 6 mm length, 3 mm width, and 2 mm thickness). These magnets form a cuboid structure with a height of 3 mm, to produce a strong magnetic field in a low-profile design. Two different architectures in these segments define distinct electrogoniometry systems, the FG and WG, each tailored to different joints. Detailed dimensions and other information can be found in Supplementary Fig. 1.
The enclosures function not only to isolate the electronics from the environment but also to facilitate joint angle measurements using embedded fiducial markers (i.e., ArUco marker37). As shown in Fig. 1a, b, patterns of silicone with white and black dye define ArUco markers with high contrast, ensuring the accuracy and reliability of joint angle measurements using computer vision for purposes of calibration with a smart device (iPhone 12 Pro, Apple Inc.). The fPCBs (Fig. 1a, b; Supplementary Fig. 1) support and interconnect a collection of electronic components, including a magnetometer (MLX90393, Melexis), a power management integrated circuit (PMIC) with a wireless charging coil, and a Bluetooth Low Energy (BLE) system on a chip (SoC; ISP-1807, Insight SIP). This system provides digital measurements of magnetic field strength along three axes. Along with the PMIC, a foldable charging coil (Supplementary Fig. 1) facilitates wireless charging using near-field communication standards. The magnetometer protrudes from the main fPCB body to align with an ArUco marker. For the FG, the magnetometer connects to the main body by a serpentine wire that bypasses the non-targeting joint. This design reduces the sensitivity of the goniometer to motions of non-targeted joints and allows the main body to be placed on the back of the hand.
Figure 1c illustrates a real-time GUI that displays quantitative information on joint angles at 25-ms intervals, sufficiently fast to capture natural kinematics of the finger and wrist. Data communication between the smart device and the BLE SoC utilizes standard BLE protocols, ensuring smooth transmission of magnetometer data along with their timestamps. Along with real-time data, the GUI estimates and continuously updates minimum and maximum angles during use, to show the range of motion. Moreover, the GUI, integrated with the Open Source Computer Vision Library (OpenCV), accurately measures joint angles by tracking ArUco markers with the camera of the smart device. This information serves to calibrate the magnetometer responses to joint motions. These systems can be used in both clinical and home settings, as illustrated in Fig. 1d. Details are in Supplementary Movies 1–3.
An initial calibration with computer vision and routine use
Figure 2a illustrates the procedures for calibration and subsequent routine use. The former utilizes angles determined from the computer vision system and the magnetometer, while the latter relies only on magnetometer data. The magnetometer transmits changes in magnetic field strengths along each of three axes (\({B}_{i}\), where \(i=x,\,y,\) and \(z\)) in a 3D Cartesian coordinate system to the BLE SoC at 30 Hz using the Inter-Integrated Circuit (I2C) protocol. These \({B}_{i}\) values facilitate the calculation of relative angles of the magnet cuboid to the magnetometer by using two \({B}_{i}\) on a targeting plane, as shown in Fig. 2b, c. For example, flexion/extension (flex/ext) motions occur in the \({yz}\)-plane, and the angle resulting from these spatial motions can be defined as \({\phi }_{f}={{{\rm{atan}}}}({B}_{z}/{B}_{y})\). Similarly, \({B}_{x}\) and \({B}_{y}\) on the \({xy}\)-plane determine the angle from radial/ulnar (rad/uln) motions as \({\phi }_{r}={{{\rm{atan}}}}({B}_{x}/{B}_{y})\).

a Functional flow chart of the system, showing initial data collection for magnetometer response calibration and routine use with calibrated magnetometer responses. During calibration, ground truth angles (θ) are collected through the vision system. Orientation vectors (u, ν, and w) of two markers are used to estimate angles from (b) flexion/extension and (c) radial/ulnar motions. Subscripts, d, p, f, and r, denote distal, proximal, flexion/extension, and radial/ulnar, respectively. Symbols θ and ϕ represent joint angles and magnet angles, respectively. d A captured image of the screen of a smart device while marker tracking is active. The accuracy and range of measured angles with respect to four different camera angles are displayed in (e) and (f). Boxes in (f) simply denote the range (i.e., the minimum and maximum values) for each camera angle, whereas in (e), they represent the interquartile range (IQR) from the 25th to the 75th percentiles. Whiskers extend to 1.5 times the IQR. The midline within each box indicates the median of the dataset. g Algorithm flow chart for the calibration, detailing the use of extrapolation to address the limited range of measured angles resulting from camera angles. An \({{{{\boldsymbol{R}}}}}^{{{{\boldsymbol{2}}}}}\) value obtained from curve fitting indicates the goodness of fit and serves as a criterion for either passing or failing the calibration step.
Even though \(\phi\) changes along with changes in joint angles (\(\theta\)), \(\phi\) cannot directly represent \(\theta\) because the center of rotation for \(\phi\) is at the magnetometer, whereas the joint itself serves as the center of rotation for \(\theta\). The initial calibration step effectively addresses this limitation by establishing a relationship between \(\theta\) and \(\phi\) as a function of \(\phi\). The computer vision system with ArUco marker provides estimates of \(\theta\) during the calibration step. Utilizing the embedded camera with OpenCV library and SceneKit in a custom app, the smart device tracks the positions and orientations of the two ArUco markers at 60 frames per second (fps). Similar to the orient-x-based method presented in a previous study21, orientation vectors of the markers on distal and proximal segments facilitate joint angle estimations for each motion. For instance, \({\theta }_{f}\) for flex\ext motions can be expressed as shown in Fig. 2b:
where the subscripts \(d\) and \(p\) represent distal and proximal, respectively. For rad/uln motions, \(x\)-axial orientation vectors (\({u}_{p}\) and \({u}_{d}\)) and a z-axial orientation vector at the proximal (\({w}_{p}\)) can yield estimates for \({\theta }_{r}\):
Motions of targeted joints can be modeled as one degree-of-freedom (DOF) rotations. As such, this strategy based on axial orientation vectors effectively estimates joint motions.
