
Abstract
Long-term effects of COVID-19 infection, termed Long COVID (LC), are associated with reduced quality of life. Symptoms associated with overweight/obesity overlap with and may aggravate those of LC. This paper reports the economic evaluation alongside the ReDIRECT Trial, which evaluated the impact of an evidence-based, remotely-delivered weight management programme on self-reported symptoms of LC in those living with overweight/obesity in the United Kingdom. Recruited participants (n = 234) were randomly allocated to the intervention group (weight management) or control group (usual care). Incremental costs and Quality-Adjusted Life Years (QALYs) were calculated using intervention cost, healthcare resource use and EQ-5D-5L data collected at baseline, three and 6 months. In this work, we show that the ReDIRECT intervention is likely cost-effective in improving LC symptoms from an NHS/PSS perspective, compared to usual care (Incremental Cost-Effectiveness Ratio of £14,754/QALY). Adopting a broader societal perspective, the intervention becomes potentially cost saving compared to usual care.
Similar content being viewed by others

Introduction
Long COVID (LC), described as persistent symptoms following COVID-19 infection, places a large burden on health systems globally1, with those affected suffering a wide range of symptoms, including fatigue, breathlessness, cognitive dysfunction and widespread pain2,3. Although research into treatment of LC is ongoing, there are no established interventions, other than self-management, support and information, and treatment of individual symptoms4,5. A Bayesian meta-regression of 54 studies and two databases estimated that, of individuals surviving symptomatic episodes of COVID-19 infection, 6.2% experienced at least one LC symptom 3 months after initial infection, with 15.1% of these individuals experiencing persistent symptoms at 12 months6. Studies with matched controls conducted in the UK and the Netherlands suggest its prevalence is between 6 and 12% three to six months after initial COVID-19 infection, with UK estimates suggesting 10% prevalence of symptoms up to 18 months after infection7,8.
In addition to the clinical and quality of life burden, LC carries a substantial economic burden at both individual and societal levels9,10,11,12. LC has been found to affect labour participation, employment, and productivity of individuals as well as their caregivers13. Even in those not hospitalised with COVID-19, up to 23% of people remain absent from work between three and seven months after acute infection11. In addition to full absence from work, reduced capacity to work is also a factor11, with the mean monthly income from work declining by 24.5% in a survey of people living with LC in the UK14. Therefore, evaluating interventions that may reduce the clinical and economic burden of LC are of societal importance9,12,13.
Previous research has hypothesised that symptoms associated with overweight/obesity overlap with, and may aggravate, those of LC15. It is established that weight loss can improve health-related quality of life (HRQoL)16,17,18 and may also lower levels of systemic inflammation19,20,21,22, one potential factor in LC pathophysiology23,24. The Remote Diet Intervention to Reduce Long COVID Symptoms Trial (ReDIRECT) is a randomised controlled trial (RCT), which evaluated whether a remotely delivered weight loss intervention can help to alleviate the symptoms of LC in those living with overweight/obesity2. The intervention, Counterweight-Plus, is a dietary weight management programme, which the DiRECT trial showed to be safe, effective, and cost-effective in achieving and sustaining weight loss and remission of Type 2 Diabetes25,26. In the ReDIRECT RCT, the weight management programme was delivered remotely, using digital technology and remote dietetic advice2.
This economic evaluation estimated the likely cost-effectiveness of the remotely delivered Counterweight-Plus intervention to alleviate LC symptoms. It is vital to understand the value for money gained from the intervention to inform decision-making on its implementation27.
Results
Baseline characteristics
The characteristics of the study population at baseline are presented in Table 1, with further details reported elsewhere15. Participant characteristics, including mean age, weight, and utility were similar across the intervention and control groups.
Health-related quality of life (HRQoL)
Utility scores for each participant were calculated using the EuroQol-5 Dimensions-5 Levels questionnaire (EQ-5D-5L) data, mapped to EQ-5D-3L utilities using the UK value set, and are presented in Fig. 1 by trial arm over the trial period. Figure 1a reports mean utility scores with standard error shading, while Fig. 1b shows the distribution of the utility scores in each arm, including the presence of outliers at the lower end of the utility score spectrum. Table 2 presents the summary results of the Area Under the Curve (AUC) utility score analysis (unadjusted and adjusted for baseline covariates), with total Quality-Adjusted Life Years (QALYs) calculated.

a Line graph showing mean utility score by trial arm, with standard error shading (n = 118 control, n = 116 intervention), and b box plot showing the distribution of utility scores by trial arm over the trial period (n = 118 control, n = 116 intervention). The box plots show the median (centre line), the first and third quartiles (the lower and upper bounds of the box), and the whiskers show 1.5× the interquartile range. Points beyond the whiskers are ‘outlying’ points plotted individually. Source data are provided with this paper.
Intervention micro-costing
Counterweight Ltd charges the NHS £1,000 per person for delivery of the intervention, which was therefore deemed the appropriate intervention cost to use in the base case analysis (rather than the micro-cost estimate). Micro-costing of the intervention, with cost components identified, measured, and valued resulted in a mean cost per participant of approximately £885 (base year 2022) — see Table S2 in the Supplementary Materials.
Healthcare resource use
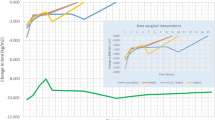
Figure 2a presents a line graph showing the mean cost per participant by trial arm at baseline, 3 months and 6 months, while Fig. 2b presents box plots of the distribution of this resource use over the same period. These plots illustrate the difference between the mean resource use at baseline in the two trial arms, as well as the presence of healthcare resource use outliers – typically resulting from hospitalisation in the 3 months preceding each assessment. One observation, found to have particularly high healthcare resource use at baseline (in the control arm), was subject to a further sensitivity analysis (outlier removed). This sensitivity analysis showed that excluding the outlier observation would not alter the interpretation of cost-utility analysis results (Supplementary Materials Tables S3 and S4 and Figs. S1 and S2). With no further indication to remove the outlier, this observation was included in the base case analysis. Differences in healthcare resource use in the intervention arm, relative to the control arm, were not statistically significant at 6 months (mean difference: -£47.03, 95% CI: -£236.83 to £142.77).

