
Abstract
Psychosis progresses along a continuum. While heterogeneity is evident across the continuum, it remains unknown whether this is also reflected in white matter (WM) heterogeneity and whether parsing WM heterogeneity may reveal subgroups with more pronounced clinical features. This analysis included 212 participants consisting of healthy controls (HC, n = 59), individuals with high schizotypy (SPT, n = 27), at-risk mental state (ARMS, n = 35), and patients with first episode psychosis (FEP, n = 50) and schizophrenia (SZ, n = 41). Fractional anisotropy (FA) and mean diffusivity (MD) were derived from diffusion tensor imaging (DTI), and fibre density (FD), a non-tensor-derived diffusion marker, was computed. The Person-Based-Similarity Index (PBSI) and Coefficient of Variation Ratio (CVR) were computed to assess global and local heterogeneity. ANOVAs were performed to determine whether people with deviating PBSIs exhibit more pronounced clinical features. Global heterogeneity for all diffusion parameters significantly differed across groups, with greatest difference in heterogeneity between SZ and HC. Results further indicate that FA deviators exhibit lower global functioning and higher negative symptoms. Local FA heterogeneity was greater in FEP relative to ARMS and HC in almost all WM tracts, while SZ patients specifically showed greater heterogeneity in the right thalamic radiation and the left uncinate compared to HCs. Group differences in WM heterogeneity might be indicative of symptom specificity and duration. While these findings offer valuable insights into the neurobiological variability of psychosis, they are primarily hypothesis-generating. Future large-scale studies are warranted to test the robustness of diffusion markers and their clinical relevance.
Similar content being viewed by others

Introduction
Acute psychosis is greatly debilitating, and amongst the highest weighted global burdens of disease1. Psychosis occurs along a continuum ranging from stages with subclinical psychotic like experiences in healthy subjects from the general population (e.g., people with schizotypy) and individuals at clinical high-risk for psychosis (CHR), not bound to transition2,3, and further to patients with first-episode psychosis (FEP) and schizophrenia (SZ)4. This classification into stages primarily enabled diagnosis and has advanced our understanding of pathogenesis and aetiology5, yet psychosis is regarded as inherently heterogeneous in symptom presentation, functioning and treatment response6. Clinical heterogeneity is apparent at each stage across the psychosis continuum6,7,8 and accompanied by heterogeneity in brain structure as well as function9. Dissecting brain heterogeneity within and across stages on the continuum may help to identify more homogeneous subgroups with common clinical manifestations and in turn enhance preventive treatment responses and outcomes to more targeted interventions, proportionate to clinical need10.
Magnetic resonance imaging (MRI) has become an important non-invasive tool, supporting our understanding of structural brain abnormalities in psychosis and their respective symptom expression11, with evidence for whole-brain grey matter (GM) alterations at each stage across the psychosis continuum. However, such mean group comparisons did not establish any reliable neuroanatomical biomarkers, probably because case-control analyses do neglect within-group variability12,13. Seminal works addressed this gap by first exploring interindividual variability of regional grey matter volume (GMV) in schizophrenia. Brugger and Howes investigated the variability of regional GMV by utilising the log variability ratio (VR) and log coefficient of variation ratio (CVR) and found significant differences in the variability of regional GM in SZ patients14. Later studies, utilising the CVR, consistently reported greater cortical and subcortical volume heterogeneity in SZ patients referenced to controls15, yet report no significant regional heterogeneity difference in CHR relative to a healthy control (HC) sample in structural MRI measures of cortical surface are (SA), cortical thickness (CT), and subcortical volume (SV)16.
The Person-Based-Similarity Index (PBSI) has recently been introduced as an index of global brain heterogeneity, with the advantage of returning personalised estimates of the degree of similarity of single individuals to the normative reference or within the group17. By utilising the PBSI as a personalised metric to investigate inter-subject correlation, a greater within-group variability (lower PBSI scores) in CHR subjects compared to HCs was confirmed for SA, CT, and SV16. Antoniades et al.18 further showed that relative to HCs, CHR individuals and FEP patients also revealed a lower PBSI for CT, SA and SV. Moreover, they could also show that individuals with deviating PBSI scores had lower IQ and higher psychopathology18, indicating the potential of normative models to identify individuals with more prominent clinical manifestations13.
Diffusion tensor imaging (DTI) studies demonstrated widespread white matter (WM) microstructural differences in SZ. The largest study so far, conducted in 4322 patients, reported reduced fractional anisotropy (FA) and increased mean diffusivity (MD) across all major WM fasciculi19. Previously, we also showed that a new, non-tensor-derived diffusion marker, the measure of fibre density (FD), may be more sensitive to subtle changes in WM microstructure compared to FA in SZ20. Such deficits in WM integrity have been reported in early psychosis21,22,23 and related to a number of affective, cognitive, and perceptual symptoms observed in psychosis,24,25,26 as well as to treatment response27. Recent works have focused on multimodal variability in patients28, however, to the best of our knowledge, no study has yet compared variability in WM integrity among different stages along the psychosis continuum.