Figure 2d shows the screen of a smart device tracking Aruco markers from a specific camera angle. Orientation indicators on the markers inform the user about the status of the marker tracking. As illustrated in Fig. 2e, absolute errors between measured angles and applied angles from a motorized stage (Supplementary Fig. 2) are less than 0.9° across four camera angles for both flex/ext and rad/uln motions. Under these quasi-static conditions, the computer vision system accurately measures angles with errors less than 1.2° within a 95% confidence interval (Supplementary Figs. 3, 5, and 7). Along with this high accuracy in angle measurements under quasi-static loads, root mean squared errors (RMSEs) of less than 2.3° for measured angles compared to applied cyclic loadings (Supplementary Figs. 4, 6, and 8) further confirm the ability of the computer vision system to serve as ground truth for calibrating magnetometer responses to joint motions.
Figure 2g details this initial calibration, followed by routine use. A smart device simultaneously collects angles from the computer vision system (\(\theta\)) and the magnetometer (\(\phi\)), synchronizing these data to accommodate their asynchronous sampling. After collecting over 100 samples of both \(\theta\) and \(\phi\), the device implements two types of curve fitting—interpolation for rad/uln motions and extrapolation for flex/ext motions—using the MPFIT library38. As Fig. 2f illustrates, a single camera can capture the full range of rad/uln angles, thus making interpolation suitable for data from this motion. Flex/ext angles, however, exceed the capture range of a single camera angle, thus necessitating extrapolation to reconstruct the full range of motion from the limited calibration data.
In the Extrapolation block of Fig. 2g, three steps mitigate intrinsic uncertainty in this process. Initially, the sampled ϕ and \({\theta }\) are examined using 120 reference functions, \(\theta=f(\phi )\). These functions, obtained from experiments that explore possible locations of the magnet cuboid and magnetometer (Supplementary Fig. 9), have \({R}^{2}\) values close to 0.99 and encompass the expected ROM of the hand digit PIP, IP, and wrist joint, as reported in previous studies (Supplementary Tables 3 and 4). The RMSE of \(\theta\) to outputs from these functions allows selection of two functions with the minimum RMSE, and their coefficients establish an initial guess and boundaries for curve fitting. The FG employs extrapolation curve fitting, while the WG utilizes both interpolation and extrapolation, depending on the types of motion. The \({R}^{2}\) value from the curve fitting determines whether to proceed with the routine use or to recalibrate. Once the fitted function meets the criterion (\({R}^{2} \, > \, 0.95\)), the system estimates joint angles using magnetometer data and the fitted function, as shown in the Routine use block in Fig. 2g. Details on this calibration procedure and its implementation in the GUI are in Supplementary Fig. 10.
Responses of the electrogoniometry systems under benchtop experimental conditions
Figure 3 illustrates the responses of the electrogoniometry systems under a benchtop experimental setup (Supplementary Fig. 2). These experiments evaluate the effect of the range of calibration data on extrapolation accuracy, and the accuracy and repeatability of measurements. As demonstrated in Fig. 3a, the FG effectively responds to low-rate angular loads (17.6°/s) across the expected full range of motion of the PIP and IP joint (from −18° to 110°) using only a 20° range of calibration input (from 10° to 30°). A low RMSE (1.3°) of the angles measured by the FG confirms its high measurement accuracy (Supplementary Fig. 11a). Additionally, the FG shows highly repeatable responses to cyclic loadings with a higher average rate (from -9.9° to 72° at 64.2°/s), where the RMSE to ground truth is 1.6° (Supplementary Fig. 11a). Moreover, RMSEs of less than 2.9° in measurements with increased ranges of calibration data (30° and 40°; Supplementary Fig. 12) suggest that responses of the FG are minimally sensitive to the range within the test window.

Device calibration with extrapolation (left), responses to the expected full range of joint motions (center), and responses to cyclic loadings (right) in the electrogoniometry systems for capturing flexion/extension of the fingers (a) and wrists (b). c Responses of the electrogoniometer for wrist radial/ulnar motions, including device calibration with interpolation (left), response to the expected full range of motion (center), and response to cyclic loading (right). The shaded areas in blue in the left panels indicate the range of calibration data.
Figure 3b shows that the WG measures flex/ext angles with high accuracy and precision under similar experimental conditions. Similar to the FG, the WG demonstrates low RMSEs to ground truth ( < 2°) under angular loads across the expected full range of motion ( ± 74.7° at 17.6°/s) and cycles ( ± 49.4° at 71.4°/s), regardless of the range of calibration data (Supplementary Fig. 13). Figure 3c depicts rad/uln angles measured using the WG. The responses of the WG to rad/uln motions (full motion: ±51.3° at 17.6°/s; cycle: ±27.9° at 46.1°/s) exhibit improved accuracy and repeatability, likely due to an improved fitted function achieved through interpolation. The results from both flex/ext and rad/uln loads indicate that the WG can measure both types of motion with high precision, and that the ranges of calibration data also minimally affect its performance within the test window, similar to the FG.
The RMSEs tend to increase along with larger ranges of motion and higher angular load rates. This trend does not, however, stem from defects in the electrogoniometry systems but rather from limitations in the error analysis performed in this study. Errors between two asynchronously sampled time-series data sets can be quantified by first resampling the data from the ground truth (60 Hz) to match the lower sampling rate of the device (25 Hz). This resampling, along with potential time mismatches, leads to higher errors under more dynamic conditions. Outliers in absolute errors observed during transitions, as depicted in Supplementary Figs. 11, 12, and 13, corroborate this trend. The remaining sections utilize this error analysis method to quantify discrepancies between the angles measured by the systems and the ground truth.
Besides the extrapolation performance and measurement accuracy and precision, the benchtop experimental setup also characterizes key aspects of the FG and WG as sensing systems. The FG exhibits an overall sensitivity of 2.3° joint angle/1° magnet angle across three different distances between the magnet and magnetometer (Supplement Fig. 14). Notably, misalignment between the magnet and magnetometer has a negligible effect on device responses, as shown in Supplementary Fig. 15. Supplementary Fig. 16 illustrates the highly repeatable responses of the FG, both within trials of an individual FG and across FGs of different ages. Additionally, all three FGs demonstrate resolutions close to 1° degrees. Sensitivities of the WG to angular motions, as shown in Supplementary Figs. 17 and 18, are 3.8° and -4.2° joint angle/1o magnet angle for the flex/ext and rad/ulnar motions, respectively, across three different distances. The resolution is less than 2° in both motions.