a shows the mean resource use per participant over the trial period, by trial arm, with standard error shading (n = 118 control, n = 116 intervention); b shows box plots of the distribution of resource use costs among participants over the trial period, by trial arm (n = 118 control, n = 116 intervention). The box plots show the median (centre line), the first and third quartiles (the lower and upper bounds of the box), and the whiskers show 1.5× the interquartile range. Points beyond the whiskers are ‘outlying’ points plotted individually. c is a bar chart showing resource use category cost drivers over the trial period, by trial arm (n = 118 control, n = 116 intervention). Source data are provided with this paper.
The healthcare resource use cost drivers are displayed in Fig. 2c, showing high hospitalisation costs at baseline and 3 months after randomisation for the control arm, relative to the intervention arm. Summary cost results (unadjusted and adjusted for baseline covariates) are presented in Table 3.
Societal perspective: productivity losses
Figure 3a shows the total number of hours of work missed due to sickness in the week prior to each assessment, by trial arm, while Fig. 3b shows the mean number of hours of work missed due to sickness in each arm over the trial period. With weekly wage rates applied to hours missed due to sickness and extrapolated over the trial period, the costs associated with lost productivity are presented in Table 3, along with per-person food costs. The mean number of hours of work missed due to sickness reduced by 2.3 (SD 14.02) in the control arm and by 2.8 (SD 14.50) in the intervention arm, on average, with a treatment effect of 1.91 (95% CI −1.01 – 4.83, p = 0.20), adjusting for primary outcome selected, sex, age, index of multiple deprivation, ethnicity and hours of work missed due to sickness at baseline.

a Bar chart showing the total number of hours of work missed, by trial arm; b line graph showing mean number of hours of work missed per participant, by trial arm, with standard error shading. Source data are provided with this paper.
Handling missing data
Data were assessed to be missing at random (MAR), with an imbalance in missingness by trial arm: 1 observation (out of 354) was missing in the control arm, while 36 observations (out of 348) were missing in the intervention arm, with a total of 25 individuals having at least one missing observation (1 out of 118 in the control arm and 24 out of 116 in the intervention arm). Multiple imputations using chained equations (MICE) was used to impute missing data with 10 iterations using the mice function in R28. Seemingly unrelated regression (SUR) models controlled for age, sex, index of multiple deprivation, the participant-selected primary outcome, as well as costs and utility at baseline. Pooled cost difference and effect difference were estimated from 5000 bootstrapped replicates of the imputed dataset using Rubin’s Rules to estimate the incremental cost-effectiveness ratio (ICER) and 95% confidence intervals.
Cost-effectiveness analysis
Figures 4a, c present ICER planes of the bootstrapped results from the National Health Service and Personal Social Services (NHS/PSS) perspective and societal perspective, respectively, while Fig. 4b, d present cost-effectiveness acceptability curves (CEACs) from the NHS/PSS and societal perspectives, respectively. In Fig. 4a, c, the diagonal lines crossing through the planes represent the £30,000/QALY cost-effectiveness threshold indicated for use by the National Institute for Health and Care Excellence (NICE)29, with the corresponding CEACs - Fig. 4b, d - showing the probability of weight management being considered cost-effective at different cost-effectiveness thresholds. Figure 4b shows that at a threshold of £20,000/QALY, there would be approximately 72% probability of the intervention being considered cost-effective, increasing to 89% at a threshold of £30,000/QALY. From a broader societal perspective, Fig. 4d shows that there would be a 93% probability of the intervention being considered cost-effective at a threshold of £20,000/QALY, increasing to 96% at a threshold of £30,000/QALY. Further, Fig. 4c, d indicate that the intervention may be cost-saving when a societal perspective is adopted, with a 74% probability of being cost-saving at a threshold of £0/QALY.

Each individual had three scheduled observations, with a total of 37/702 missing observations (1/354 missing observation in the control arm, 36/348 missing observations in the intervention arm). a ICER Plane from the NHS/PSS perspective. b CEAC from the NHS/PSS perspective. c ICER Plane from the societal perspective. d CEAC Plane from the societal perspective. QALY: Quality-adjusted life year.
Table 4 presents the pooled estimates, along with the 95% confidence intervals, for the between-group QALY and cost differences, from the NHS/PSS perspective and the broader societal perspective.
Discussion
This paper reports the within-trial cost-utility analysis of the ReDIRECT trial, a remotely-delivered weight management programme to alleviate symptoms of LC5. In the base case analysis, taking an NHS/PSS perspective, we found that weight management is likely to be cost-effective, with an ICER of approximately £14,800/QALY and an 89% probability of cost-effectiveness at a £30,000/QALY threshold.
The primary outcome result within the ReDIRECT trial mirrored the HRQoL findings, with self-reported LC symptoms of fatigue, breathlessness and anxiety/depression improving at 6 months in the intervention group compared to the control group5. Compared to an age- and sex-adjusted UK general population utility score of 0.8630, the baseline utility scores in our study population were relatively low, with a mean utility of 0.478 (SD = 0.255) across the two trial arms. For context, a study estimating HRQoL for patients with myalgic encephalomyelitis (ME) and chronic fatigue syndrome (CFS), using the EQ-5D, reported a mean population utility score of 0.469 (95% CI 0.408 − 0.530)31. ME/CFS is also considered to be a severely debilitating condition and such low HRQoL scores for this study’s LC population provide evidence of the severe impact of LC on those affected.