Drift is another important aspect of a sensing system. With negligible drift over 45 min, the FG captures angular motions (−14° to 51°) sequentially applied at three angular speeds (ω1 ≈ 55°/s; ω2 ≈ 75°/s; ω3 ≈ 125°/s), as shown in Supplementary Fig. 19a–d. The FG also demonstrates stable responses under temperature variations (23.5 °C to 40 °C), a common cause of drift in magnetometers, with drift limited to only 1.3% of the full span (Supplementary Fig. 19e, f). In addition, hysteresis in the FG is negligible, as depicted in Supplementary Fig. 20.
Sensing hand digit PIP and IP joint and wrist joint motions
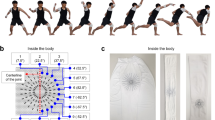
Targeted joint motions captured by the electrogoniometry systems involve complex 3D movements but can be assumed to consist of a single DOF rotation. Ground truth data for purposes of validation uses 3D marker tracking with improved 3D reconstruction and pose estimation, utilizing Pose 3D and DeepLabCut (DLC)39. This approach not only provides detailed motion paths but also significantly reduces the ambiguity in movement interpretation by precisely quantifying the angles and trajectories involved.
Figure 4 illustrates the use of four fiducial markers for this purpose. Two markers on each segment represent the proximal and middle (or distal) phalanges of the hand and the carpal and forearm bones of the wrist. The marker tracking process precisely captures and reconstructs the positions of these markers in 3D space from videos recorded by four time-synchronized, high-speed cameras, each operating at 60 fps (Supplementary Fig. 21a,b; Supplementary Movie 4). The estimated positions (P1, P2, P3, and P4 in Fig. 4) facilitate the measurement of angles using two vectors: \(\theta \,={\cos }^{-1}(({{{\bf{a}}}}\cdot {{{\bf{b}}}})/(\left|{{{\bf{a}}}}\right|\left|{{{\bf{b}}}}\right|))\), where the vectors, \({{{\bf{a}}}}\) and \({{{\bf{b}}}}\), represent vectors from the positions, \({{{\bf{P}}}}{{{\bf{2}}}}-{{{\bf{P}}}}{{{\bf{1}}}}\) and \({{{\bf{P}}}}{{{\bf{4}}}}-{{{\bf{P}}}}{{{\bf{3}}}}\), respectively. An overall RMSE of 0.9° within the range of 15° to 75° (Supplementary Fig. 21c,d) confirms that angles measured in this manner are sufficiently accurate to serve as ground truth.

Still shots from high-speed videos captured during experiments (left), positions of markers tracked in 3D space (center), and joint angles estimated by 3D marker tracking alongside device measurements (right) during flexion/extension motions of the fingers (a, b) and wrist (c), as well as radial/ulnar motions of the wrist (d).
Figure 4a, b demonstrates the responses of the FG to spatial motions of the thumb and index finger. On the thumb, the FG accurately captures motions of the IP joint, ranging from -13.1° (hyperextension) to 60.7° (full flexion), closely aligning with the range of the ground truth, spanning from −11.8° to 59.7°. Despite the limitations in error analysis, an RMSE of 2.2° (Supplementary Fig. 22a) confirms a high degree of agreement between the ground truth and the responses of the FG. The FG also measures rotational angles of the PIP joint in the index finger, exhibiting its typical range of motion, from -6.9° (hyperextension) to 88.9° (full flexion), with an RMSE of 1.9° (Supplementary Fig. 22b), indicating strong agreement with the ground truth (from -11° to 90.2°; Fig. 4b). The full flexion angles observed in both hand digits are marginally lower than the documented ranges (Supplementary Table S3), likely due to interference from the strap bands of the FG. In addition, the tendency of the FG to slightly underestimate hyperextension may result from the mildly degraded performance of the extrapolation under this more practical setup. While the RMSE tends to decrease with increasing independence of finger movement40, the little finger shows the highest error (3.4o), likely due to its smaller size that limits optimal placement of the FG despite having relatively high independence compared to the middle and ring fingers. Further details on the measurements for the rest of the fingers are available in Supplementary Fig. 23. Given the anatomical differences between the thumb and fingers, the experimental results validate that the FG effectively captures flex/ext motions of the PIP and IP joints in hand digits.
The enhanced 3D marker tracking also facilitates a detailed assessment of the performance of the WG in measuring both flex/ext and rad/uln motions of the wrist. For flex/ext motions, the range captured by the WG extends from −57.8° to 48.8°, closely matching the range of the ground truth from −59.6° to 47.7°, as shown in Fig. 4c. An RMSE of 3.6° (Supplementary Fig. 22c) indicates good agreement between these two data sets. Figure 4d illustrates responses of the WG to rad/uln motions with measurements ranging from −35.1° to 3.5°, demonstrating strong agreement with the ground truth (from −35.2° to 4°), further supported by a lower RMSE of 1.3° (Supplementary Fig. 22d). These improved results likely follow from the reduced range of rad/uln motions compared to flex/ext motions and the use of interpolation in measuring these motions.
In addition to the experiments on the FG and WG under the free motion condition, both goniometry systems demonstrate their responsiveness to simulated patient conditions, including restricted movements and artificial tremors comparable to human tremors (3 Hz to 12 Hz41). Supplementary Figs 24 and 26a,b illustrate the responses of the FG and WG to restricted motion, showing even lower RMSEs (FG: 0.3o; WG (flex/ext): 0.6o; WG (rad/uln): 0.4o) compared to those observed under the free motion condition, likely due to the reduced range of movement. Furthermore, the FG exhibits stable responses under artificial tremor (Supplementary Fig. 25), suggesting that the goniometry systems are capable of reliably monitoring angular motions of patients with high accuracy and precision.