At 6 months post-randomisation, the incremental QALY gain was 0.0502 (95% CI 0.0127 − 0.0876), with Fig. 1a showing an increase in health utility for the intervention arm at 3 months post-randomisation, and the between-group difference narrowing at 6 months. Other studies evaluating similar remotely delivered weight management interventions report mixed findings relating to HRQoL. A remotely delivered self-directed behavioural intervention (with minimal coaching) among adults with obesity in the US did not impact on HRQoL (p = 0.81), with authors suggesting that interventions with behavioural support have greater effect sizes, as the weight loss found in the intervention group was not deemed clinically significant (1.93 kg, 95% CI 0.61 − 3.24)32. Another study, conducted in the UK, found that a digital weight loss management intervention showed no evidence of significant weight loss or cost-effectiveness33. A lifestyle intervention in the Netherlands involving remote counselling via email found an increase in health utility (measured using the EQ5D) and a 60% probability of being cost-effective at a €20,000/QALY threshold. The between-group difference in health utility gain (0.01) was not statistically significant (95% CI −0.01 − 0.04), which may have been due to a relatively high baseline mean health utility in this population of 0.91334. Important to note is that none of these studies included a total diet replacement component in the intervention, and they did not report clinically meaningful weight loss in the intervention groups when compared to the controls. These comparisons suggest that there may be specific features of the ReDIRECT intervention and study population that play a role in the QALY gain found – particularly the low baseline health utility in our population, the total diet replacement, and the higher level of contact that participants in our study had with dietitians, enhancing the behavioural component of the intervention.
There have been several randomised controlled trials evaluating interventions for the management of LC, with a living systematic review finding evidence of moderate certainty that physical and mental health rehabilitation programmes improve quality of life for people with LC symptoms35. However, to the best of our knowledge, no other economic evaluation has been published alongside a randomised controlled trial for the management of LC, which makes this study particularly timely and important.
Between-group differences in total healthcare resource use over the trial period were not statistically significant, with an adjusted difference of the intervention group relative to control group of -£264.35 (95% CI: -£640.47 to £ 111.78). While an outlier observation generated higher baseline resource use in the control arm, baseline costs were controlled for in the SUR models, ensuring that these baseline differences do not impact the cost-utility analysis results. Further, sensitivity analysis with this outlier removed did not change interpretation of the cost-utility analysis results.
When including the broader societal perspective costs associated with lost productivity and food costs, the ReDIRECT intervention becomes cost-saving, with an ICER indicating dominance of the intervention over the control. Such a finding indicates the magnitude of the economic burden of LC in terms of absenteeism from work, and demonstrates the potential societal impact of an intervention reducing not only LC symptoms, but also reducing the associated economic burden of LC.
Further to the productivity cost-savings found in the study, the remote delivery mode of the ReDIRECT intervention meant lower intervention costs faced by participants associated with time and travel, compared to interventions delivered at healthcare facilities. The DiRECT trial did not incorporate a societal perspective in the economic evaluation, hence we are unable to draw direct comparisons as to costs faced by participants associated with time, travel and productivity; however, several other studies indicate that remote delivery of interventions result in reduced time, travel and productivity costs faced by patients36,37,38,39,40. A nationwide population cohort study for Scotland found an association between socio-economic deprivation and both the risk of developing LC and reduced probability of symptom improvement41,42. This indicates the importance of equity considerations for LC and for the implementation of weight management interventions.
Several limitations apply to this within-trial economic evaluation. First, due to mirroring the trial time horizon, there is a relatively short time horizon over which we conducted the economic analysis, with 6 months of data collected for the between-group comparison. It is not yet clear how long symptoms of LC may persist beyond COVID-19 infection, but a decision-analytic model capturing costs and health impacts of weight management over a longer time horizon may provide important economic evidence to inform the implementation of the intervention on a larger scale. The US Panel on Cost-Effectiveness in Health and Medicine recommends that a societal perspective should include future medical costs and effects on future productivity and consumption43. Due to the limited time horizon of this within-trial economic evaluation, it was not possible to include such future costs.
With delayed entry into the intervention for the control group at 6 months post randomisation, we only have 6 months of RCT between-group data. However, we have 12 months of observational data for both groups receiving the intervention (the control group was followed for a total of 18 months)2. This observational data will be used to validate the extrapolation functions of costs and utilities for the intervention group in the long-term model.
There is some published evidence that health loss can be over-stated by the EQ-5D-3L compared to the EQ-5D-5L44,45,46. Therefore, mapping the EQ-5D-5L data collected to the EQ-5D-3L UK value set may have overstated health loss in our population. Future sensitivity analyses with updated UK value sets (when available) using the EQ-5D-5L would be useful to determine the impact of this on our cost-utility analysis results47.
Using £1000 as the intervention cost for the base-case analysis may not reflect the true delivery cost of the intervention in routine use. The results of the intervention micro-costing analysis indicate that the intervention costs approximately £885 per patient. This micro-costing assumed a conservative cost of £1 per participant for the development of the application, under the assumption that the application had already been developed and implemented by Counterweight Ltd before this study, using established literature for similar interventions with no opportunity costs identified48. Further, including application development cost in a within-trial cost-utility analysis with a time horizon of only 6 months means that the cost cannot be annualised, and there is no accounting for potential economies of scale on implementation of the intervention in the NHS, and thus is not appropriate in this analysis. It may be useful to include application development costs as a parameter in a decision analytic model with a longer time horizon and larger study population so that the true impact of this cost input can be reflected.
Unlike the costs, health impacts of adverse events were not explicitly modelled in the within-trial analysis, as it was assumed that any impact would be reflected in the HRQoL of participants, and thus accounted for in utility scores. In a long-term model, it may be important to explicitly account for adverse events by adding an ‘adverse event’ health state.
In conclusion, this economic evaluation alongside the ReDIRECT clinical trial suggests that weight management may be cost-effective in managing LC symptoms from an NHS/PSS perspective, compared to usual care. When a broader societal perspective is adopted, the intervention is predicted to become cost-saving, dominating usual care, with those in the intervention arm potentially achieving cost savings through productivity gains. In terms of decision-making, this weight management programme meets the health economic criteria for implementation at scale for people living with LC. A decision analytic model estimating cost-effectiveness over the longer term will be useful in informing implementation.