Sensing finger PIP joint motions during simulated supervised hand therapy
As verified by the full 3D marker tracking, the FG can effectively monitor PIP and IP joint motions under practical settings, with high precision. Demonstrating the efficacy of the FG in clinical and therapeutic contexts, however, is a fundamental step in assessing its usability and reliability as a biomedical wearable. This technical validation includes exploring three data collection protocols with healthy volunteers as subjects in physical therapy settings. The first protocol focuses on comparing PIP joint angles in index fingers measured by the FG to those from clinical ground truth. Data for this comparison came from five healthy volunteers (Supplementary Table 5) wearing the device on either their left or right index finger while executing flex/ext motions under the supervision of a hand surgeon, as shown in Supplementary Fig. 27a. Figure 5a illustrates markerless tracking performed on videos recorded by a mini C-arm fluoroscopy (Fluoroscan InSight FD, Hologic Inc.) at 30 fps during the experiments. Similar to the full 3D marker tracking, DLC facilitates angle estimations using vectors obtained from this 2D markerless tracking by recognizing and tracking four points in 2D space—the head and base of the middle phalanx and the head and center of the proximal phalanx (Supplementary Movie 5). As shown in Fig. 5b, linear fitting functions with slopes close to 1, along with Pearson correlation coefficient (r value) exceeding 0.99, confirm strong agreement between angles from these two measurements. Figure 5c further corroborates this finding in graphs that show deviations of less than ±5° between these two measurements within a 95% confidence interval. Importantly, this range of accuracy, within an error margin of 5°, is considered acceptable for goniometric measurement of finger joints42.

a Two overlaid still shots from a fluoroscopic video taken during experiments. Tracking points are to estimate ground truth angles of the proximal interphalangeal joint (PIP) in the index finger. b Comparison of ground truth angles from five healthy volunteers with those measured by the device. c Bland-Altman plot assessing the agreement between the two sets of readings. d Comparison of PIP joint angles in the index, middle, and small fingers of the right and left hands of ten healthy volunteers, measured by a hand therapist using a digital goniometer, versus those measured by the device. e Bland-Altman plot illustrating the agreement between the two measurement methods. f Photographs of three types of tendon glide exercises, accompanied by time-series data of PIP joint angles in index finger collected during the exercises.
The general practice in hand therapy sessions involves assessing the range of motion of a joint using a handheld goniometer. The second protocol, therefore, aims to compare the responses of the FG to this general practice to determine the clinical relevance of the device. Supplementary Fig. 27b illustrates the PIP joint angles of the index, middle, and small fingers on both hands of ten healthy volunteers, measured by an occupational therapist using a digital goniometer (82311-200 P, GemRed; ±0.3° accuracy). The data shown in Fig. 5d arise from the same rater, to eliminate inter-rater variations16. Details on the session and volunteers are in Supplementary Fig. 27b and Table 5. As with the results of the first study, slopes close to 1 in linear fitting functions and r values of 0.98 demonstrate strong accordance of the FG with the general practice. These two methods, however, show almost twice the deviation (−10.9° to 9.9° within a 95% confidence interval) compared to the first study, as depicted in Fig. 5e. Along with the estimated errors in the FG from the first study, human errors may contribute. Notably, increased errors for small fingers, as illustrated in Supplementary Fig. 28, reflect human errors, typically related to the design of the digital goniometer18, which is unfavorable for small fingers (Supplementary Fig. 27b). Nonetheless, this level of error remains within a reasonable range, considering the combined error from defects in the FG (5°) and human error (8°) totals 9.4°.
The third protocol demonstrates the compatibility of the FG with active ROM exercises that patients routinely perform during supervised hand therapy sessions and the HEP. The FG can provide patients with continuous feedback during such exercises, which is not possible with conventional measurement techniques. Use of the FG in hand therapy sessions could thus offer significant benefits in a therapeutic context. Figure 5f and Supplementary Movie 6 illustrate responses of the FG during three specific active ROM gliding exercises: straight fist, hook fist, and reverse blocking. The device provides continuous feedback to a healthy volunteer (Supplementary Table 5) while conducting these exercises, demonstrating compatibility with standard rehabilitation practices. The data illustrated in Fig. 5f show similar ranges of motion for the straight fist (-1.1° to 92.5°) and hook fist (-0.8° to 97.8°), while the reverse block shows a distinct range of motion (9.6° to 80°) from those two. These ranges remain within the reported range of motion for the finger PIP joints (Supplementary Table 3). This unique function in offering real-time angle feedback to users could significantly enhance therapeutic outcomes, as previous studies show that such feedback can motivate users and help them track progress33. This real-time feedback, particularly in variations noted in exercises like the reverse block, suggests that applications of the FG could help to fine-tune therapy protocols to maximize patient recovery based on immediate biomechanical responses.
Sensing finger PIP joint motions during activities
Monitoring the kinematics of a targeted finger joint during occupational activities adds another important layer from clinical and therapeutic perspectives. The feedback provided by the FG could be particularly beneficial for both clinicians and patients, helping to accelerate their rehabilitation progress. An office setup with a keyboard and mouse, depicted in Fig. 6a, may represent a typical environment for many individuals. Figure 6b illustrates data on the FG from three healthy volunteers (Supplementary Table 5) who participated in this study, showing different ranges of motion but similar trends. Although the range of motion for PIP joint in the index fingers varies among individuals as well as between their hands (68.3 ± 15.3°), the average angles across all PIP joints are comparable (28.2 ± 5.8°). Notably, the left index finger exhibits lower ranges of motion than the right index finger. This variation likely stems from the difference in primary tasks of the right and left index fingers—keyboard typing and mouse clicking/scrolling, respectively. The time-series data (Fig. 6b; Supplementary Fig. 29) clearly illustrates these trends. Long-term measurements capture PIP joint in the index fingers of a healthy volunteer (subject 15) in a workplace setting. Compared to results from the office setup, these long-term measurements reveal a slightly higher overall angle (31.9 ± 0.4°) and a wider range (112.5 ± 2.9°), reflecting more dynamic motions from various activities. In situations where a rehabilitation or injury-prevention plan requires avoidance of extreme flexion or extension, this device could prove useful by notifying the user of motion beyond a specified range. Ideally, this process of biofeedback could train the user to sense when they approach the bounds of the specified range, thus allowing the device to be discontinued after sufficient training (while still having ongoing benefit).