Methods
The main randomised controlled trial (ReDIRECT)
ReDIRECT was a wait-list RCT, with participants allocated in a 1:1 ratio at baseline to one of two groups: intervention or control (ISRCTN registry 12595520). Ethical approval of the study protocol was obtained from the South-East Scotland Research Ethics Committee 01 (reference number: 21/SS/0077). Informed consent was obtained from all trial participants.
The allocation was designed to maintain balance with respect to dominant LC symptom (as selected by each participant) and socio-demographic characteristics (sex, ethnicity and index of multiple deprivation). Assessments were taken at baseline, 3 months and 6 months.
Participants in the intervention arm were enroled in the weight management programme, with the intervention described in detail in the trial protocol2. In brief, the intervention entailed dietitian-supported total diet replacement (8–12 weeks), food reintroduction (4–12 weeks), and long-term weight-loss maintenance (up to 1 year). The intervention was delivered remotely by Counterweight Ltd via an online platform with personal video/telephone/in-app chat support. Individuals were allocated a named ‘Counterweight Coach’ (all registered dietitians) for personal support and regular appointments. All participants could join a coach-moderated in-app ‘chat’ facility for peer support. Participants allocated to the control arm received usual care and were given access to the weight management programme 6 months after baseline assessment. Usual care involved standard general practitioner (GP) care with potential referral to NHS post-COVID services, typically comprising multidisciplinary assessments, diagnostic tests, and management or appropriate onward referral to post-COVID rehabilitation49 (the economic evaluation design captured this heterogeneous resource use). Between-group RCT analysis consisted of baseline, three-month and six-month assessments.
The trial primary outcome was a continuous measure derived from the symptom score for the most important LC symptom selected by each participant at baseline (from a list of fatigue, breathlessness, pain, anxiety, depression, and “other”). Secondary outcomes included changes in any of the individual symptoms reported, weight, blood pressure, HRQoL, psychological outcomes, healthcare resource utilisation, work productivity, and personal food costs2,5. Process outcomes for the trial will be reported separately.
The study recruited 234 participants aged 18 and above living with overweight/obesity and self-reported symptoms of LC, between December 2021 and July 2022. The inclusion and exclusion criteria for the ReDIRECT Trial were detailed in the published trial protocol2 with baseline cohort characteristics described in detail elsewhere15. The trial was delivered remotely with participants recruited from across the UK (England, Scotland, Wales, and Northern Ireland).
Economic evaluation
In line with NICE guidance, the base-case within-trial cost-utility analysis of the ReDIRECT intervention compared to usual care, adopted an NHS/PSS perspective50. Secondary analysis considered a broader societal perspective (including costs associated with productivity loss, and food expenditure). The time horizon for the within-trial analysis was 6 months, in line with the RCT analysis time horizon. The economic evaluation was carried out according to a pre-specified Health Economics Analysis Plan (HEAP, available upon request), and the updated Consolidated Health Economic Evaluation Reporting Standards (CHEERS) were adhered to in all economic analysis and reporting51, with a CHEERS checklist available in the Supplementary Materials (Table S1).
Health outcome for the economic evaluation
The outcome for the economic evaluation was QALYs, estimated using the EQ-5D-5L52,53, completed at baseline, 3 months, and 6 months to generate AUC QALYs. The scores recorded were mapped to EQ-5D-3L utility values for the UK population using NICE Decision Support Unit guidelines54. A cost-utility analysis framework was adopted.
Resource use
The NHS/PSS perspective base-case analysis included intervention costs and direct health and personal social service use by participants, while the broader societal perspective also captured indirect costs associated with productivity (employment) impacts, and personal food costs. All costs were estimated in 2022 British pound sterling.
Intervention costs
In the primary analysis, the intervention cost was set at the cost to the NHS of utilising the Counterweight-Plus intervention (£1000). Micro-costing of resource use associated with the delivery of the intervention was conducted as a scenario analysis, with the unit cost inputs for each resource item presented in Table S2 in the Supplementary Materials.
Healthcare service resource use
Data on healthcare services used by participants in the preceding 3 months were collected at baseline then at 3 months and 6 months following randomisation. These data include consultations with general practitioners (GPs), nurses, allied healthcare professionals, community nurses and social workers. Data on hospital visits (both outpatient visits and in-patient stays) were also collected. The quantity of each resource use item was combined with their unit cost to estimate total healthcare resource use per participant and mean healthcare resource use for each trial arm. Unit costs attached to healthcare resource use were obtained from various sources including the Personal Social Services Research Unit (PSSRU), NHS reference costs, Scottish Health Service costs, the Office for National Statistics, and the literature (see Table 5)55,56,57,58,59,60,61,62. Data pertaining to medication use were collected for each participant at baseline, three and 6 months. Unit costs from the British National Formulary (BNF) were used to estimate the cost of medication use for each trial arm over the trial period63,64.
Adverse events
All adverse events throughout the trial were recorded2. Healthcare resource use reported by participants was cross-checked with all adverse events logged to ensure all resource use associated with potential adverse events was measured and valued for inclusion in the cost-utility analysis.
Productivity costs and personal food costs
Data were collected on hours of work missed due to illness in the preceding seven-day period at baseline, three and 6 months using the Work and Productivity Activity Impairment (WPAI) instrument65. Costs associated with lost productivity (indirect costs) were estimated for each arm over the trial period: age- and sex-specific national average weekly wage rates applied to the mean hours missed per week and extrapolated over the three-month period preceding each assessment. Similarly, participants were asked about their household food costs in the preceding seven-day period at baseline, 3 months and 6 months, as well as the number of individuals in the household. This was used to estimate a per-person food cost by trial arm, with mean weekly costs extrapolated over the three-month period preceding each assessment during the study period. The WPAI instrument and personal food and drink costs questionnaire can be found in the Supplementary Materials.