a A photograph of the finger goniometer worn on the right index finger to track PIP joint motions during office work, captured over 1 hour. b The measured range of motion in the joint angles for three healthy subjects (left), and time-series data of measured angles of Subject 1 (right). c Long-term (7-hour) measurements of PIP joint angles in both the left and right index fingers, showing their range and time-series data. The time-series data consist of over 627,000 data points for each finger, and the range was estimated from these data. d An image of the device on the right index finger during baseball throwing, executed ten times. e The measured range of motion in joint angles (left), and time-series data of Subject 1 (right), with red triangle markers indicating release points. f An image of the device on the right hand while playing the piano. g Time-series data of measured angles and a music sheet from a specific section of the performance. Boxes in (b, c, e) represent the interquartile range (IQR) from the 25th to the 75th percentiles; whiskers extend to 1.5 times the IQR; and the midline within each box indicates the median of the dataset.
Beyond clinical applications, another advantage of using this system is its ability to track joint kinematics during vigorous activities, including sports and playing musical instruments. Figure 6d illustrates this capability by demonstrating the FG during a baseball throw. Results from three healthy volunteers (Supplementary Table 5) shown in Fig. 6e reveal varying ranges of motion in the PIP joint of the right index finger (62.5 ± 18.5°), reflecting differences in the throwing habits of each volunteer. In addition, the time-series data (Fig. 6e; Supplementary Fig. 30) illustrate angles while holding and releasing a ball. Such results may be useful for analyzing pitching techniques. The usability of the FG extends to tracking PIP joint motions while playing musical instruments, as illustrated in Fig. 6f. Figure 6g and Supplementary Movie 7 display the changes in angle of the PIP joints in the left and right index fingers while a user plays a section of Kaiser-Walzer, Op. 437. The time-series data show that the FG effectively captures the joint motions of both fingers during the performance. Notably, the measured angles exhibit slight variations between trials, even though the same musician plays the same section of the song (Supplementary Fig. 31). Through advanced data analysis, such data can assist musicians in refining their techniques or adjusting their playing habits by enabling comparisons of motion data across different performances.
Discussion
The electrogoniometry systems presented here facilitate continuous monitoring of joint kinematics while addressing typical challenges associated with wearable electrogoniometers, which would benefit both patients and clinicians. The operation relies on simple measurements of the magnetic field strength from a permanent magnet, with the magnet and magnetometer placed distal and proximal (respectively) to a target joint. Computer vision incorporated in a smart device precisely calibrates responses of the magnetometer to joint angles. This instant and easy calibration strategy, designed to take 4 seconds, can bypass the need for additional equipment, large training datasets for machine learning, and significant computational power for magnet pose reconstruction. Consequently, patients could utilize the presented systems with real-time biofeedback displayed on an intuitive GUI in a routine and frequent manner, regardless of the setting or the presence of a clinician.
Given the results from comprehensive experiments including physical simulations, demonstrations with two ground truth methods, and human trials, the technology—demonstrating clinically acceptable reliability—would reduce previously reported uncertainties resulting from goniometers and practitioners. The strong compatibility with general rehabilitation exercises shown by the FG would allow both patients and clinicians to receive real-time joint angle biofeedback during exercise. Ideally, this technology could be made available to patients who require routine performance of a HEP. They would don the device at home for each exercise session, and receive real-time feedback, rather than (approximately) weekly feedback only when visiting a therapist. This routine biofeedback may facilitate better engagement more with the exercise program, help the patient push harder to gain improvement, and ultimately facilitate the achievement of a superior outcome. Future study will specifically examine how this device truly impacts the patient experience and clinical outcomes.
Additionally, the ability of the system to perform long-term continuous monitoring during daily activities would be advantageous for tracking joint usage throughout the day, particularly benefiting patients who require some feedback to avoid the extremes of motion (i.e. patients in the early phases of flexor tendon rehabilitation). Furthermore, additional kinematic parameters, including angular velocity and acceleration (Supplementary Fig. 32), may serve as useful biomarkers for evaluating rehabilitation progress. Previous work has used such parameters to monitor hand rehabilitation in post-stroke patients43 and confirm relationships between angular speed and muscle weakness in Parkinson’s disease44. By leveraging the full rotation matrix of ArUco markers21 and the orientation of a magnet, multi-DOF monitoring of a wrist joint, demonstrated in Supplementary Fig. 26, suggests a promising prospect for the future generalization of this technology to larger and more complex joints. While the primary target of the electrogoniometry systems is medical diagnostics and rehabilitation, the full kinematic parameters could also be applied to physical activities, as demonstrated in this work with joint angles. Further opportunities may emerge in both medical and physical activity contexts when the systems are integrated with immersive technologies.
Methods
Device preparation
A commercial electronic design software package (Eagle 9.6.2, Autodesk) was used to design the fPCB. Custom firmware was developed using an integrated development environment (Embedded Studio, SEGGER) and uploaded to the BLE SoC. To mitigate potential electromagnetic interference from nearby metallic components, a wireless charging coil was integrated with an NFC film (IBQ15, TDK Corporation) and then tuned using a set of ceramic capacitors. This electronics preparation was completed by folding the wireless coil onto the fully populated fPCB, as shown in Supplementary Fig. 1.
Silicone enclosures for encapsulating the electronics with a 3.7-V lithium polymer battery (45 mAh; dimensions: 15 mm length, 12 mm width, and 4 mm thickness) were prepared using a set of acrylic molds manufactured with a benchtop milling machine (Roland MDX540). Liquid silicone (Silbione RTV 4420) dyed with white pigment (Silc Pig, White, Smooth-On; 10 wt.%) was poured into the molds and then cured in an oven at 80 °C for one hour. The top shells of each segment contained slots to mate with black patterns of ArUco markers. After cooling, the electronics and the battery were sandwiched between silicone shells in the molds, which were then filled with liquid silicone (Eco-Flex 0035, Smooth-On). The assembly was clamped and left at room temperature for 5 min, allowing the liquid silicone to solidify and bond the two silicone shells together. Excess material was trimmed using a custom cutting die to achieve the desired device shape. For the strap of the FG, seven holes were punched at 5 mm intervals using a 1.5 mm biopsy punch, and a custom pin—an assembly of a 3D-printed stud and a copper hollow rivet—was inserted and secured with silicone adhesive (Sil-poxy, Smooth-On), as illustrated in Supplementary Fig. 1a. For the WG, a single hole was made on each segment, and a larger custom pin was attached to the magnet segment using the same adhesive (Supplementary Fig. 1b).
The black patterns of ArUco markers were fabricated separately by casting the Silbione RTV in a machined acrylic mold. Similar to the white silicone shells, 10 wt.% of black pigment (Silc Pig, Black, Smooth-On) was used to dye the silicone to achieve high contrast for ArUco markers. The black-dyed silicone was cured in an oven 80 °C for one hour, and then peeled off from the mold. The black patterns were refined by cutting excess material with a razor blade and secured in the slots of the white shells using Sil-poxy.
Experimental setup
A custom motorized stage, constructed on an aluminum breadboard, possessed a stepper motor (1478, Pololu), a commercial motor controller (Tic T825, Pololu), a 3D printed rod with acrylic plates, and manual stages, as illustrated in Supplementary Fig. 2. This motorized stage was designed to characterize responses of the electrogoniometry systems under constrained conditions, focusing on their accuracy and reliability. The main component, the stepper motor, operated smoothly at targeted rates through 1/16 microstepping, managed by the Teensy 3.6 (PJRC) which communicated with the motor controller via I2C using custom Arduino code. A 3D printed rod (125 mm length), connected to the motor rod, effectively positioned the magnetometer at a sufficient distance from the motor to negate any fringing magnetic fields, as shown in Supplementary Fig. 2b. Two acrylic plates, designed to simulate the structure of targeted joints, were mounted—one at the rod’s tip (distal) and the other fixed on an aluminum bracket (proximal)—and aligned precisely with manual stages. Adjusting the configuration of the 3D-printed rod and acrylic plates enabled the simulation of flex/ext and rad/uln motions, as illustrated in Supplementary Fig. 2c, e.
Stepper motors are typically considered highly reliable, leading to often being used without encoders. Therefore, the motions of the custom motorized stage were recorded at 60 fps using a smart device (iPhone XR, Apple Inc.). These videos were subsequently analyzed with an open-source video analysis package (Tracker, Open Source Physics). Three fiducial markers—located on the distal, proximal, and at the center of the joint—facilitated the estimation of joint angles at each video frame, as shown in Supplementary Fig. 2d, f.
Collecting reference functions for extrapolation
The same benchtop experimental setup was employed to collect reference functions for extrapolation during the calibration step. Magnetic field strengths read by a magnetometer typically depend on the relative distances between a magnet and a magnetometer. To explore this dependency, responses of the magnetometer were investigated by adjusting these distances, as illustrated in Supplementary Fig. 9a. Both the magnet cuboid and the magnetometer were moved in 1 mm longitudinal steps within the distances investigated ranging from 5 mm to 40 mm for the magnet cuboid on the distal and from 10 mm to 45 mm for the magnetometer on the proximal. For the transverse distances, only the magnet cuboid was moved in 2.5 mm transverse steps within the 0 mm to 7.5 mm range. While positioned at each location within the test windows, the stepper motor generated quasi-static step rotations with an increment of 0.9° across two different ranges of motion: −18° to 110° for the FG and -75° to 75° for the WG. At each step, the motor paused for 1.5 seconds, and data of the magnetometer were collected. Curve fitting was performed on the collected data using third-order polynomials with Matlab R2022b (MathWorks), as the relationship must be bijective for practical use. Heat maps, shown in Supplementary Fig. 9b, illustrate the \({R}^{2}\) values from the curve fitting; 120 functions with \({R}^{2}\) values close to 0.99 were selected as reference functions and utilized in the calibration step.
Measuring changes in joint angles using 3D marker tracking and 2D markerless tracking
A custom multi-camera setup was built to record videos of targeted joints undergoing specified movements, as shown in Supplementary Fig. 21a. A previous study45 highlighted the advantages of this vision-based setup for analyzing the underlying mechanics in skin-interfaced electronics. DeepLabCut and Pose3D39,46 were used together to benchmark the device by estimating changes in joint angles. Although DeepLabCut functions as a markerless system, the tracked points were trained using physical markers to enhance accuracy—similar to marker-based systems such as Vicon and OptiTrack. Videos of flex/ext motions of PIP joints in all hand digits and both flex/ext and rad/uln motions of a wrist were captured using four time-synchronized high-speed cameras (2048 × 1088 resolution; HT-2000M, Emergent) equipped with 35 mm lenses (F1.4 manual focus; Kowa) at 60 fps. A user wore the electrogoniometry systems, which were equipped with four fiducial markers for this 3D tracking. The 3D tracking process involved stereo camera calibration, data collection, iterative frame labeling, network training, evaluation for all camera pairs, triangulation, and post-processing, as depicted in Supplementary Fig. 21b.
3D movements of fingers and wrists were associated with translations of up to 40 mm and rotations of up to 110°, leading to challenges in accurately estimating 3D positions over time. To address these challenges, over 100 stereo camera calibration images were collected and filtered based on a reprojection error of \(\bar{{{{\rm{\varepsilon }}}}}\) < 0.2 pixels. Each dataset was then labeled and processed separately using a convolutional neural network (ResNet50), achieving a detection likelihood of over 90%. An open-source toolbox, Pose3D, was utilized for 3D reconstruction of the 2D tracked data. This approach achieved a root mean square deviation (RMSE) of less than 1 degree, as shown in Supplementary Fig. 21d. The same technique without the 3D reconstruction process was applied to analyze videos recorded using a mini C-arm fluoroscopy (Fluoroscan Insight FD, Hologic Inc.) at 30 fps. DLC successfully recognized and tracked four key points—the head and base of the middle phalanx, and the head and center of the proximal phalanx—in these 2D fluoroscopic videos. Using the obtained positions of these points in 2D space, joint angles were accurately estimated.