Missing data
Missing data were descriptively analysed, and MICE was conducted, separating the intervention and control arm28,66. Missing cost data were imputed at the level of the main resource use categories. Missing EQ-5D-5L data were imputed at the level of the utility score66,67. SUR models were fitted on the imputed datasets and for each imputed dataset 5000 bootstrapped samples were drawn68,69. The SUR modes included age, sex, index of multiple deprivation, baseline costs, baseline utilities and the primary outcome selected, in line with the statistical analysis conducted for the trial primary outcome. The cost and health outcome statistics of interest were then pooled using Rubin’s rules, and pooled covariance estimated66,68. An ICER plane and CEAC were derived from the output70.
Incremental cost-utility analysis
The results of the cost-utility analysis are presented as incremental costs per incremental QALY gained. An ICER was calculated as the between-group difference in the total costs divided by the difference in QALYs at 6 months post-randomisation. 95% confidence intervals were based on 5000 non-parametric bootstrap iterations. An ICER plane and CEAC were drawn from the results of the multiple imputations and presented for both the base case NHS/PSS perspective as well as the broader societal perspective.
Software
For data collection, trial participants entered data directly into bespoke electronic Case Report Forms (eCRF) and data relating to dietetic visits were entered in Excel spreadsheets. All analyses were conducted using R Statistical Software, version 4.4.1 (2024-06-14 ucrt) and RStudio version 2024.04.2−76471,72. The R packages used in the analysis include: boot (R package version 1.3−30)73, data.table (R package version 1.16.0)74, lme4 (R package version 1.1-35.5)75, mice (R package version 3.16.0)28, summarytools (R package version 1.0.1)76, ggpattern (R package version 1.1.4)77, readstata13 (R package version 0.10.1)78, viridis (package version 0.6.5)79, flextable (R package version 0.9.6)80, finalfit (R package version 1.0.8)81, systemfit (R package version 1.1-30)69, doBy (R package version 4.6.22)82, ggpubr (R package version 0.6.0)83, ggpointdensity (R package version 0.1.0)84, eq5d (R package version 0.15.3)85, table1 (R package version 1.4.3)86, miceadds (R package version 3.17)87, gtsummary (R package version 2.0.2)88, reshape (R package version 0.8.9)89, tidyverse (R package version 2.0.0)90, devtools (R package version 2.4.5)91, scales (R package version 1.3.0)92, rmarkdown (R package version 2.28)93, kableExtra (R package version 1.4.0)94.
Reporting summary
Further information on research design is available in the Nature Portfolio Reporting Summary linked to this article.
Data availability
As per our study protocol, access to the raw data is restricted to the primary research team while the research is being conducted and prior to publication of the primary research papers. The primary research papers include the primary trial outcome paper (published, ref. 5), this health economics paper, the process evaluation paper and the Patient and Public Involvement paper. Upon publication of these papers, fully anonymized and minimised data (and data dictionaries) will be placed in a research data repository with access given to bona fide researchers, on request to the corresponding author and subject to appropriate data-sharing agreements. Proposals will be assessed on a monthly basis, with a response within 2 months of submission. The Trial Statistical Analysis Plan is available via ISRCTN (10.1186/ISRCTN12595520), and ReDIRECT study eCRF questionnaire screenshots are available via Figshare at 10.6084/m9.figshare.21270837 (ref. 95). Source data for Figs. 1−3 and Fig. S1 are provided with this paper.
References
Parums, D. V. Editorial: Long COVID, or Post-COVID Syndrome, and the Global Impact on Health Care. Med. Sci. Monit. 27, e933446 (2021).
Haag, L. et al. The remote diet intervention to reduce Long COVID symptoms trial (ReDIRECT): protocol for a randomised controlled trial to determine the effectiveness and cost-effectiveness of a remotely delivered supported weight management programme for people with Long COVID and excess weight, with personalised improvement goals [version 2; peer review: 2 approved]. NIHR Open Res. 2, 57 (2023).
Davis, H. E. et al. Characterizing long COVID in an international cohort: 7 months of symptoms and their impact. eClinicalMedicine 38, 101019 (2021).
NICE. COVID-19 rapid guideline: managing the long-term effects of COVID-19. NICE Guidance. https://www.nice.org.uk/guidance/ng188/chapter/5-Management (2020).
Combet, E. et al. Remotely delivered weight management for people with long COVID and overweight: the randomized wait-list-controlled ReDIRECT trial. Nat. Med. 31, 258–266 (2025).
Wulf Hanson, S. et al. Estimated global proportions of individuals with persistent fatigue, cognitive, and respiratory symptom clusters following symptomatic COVID-19 in 2020 and 2021. JAMA 328, 1604–1615 (2022).
Ballering, A. V., van Zon, S. K. R., olde Hartman, T. C. & Rosmalen, J. G. M. Persistence of somatic symptoms after COVID-19 in the Netherlands: an observational cohort study. Lancet 400, 452–461 (2022).
Hastie, C. E. et al. True prevalence of long-COVID in a nationwide, population cohort study. Nat. Commun. 14, 7892 (2023).
Reuschke, D. & Houston, D. The impact of long COVID on the UK workforce.Appl. Econ. Lett. 30, 1–5 (2022).
Aiyegbusi, O. L. et al. Symptoms, complications and management of long COVID: a review. J. R. Soc. Med 114, 428–442 (2021).
Nittas, V. et al. Long COVID through a public health lens: an umbrella review. Public Health Rev. 43, 1604501 (2022).
Rajan, S. et al. In the Wake of the Pandemic: Preparing for Long COVID. European Observatory on Health Systems and Policies, Copenhagen (Denmark, 2021).
Al-Aly, Z. et al. Long COVID science, research and policy. Nat. Med. 30, 2148–2164 (2024).
Kwon, J. et al. Impact of Long COVID on productivity and informal caregiving. Eur. J. Health Econ. 25, 1095–1115 (2024).
Haag, L. et al. Baseline characteristics in the remote diet intervention to REduce long-COVID symptoms trial (ReDIRECT). NIHR Open Res 4, 7 (2024).