Protocols for human subject studies
The human subject studies were approved by the Institutional Review Board of Washington University in St. Louis (202304036). Informed consent was obtained from each participant prior to every experiment, and participants were not compensated. Adults between 18 to 65 years of age took part in the study. Although participants self-reported their sex, age and sex/gender were not considered in the human trials, as the study focused on joint angle measurements in the fingers. These measurements provide more relevant information about device functionality across varying hand sizes, which are more pertinent to hand therapy than age or sex/gender. No other factors associated with age or sex were expected to influence the study outcomes. Details of participants are available in Supplementary Table 5.
Reporting summary
Further information on research design is available in the Nature Portfolio Reporting Summary linked to this article.
Data availability
The benchtop experimental data generated in this study have been deposited in the Figshare database under accession code https://doi.org/10.6084/m9.figshare.2886165547. The human trial data are protected and are not publicly available due to data privacy laws. However, anonymized data can be made available upon request for academic purposes. Sample data from the human trials is also available in the repository.
References
Baldwin, M. L. & Butler, R. J. Upper extremity disorders in the workplace: Costs and outcomes beyond the first return to work. J. Occup. Rehabil. 16, 296–316 (2006).
Keogh, J. P., Nuwayhid, I., Gordon, J. L. & Gucer, P. W. The impact of occupational injury on injured worker and family: Outcomes of upper extremity cumulative trauma disorders in Maryland workers. Am. J. Ind. Med. 38, 498–506 (2000).
Mkandawire, N. C., Boot, D. A., Braithwaite, I. J. & Patterson, M. Musculoskeletal recovery 5 years after severe injury: long term problems are common. Injury 33, 111–115 (2002).
Robinson, L. S., Sarkies, M., Brown, T. & O’Brien, L. Direct, indirect and intangible costs of acute hand and wrist injuries: A systematic review. Injury 47, 2614–2626 (2016).
Faria-Fortini, I., Michaelsen, S. M., Cassiano, J. G. & Teixeira-Salmela, L. F. Upper extremity function in stroke subjects: relationships between the international classification of functioning, disability, and health domains. J. Hand Ther. 24, 257–265 (2011).
Dalyan, M., Cardenas, D. D. & Gerard, B. Upper extremity pain after spinal cord injury. Spinal Cord. 37, 191–195 (1999).
van Oosterom, F. J. T., Ettema, A. M., Mulder, P. G. H. & Hovius, S. E. R. Impairment and Disability After Severe Hand Injuries With Multiple Phalangeal Fractures. J. Hand Surg. 32, 91–95 (2007).
Korhonen, L., Pokka, T., Holappa, A., Serlo, W. & Sinikumpu, J.-J. The measurement methods of movement and grip strength in children with a previous upper extremity fracture: a comparative, prospective research. Scand. J. Surg. 109, 351–358 (2020).
Mawase, F. et al. Pushing the rehabilitation boundaries: hand motor impairment can be reduced in chronic stroke. Neurorehabil. Neural Repair. 34, 733–745 (2020).
Kloosterman, M. G. M., Snoek, G. J. & Jannink, M. J. A. Systematic review of the effects of exercise therapy on the upper extremity of patients with spinal-cord injury. Spinal Cord. 47, 196–203 (2009).
Beebe, J. A. & Lang, C. E. Active range of motion predicts upper extremity function 3 months after stroke. Stroke 40, 1772–1779 (2009).
Groth, G. N. & Wulf, M. B. Compliance with hand rehabilitation: health beliefs and strategies. J. Hand Surg. 8, 18–22 (1995).
Bassett, S. F. The assessment of patient adherence to physiotherapy rehabilitation. N. Z. J. Physiother. 31, 60–66 (2003).
Giggins, O. M., Persson, U. M. & Caulfield, B. Biofeedback in rehabilitation. J. Neuroeng. Rehabil. 10, 60 (2013).
Meijer, H. A., Graafland, M., Goslings, J. C. & Schijven, M. P. Systematic review on the effects of serious games and wearable technology used in rehabilitation of patients with traumatic bone and soft tissue injuries. Arch. Phys. Med. Rehabil. 99, 1890–1899 (2018).
Ellis, B., Bruton, A. & Goddard, J. R. Joint angle measurement: a comparative study of the reliability of goniometry and wire tracing for the hand. Clin. Rehabil. 11.4, 314–320 (1997).
Ellis, B. & Bruton, A. Clinical assessment of the hand - a review of joint angle measures. Hand Ther. 3.2, 5–8 (1998).
Burr, N., Pratt, A. L. & Stott, D. Inter-rater and intra-rater reliability when measuring interphalangeal joints: comparison between three hand-held goniometers. Physiotherapy 89, 641–652 (2003).
Kiatkulanusorn, S. et al. Analysis of the concurrent validity and reliability of five common clinical goniometric devices. Sci. Rep. 13, 20931 (2023).
Wu, E. et al. Back-Hand-Pose: 3D hand pose estimation for a wrist-worn camera via dorsum deformation network. UIST 20, 1147–1160 (2020).
Yuan, T., Song, Y. W., Kraan, G. A. & Goossens, R. H. M. Identify finger rotation angles with ArUco markers and action cameras. J. Comput. Inf. Sci. Eng. 22, 031011 (2022).
Metcalf, C. D. et al. Markerless motion capture and measurement of hand kinematics: validation and application to home-based upper limb rehabilitation. IEEE Trans. Biomed. Eng. 60, 2184–2192 (2013).
Mulla, D. M., Majoni, N., Tilley, P. M. & Keir, P. J. Two cameras can be as good as four for markerless hand tracking during simple finger movements. J. Biomech. 2025, 112534 (2025).
Dejace, L., Laubeuf, N., Furfaro, I. & Lacour, S. P. Gallium-based thin films for wearable human motion sensors. Adv. Intell. Syst. 1, 1900079 (2019).
Araromi, O. A. et al. Ultra-sensitive and resilient compliant strain gauges for soft machines. Nature 587, 219–224 (2020).
Li, L. et al. Embedded FBG-based sensor for joint movement monitoring. IEEE Sens. J. 21, 26793–26798 (2021).