Aucott, L. et al. Effects of weight loss in overweight/obese individuals and long-term hypertension outcomes.Hypertension 45, 1035–1041 (2005).
Avenell, A. et al. Systematic review of the long-term effects and economic consequences of treatments for obesity and implications for health improvement. Health Technol. Assess. 8, 1–182 (2004).
Stenius-Aarniala, B. et al. Immediate and long term effects of weight reduction in obese people with asthma: randomised controlled study. BMJ 320, 827–832 (2000).
Sheu, W. H.-H. et al. Effect of weight loss on proinflammatory state of mononuclear cells in obese women. Obesity 16, 1033–1038 (2008).
Marfella, R. et al. Effect of weight loss on cardiac synchronization and proinflammatory cytokines in premenopausal obese women. Diab. Care 27, 47–52 (2004).
Vilarrasa, N. et al. Effect of weight loss induced by gastric bypass on proinflammatory interleukin-18, soluble tumour necrosis factor-α receptors, C-reactive protein and adiponectin in morbidly obese patients. Clin. Endocrinol. 67, 679–686 (2007).
Welsh, P. et al. Unraveling the directional link between adiposity and inflammation: a bidirectional mendelian randomization approach. J. Clin. Endocrinol. Metab. 95, 93–99 (2010).
Liew, F. et al. Large-scale phenotyping of patients with long COVID post-hospitalization reveals mechanistic subtypes of disease. Nat. Immunol. 25, 607–621 (2024).
Evans, R. A. et al. Clinical characteristics with inflammation profiling of long COVID and association with 1-year recovery following hospitalisation in the UK: a prospective observational study. Lancet Respir. Med. 10, 761–775 (2022).
Lean, M. E. J. et al. Primary care-led weight management for remission of type 2 diabetes (DiRECT): an open-label, cluster-randomised trial. Lancet 391, 541–551 (2018).
Xin, Y. et al. Type 2 diabetes remission: 2 year within-trial and lifetime-horizon cost-effectiveness of the Diabetes Remission Clinical Trial (DiRECT)/Counterweight-Plus weight management programme. Diabetologia 63, 2112–2122 (2020).
Drummond, M. F., Sculpher, M. J., Claxton, K., Stoddart, G. L. & Torrance, G. W. Methods For The Economic Evaluation Of Health Care Programmes. (Oxford University Press, 2015).
van Buuren, S. & Groothuis-Oudshoorn, K. Mice: multivariate imputation by chained equations in R. J. Stat. Softw. 45, 1–67 (2011).
National Institute for Health Care Excellence. NICE Health Technology Evaluations: The Manual. (National Institute for Health and Care Excellence, 2022).
Kind, P., Hardman. G. & Macran, S. UK population norms for EQ-5D, Working Papers 172chedp, Centre for Health Economics, University of York (1999).
Falk Hvidberg, M., Brinth, L. S., Olesen, A. V., Petersen, K. D. & Ehlers, L. The health-related quality of life for patients with myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS). PLoS ONE 10, e0132421 (2015).
Hoerster, K. D. et al. Effect of a remotely delivered self-directed behavioral intervention on body weight and physical health status among adults with obesity: the D-ELITE randomized clinical trial. JAMA 328, 2230–2241 (2022).
Sniehotta, F. F. et al. Behavioural intervention for weight loss maintenance versus standard weight advice in adults with obesity: a randomised controlled trial in the UK (NULevel Trial). PLOS Med. 16, e1002793 (2019).
van Wier, M. F. et al. Economic evaluation of a weight control program with e-mail and telephone counseling among overweight employees: a randomized controlled trial. Int. J. Behav. Nutr. Phys. Act. 9, 112 (2012).
Zeraatkar, D. et al. Interventions for the management of long covid (post-covid condition): living systematic review. BMJ 387, e081318 (2024).
Wood, P. R. & Caplan, L. Outcomes, satisfaction, and costs of a rheumatology telemedicine program: a longitudinal evaluation. J. Clin. Rheumatol. 25, 41–44 (2019).
Cuperus, N. et al. Cost-utility and cost-effectiveness analyses of face-to-face versus telephone-based nonpharmacologic multidisciplinary treatments for patients with generalized osteoarthritis. Arthritis Care Res. 68, 502–510 (2016).
Marques, A. et al. Effectiveness of remote care interventions: a systematic review informing the 2022 EULAR Points to Consider for remote care in rheumatic and musculoskeletal diseases. RMD Open 8, e002290 (2022).
Kessler, E. A., Sherman, A. K. & Becker, M. L. Decreasing patient cost and travel time through pediatric rheumatology telemedicine visits. Pediatr. Rheumatol. 14, 54 (2016).
Vudathaneni, V. K. P. et al. The impact of telemedicine and remote patient monitoring on healthcare delivery: a comprehensive evaluation. Cureus 16, e55534 (2024).
Hastie, C. E. et al. Outcomes among confirmed cases and a matched comparison group in the Long-COVID in Scotland study. Nat. Commun. 13, 5663 (2022).
Hastie, C. E. et al. Natural history of long-COVID in a nationwide, population cohort study. Nat. Commun. 14, 3504 (2023).
Sanders, G. D. et al. Recommendations for conduct, methodological practices, and reporting of cost-effectiveness analyses: second panel on cost-effectiveness in health and medicine. JAMA 316, 1093–1103 (2016).
Janssen, M. F., Bonsel, G. J. & Luo, N. Is EQ-5D-5L better than EQ-5D-3L? A head-to-head comparison of descriptive systems and value sets from seven countries. PharmacoEconomics 36, 675–697 (2018).
Martí-Pastor, M. et al. Head-to-head comparison between the EQ-5D-5L and the EQ-5D-3L in general population health surveys. Popul. Health Metr. 16, 14 (2018).
Thompson, A. J. & Turner, A. J. A Comparison of the EQ-5D-3L and EQ-5D-5L. PharmacoEconomics 38, 575–591 (2020).
Manca, A., Hawkins, N. & Sculpher, M. J. Estimating mean QALYs in trial-based cost-effectiveness analysis: the importance of controlling for baseline utility. Health Econ. 14, 487–496 (2005).
Little, M. et al. Five-year costs from a randomised comparison of bilateral and single internal thoracic artery grafts. Heart 105, 1237–1243 (2019).
NHS England. Post-COVID syndrome (long COVID) (2021) (Accessed 14 September 2024). Available from https://www.england.nhs.uk/coronavirus/post-covid-syndrome-long-covid/.
NICE. The reference case: Guide to the methods of technology appraisal (2013) (Accessed 12 August 2022). Available from https://www.nice.org.uk/process/pmg9/chapter/the-reference-case.
Husereau, D. et al. Consolidated health economic evaluation reporting standards (CHEERS) 2022 explanation and elaboration: a report of the ISPOR CHEERS II good practices task force. Value Health 25, 10–31 (2022).
The EuroQol Group. EuroQol-a new facility for the measurement of health-related quality of life. Health Policy 16, 199–208 (1990).
Janssen, M. F. P. A. et al. Measurement properties of the EQ-5D-5L compared to the EQ-5D-3L across eight patient groups: a multi-country study. Qual. Life Res 22, 1717–1727 (2013).
Hernández Alava, M., Pudney, S. & Wailoo, A. Estimating the relationship between EQ-5D-5L and EQ-5D-3L: results from a UK population study. PharmacoEconomics 41, 199–207 (2023).
Curtis, L. & Burns, A. Unit Costs of Health and Social Care 2019. (Personal Social Services Research Unit, University of Kent, 2019).
Goodman, C. et al. Optimal NHS service delivery to care homes: a realist evaluation of the features and mechanisms that support effective working for the continuing care of older people in residential settings. Health Serv. Deliv. Res. 5, 242 (2017).
Jones, K. C. et al. Unit Costs of Health and Social Care 2022 Manual. Personal Social Services Research Unit (University of Kent) & Centre for Health Economics (University of York, 2023).
National Health Service. National Schedule of NHS Costs 2021/22. (Accessed 20 September 2023). Available from https://www.england.nhs.uk/publication/2021-22-national-cost-collection-data-publication/ (2023).
Guest, J. F., Keating, T., Gould, D. & Wigglesworth, N. Modelling the annual NHS costs and outcomes attributable to healthcare-associated infections in England. BMJ Open 10, e033367 (2020).
National Statistics. Scottish Health Service Costs. (National Services Scotland: Information Services Division, 2019).
Francis-Devine, B. Average earnings by age and region. Commons Library. (Accessed 16 August 2024). Available from https://commonslibrary.parliament.uk/research-briefings/cbp-8456/ (2024).
Office for National Statistics. Employee earnings in the UK. (Accessed 16 August 2024). Available from https://www.ons.gov.uk/employmentandlabourmarket/peopleinwork/earningsandworkinghours/bulletins/annualsurveyofhoursandearnings/2023 (2023).
Joint Formulary Committee. British National Formulary. (BMJ and Pharmaceutical Press).
British National Formulary (BNF). The unrivalled guidance on prescribing, dispensing, and administering medicines. MedicinesComplete (Accessed: 11 October 2023). Available from https://about.medicinescomplete.com/publication/british-national-formulary/
Reilly, M. C., Zbrozek, A. S. & Dukes, E. M. The validity and reproducibility of a work productivity and activity impairment instrument. PharmacoEconomics 4, 353–365 (1993).
Faria, R., Gomes, M., Epstein, D. & White, I. R. A guide to handling missing data in cost-effectiveness analysis conducted within randomised controlled trials. Pharmacoeconomics 32, 1157–1170 (2014).
Simons, C. L., Rivero-Arias, O., Yu, L.-M. & Simon, J. Multiple imputation to deal with missing EQ-5D-3L data: should we impute individual domains or the actual index? Qual. Life Res 24, 805–815 (2015).
Ben, Â. J. et al. Conducting trial-based economic evaluations using r: a tutorial. PharmacoEconomics 41, 1403–1413 (2023).
Henningsen, A. & Hamann, J. D. systemfit: a package for estimating systems of simultaneous equations in R. J. Stat. Softw. 23, 1–40 (2008).
Fenwick, E. & Byford, S. A guide to cost-effectiveness acceptability curves. Br. J. Psychiatry 187, 106–108 (2005).
R Core Team. R: A Language and Environment for Statistical Computing. Version 4.4.1 (2024-06-14 ucrt). Available from https://www.R-project.org/ (R Foundation for Statistical Computing, 2024).
Posit Team. RStudio: Integrated Development Environment for R. Version 2024.04.2-764. Available from https://posit.co/products/open-source/rstudio/ (Posit Software, PBC, 2024).
Angelo, C. & Ripley, B. D. boot: bootstrap R (S-Plus) functions. R package version 1.3-30. https://CRAN.R-project.org/package=boot
Barrett, T. et al. data. table: Extension of ‘data.frame’. R package version 1.16.0. https://CRAN.R-project.org/package=data.table (2024).
Bates, D., Mächler, M., Bolker, B. & Walker, S. Fitting linear mixed-effects models using lme4. J. Stat. Softw. 67, 1–48 (2015).
Comtois, D. summarytools: tools to quickly and neatly summarize data. R package version 1.0.1. https://CRAN.R-project.org/package=summarytools (2022).
FC, M. & Davis, T. L., ggplot2 authors. ggpattern: ‘ggplot2’ Pattern Geoms. R package version 1.1.4. https://CRAN.R-project.org/package=ggpattern (2025).
Garbuszus, J. M. & Jeworutzki S. readstata13: import ‘stata’ data files. R package version 0.10.1. https://CRAN.R-project.org/package=readstata13 (2023).