Kim, J. S. et al. Wearable hand module and real-time tracking algorithms for measuring finger joint angles of different hand sizes with high accuracy using FBG strain sensor. Sensors 20, 1921 (2020).
Lyons, K. Wearable magnetic field sensing for finger tracking. ISWC 20, 63–67 (2020).
Parizi, F. S., Whitmire, E. & Patel, S. AuraRing: precise electromagnetic finger tracking. Proc. ACM Interact. Mob. Wearable Ubiquitous Technol. 3, 150 (2019). 1–150:28.
Liu, Y., Zhang, S. & Gowda, M. Neuropose: 3D hand pose tracking using EMG wearables. Proc. ACM Interact. Mob. Wearable Ubiquitous Technol. 5, 1471–1482 (2021).
Ngeo, J. G., Tamei, T. & Shibata, T. Continuous and simultaneous estimation of finger kinematics using inputs from an EMG-to-muscle activation model. J. Neuroeng. Rehabil. 11, 1–14 (2014).
Shull, P. B. et al. Hand gesture recognition and finger angle estimation via wrist-worn modified barometric pressure sensing. IEEE Trans. Neural Syst. Rehabil. Eng. 27, 724–732 (2019).
Connolly, J., Condell, J., O’Flynn, B., Sanchez, J. T. & Gardiner, P. IMU sensor-based electronic goniometric glove for clinical finger movement analysis. IEEE Sens. J. 18, 1273–1281 (2017).
Sharma, A. et al. SparseIMU: Computational design of sparse IMU layouts for sensing fine-grained finger microgestures. ACM Trans. Comput. -Hum. Interact. 30, 1–40 (2023).
Levanon, Y. The advantages and disadvantages of using high technology in hand rehabilitation. J. Hand Ther. 26, 179–183 (2013).
Norkin, C. C. & White, D. J. Measurement of Joint Motion: A Guide to Goniometry (F.A. Davis, 2016).
Garrido-Jurado, S., Muñoz-Salinas, R., Madrid-Cuevas, F. J. & Marín-Jiménez, M. J. Automatic generation and detection of highly reliable fiducial markers under occlusion. Pattern Recognit. 47, 2280–2292 (2014).
Markwardt, C. B. Non-linear least squares fitting in IDL with MPFIT. ArXiv 0902, 2850 (2009).
Mathis, A. et al. DeepLabCut: Markerless pose estimation of user-defined body parts with deep learning. Nat. Neurosci. 21, 1281–1289 (2018).
Häger-Ross, C. & Schieber, M. H. Quantifying the independence of human finger movements: comparisons of digits, hands, and movement frequencies. J. Neurosci. 20, 8542–8550 (2000).
Charles, P. D. et al. Classification of tremor and update on treatment. Am. Fam. Phys. 59, 1565–1572 (1999).
Bear-Lehman, J. & Abreu, B. C. Evaluating the hand: issues in reliability and validity. Phys. Ther. 69, 1025–1033 (1989).
Huang, X., Naghdy, F., Du, H., Naghdy, G. & Murray, G. Design of adaptive control and virtual reality-based fine hand motion rehabilitation system and its effects in subacute stroke patients. Front. Neurosci. 6, 678–686 (2012).
Pang, M. Y. & Mak, M. K. Influence of contraction type, speed, and joint angle on ankle muscle weakness in Parkinson’s disease: implications for rehabilitation. Arch. Phys. Med. Rehabil. 93, 2352–2359 (2012).
Kim, J.-T. & Chamorro, L. P. Coupled mechanics in skin-interfaced electronics via computer vision methods. Soft Sci. 4, 12 (2024).
Sheshadri, S., Dann, B., Hueser, T. & Scherberger, H. 3D reconstruction toolbox for behavior tracked with multiple cameras. J. Open Source Softw. 5, 1849 (2020).
Shin, H.-S., et al Benchtop experimental results of the electrogonimetry system and sample data collected during human trials. figshare https://doi.org/10.6084/m9.figshare.28861655 (2025).
Acknowledgements
This work was supported by the Querrey-Simpson Institute for Bioelectronics at Northwestern University. J.-Y. Y acknowledges funding from the Alchemist Project Program (RS-2024-00422269), supported by the Ministry of Trade, Industry & Energy (MOTIE, Korea), as well as the Competency Development Program for Industry Specialists of the Korean Ministry of Trade, Industry and Energy (MOTIE), operated by the Korea Institute for Advancement of Technology (KIAT). J.-T. K acknowledges funding from the National Research Foundation of Korea (NRF) grant funded by the Korea government (MSIT) (RS-2024-00342270; RS-2024-00406674) and funded by the Ministry of Science & ICT, Korea.
Author information
Authors and Affiliations
Contributions
H.-S.S., M.A.P., and J.A.R. conceived the idea and designed the research. H.-S.S. and J.-Y.Y. designed the wireless electronics, algorithm, and graphical user interface. H.-S.S. and J.K. designed and fabricated the goniometry systems. H.-S.S., M.A.P., and J.A.R. designed the benchtop experiments and H.-S.S., J.K., Y.S., M.J., J.B., A.T., and M.P. performed the experiments and analyzed the data. J.-T.K. performed 3D marker tracking and 2D markerless tracking. H.-S.S., N.F., L.B.P., K.K., and M.A.P. conducted human studies in clinical settings. H.-S.S., J.K., C.L., J.-T.K., and J.-Y.Y. conducted human studies in non-clinical settings. H.-S.S., J.K., J.-T.K., J.-Y.Y., M.A.P., and J.A.R. drafted the manuscript, and all the other authors contributed to writing and revising the manuscript. M.A.P. and J.A.R. supervised the overall research.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Peer review
Peer review information
Nature Communications thanks Aditya Shekha Nittala, Simiao Niu, and the other, anonymous, reviewer(s) for their contribution to the peer review of this work. A peer review file is available.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Shin, HS., Kim, J., Fadell, N. et al. Soft, skin-interfaced wireless electrogoniometry systems for continuous monitoring of finger and wrist joints. Nat Commun 16, 4426 (2025). https://doi.org/10.1038/s41467-025-59619-z
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41467-025-59619-z