Garnier, S. et al. viridis(Lite) - colorblind-friendly color maps for R. package version 0.6.5. Available from https://sjmgarnier.github.io/viridis/ (2024).
Gohel, D. & Skintzos, P. flextable: functions for tabular reporting. R package version 0.9.6. Available from https://CRAN.R-project.org/package=flextable (2024).
Harrison, E., Drake, T. & Pius, R. finalfit: quickly create elegant regression results tables and plots when modelling. R package version 1.0.8. https://CRAN.R-project.org/package=finalfit (2024).
Højsgaard, S. & Halekoh, U. DoBy: groupwise statistics, lsmeans, linear estimates, utilities. R package version 4.6.22. https://CRAN.R-project.org/package=doBy (2024).
Kassambara A. ggpubr: ‘ggplot2’ based publication ready plots. R package version 0.6.0. https://CRAN.R-project.org/package=ggpubr (2023).
Kremer, L. P. M. ggpointdensity: a cross between a 2D density plot and a scatter plot. R package version 0.1.0. https://CRAN.R-project.org/package=ggpointdensity (2019).
Morton, F. & Nijjar, J. S. eq5d: methods for analysing ‘EQ-5D’ data and calculating ‘EQ-5D’ index scores. R package version 0.15.3. https://CRAN.R-project.org/package=eq5d (2024).
Rich, B. Table 1: tables of descriptive statistics in HTML. R package version 1.4.3. https://CRAN.R-project.org/package=table1 (2023).
Robitzsch, A. & Grund, S. miceadds: some additional multiple imputation functions, especially for ‘mice’. R. package version 3, 17 Available from https://CRAN.R-project.org/package=miceadds (2024).
Sjoberg, D. D., Whiting, K., Curry, M., Lavery, J. A. & Larmarange, J. Reproducible summary tables with the gtsummary package. R. J. 13, 570–580 (2021).
Wickham, H. Reshaping data with the reshape package. J. Stat. Softw. 21, 1–20 (2007).
Wickham, H. et al. Welcome to the tidyverse. J. Open Source Softw. 4, 1686 (2019).
Wickham, H., Hester, J., Chang, W. & Bryan, J. devtools: Tools to Make Developing R Packages Easier. R package version 2.4.5. https://CRAN.R-project.org/package=devtools (2022).
Wickham, H., Pedersen, T. L. & Seidel, D. Scales: scale functions for visualization. R package version 1.3.0. https://CRAN.R-project.org/package=scales (2023).
Allaire, J. J. et al. rmarkdown: dynamic documents for R. R package version 2.28. https://github.com/rstudio/rmarkdown (2024).
Zhu, H. kableExtra: construct complex table with ‘kable’ and pipe syntax. R package version 1.4.0. https://CRAN.R-project.org/package=kableExtra (2024).
Combet, E., Blane, D. & Haag, L. ReDIRECT study eCRF questionnaires screenshots. figshare. https://figshare.com/articles/online_resource/ReDIRECT_study_eCRF_questionnaires_screenshots/21270837/4 (2022).
Acknowledgements
The authors thank the National Health Service (NHS Greater Glasgow and Clyde) sponsor representatives, project management unit staff, Robertson Centre for Biostatistics and ReDIRECT Trial Steering Committee members for their support. The authors are also grateful to Long COVID Scotland and patient representatives in the PPI group for constructive discussions about the protocol, data acquisition and interpretation. The authors thank all ReDIRECT study participants for their participation in research. This study (COV-LT2-0059 DB) was funded by the National Institute for Health and Care Research (NIHR) in response to the COVID-19 pandemic. The views expressed are those of the authors and not necessarily those of the NIHR or the Department of Health and Social Care. The study’s funder had no role in study design, data collection, analysis, interpretation or report writing. The corresponding authors had final responsibility for the decision to submit for publication.
Author information
Authors and Affiliations
Contributions
E.C. and D.N.B. are the principal investigators of the study, with E.M. the principal health economist of the study. The study was conceptualised by E.C., D.N.B., M.L., A.M., E.M., C.A.O., J.O., N.S. and T.I. All authors contributed to the methodology. L.H. and J.R. coordinated the recruitment and quantitative data acquisition, supervised by E.C. and D.N.B. Processing and quality assurance of quantitative data was conducted by C.H., supervised by A.M., and N.B. coordinated Counterweight data acquisition. H.L.F. carried out formal analysis and data visualisation, supervised by E.M. H.L.F. wrote the original draft, which was reviewed by all authors. All authors had full access to all draft versions and supplementary materials and had final responsibility for the decision to submit for publication.
Corresponding author
Ethics declarations
Competing interests
N.B. is an employee and shareholder of Counterweight Ltd., subcontracted to the University of Glasgow to deliver the ReDIRECT intervention. A.M. is a member of Clinical Steering Committee for ARC Medical Inc. N.S. has received institutional grant support from AstraZeneca, Boehringer Ingelheim, Novartis, Roche Diagnostics and honoraria from Abbott Laboratories, AbbVie, Afimmune, Amgen, AstraZeneca, Boehringer Ingelheim, Eli Lilly, Hanmi Pharmaceuticals, Janssen, Menarini-Ricerche, Merck Sharp & Dohme, Novartis, Novo Nordisk, Pfizer, Roche Diagnostics, Sanofi. M.L. has received lecturing fees from Novo Nordisk, Lilly, Nestle, Oviva, Merck, and Sanofi and is a medical advisor to Counterweight Ltd, with fees paid to the University of Glasgow. The remaining authors declare no competing interests.
Peer review
Peer review information
Nature Communications thanks Marcia Weaver and the other, anonymous, reviewer(s) for their contribution to the peer review of this work. A peer review file is available.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Source data
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Fraser, H.L., Haag, L., Brosnahan, N. et al. Cost-effectiveness of the ReDIRECT/counterweight-plus weight management programme to alleviate symptoms of long COVID. Nat Commun 16, 5592 (2025). https://doi.org/10.1038/s41467-025-59909-6
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41467-025-59909-6