In this study, we investigate global (via PBSI) and local (via CVR) heterogeneity differences in FA, MD, and FD among HCs, those with schizotypy and CHR, FEP and patients with SZ, and whether individuals with deviating PBSI score exhibited more pronounced clinical features. In line with previous works in FEP and CHR16,18 we predicted lower PBSI for all diffusion metrics in schizotypy, CHR, FEP and SZ compared to HCs and that deviators would express lower IQ and higher psychopathology. Furthermore, for subclinical stages on the psychosis continuum29, hence schizotypy and CHR, we further anticipated increased regional heterogeneity compared with HC in the corpus callosum26,30,31,32,33, bilateral anterior corona radiata, the bilateral thalamic radiation, and the left superior fronto-occipital fasciculus26, and expect these effects predominantly in FA due to its suggested early-stage-specificity26,34,35. In later stages of clinical progression (i.e. FEP and SZ patients), we expect to see increased heterogeneity in callosal and commissural fibre tracts and fronto-temporal-limbic pathways36.
Methods
This is an ad-hoc multisite analysis of previously conducted site-specific investigations in ARMS24,37, SPT38, FEP20,24, and SZ20,39. Here, we report pooled findings on global (using the PBSI) and local heterogeneity (using CVR) in WM integrity across the different stages along the psychosis spectrum.
Participants
Data of 212 participants collected at three different centres was included. Datasets were collected at the Department of Psychiatry (UPK) of the University of Basel, the University Hospital of Psychiatry, Bern and the Department of Psychiatry, Psychotherapy and Psychosomatics at the Psychiatric Hospital, University of Zurich. All participants provided written and informed consent, and the study was approved by the respective local ethics committees. Samples ranging from five different stages along the psychosis continuum were included in the study: 59 HC, 35 ARMS, 27 SPT, 50 FEP patients, and 42 patients with SZ.
The Basel sample consisting of ARMS (n = 35) and FEP (n = 36) was recruited in an open prospective clinical study for the Early Detection of Psychosis (FePsy)40. ARMS subjects were recruited according to the Personal Assessment and Crisis Evaluation (PACE)24 and the “Basel Screening Instrument for Psychosis” (BSIP)41, a screening checklist for help seeking populations which is performed by experienced psychiatrists and consists of similar criteria to the Comprehensive Assessment of ARMS questionnaire42.
FEP patients from the Basel sample fulfilled the criteria for first-episode psychosis according to the ICD-10 or DSM-IV43 but not yet for schizophrenia37,44. Inclusion criteria were scores of 4 or above on the hallucination item, of 5 or above on the unusual thought content, suspiciousness or conceptual disorganisation items, from the Brief Psychiatric Rating Scale (BPRS)37,45. The symptoms had to have occurred multiple times and persisted for more than one week37. At the time of scanning, ten of the included 36 FEP patients from the Basel sample were receiving antipsychotic treatment, five were receiving antidepressant treatment and six receiving both of unknown duration. Twelve FEP patients received neither (missing data for 3 patients).
The SZ patients from Bern (n = 21) came from the SWIFT-study and were diagnosed with schizophrenia spectrum disorder according to the DSM-IV-TR criteria39,46,47. The diagnoses were confirmed by an experienced clinician and the Mini International Neuropsychiatric Interview (MINI)39,48. Further inclusion criteria for patients were age between 18 and 65 years, sufficient fluency in German and right handedness39,47. Exclusion criteria entailed left-handedness, pregnancy, history of serious neurological issues, or reported current abuse of alcohol and/or psychoactive substances apart from nicotine39.
The Zurich sample consisted of FEP patients (n = 14) who were recruited during their first psychiatric admission in outpatient and inpatient units of the Psychiatric Hospital of the University Zurich. The inclusion criterion of a diagnosis of brief psychotic disorder, schizophreniform disorder or schizophrenia was confirmed in a structured Mini-International Neuropsychiatric Interview for DSM-IV (MINI)38,48. All FEP patients from the Zurich sample received a stable dose of second-generation antipsychotics38,49. Healthy individuals with high SPT (n = 27) were recruited using an online form of the Schizotypal Personality Questionnaire (SPQ)50. Out of 956 participants who completed the questionnaires, the individuals scoring highest (upper 10% of maximum SPQ score) were included in the study38,49. SZ patients (n = 20) from the Zurich sample were assessed with the structured MINI in accordance with DSM-IV criteria20,38,39. Patients with any other Axis I DCM-IV disorder, such as current substance use disorder or major depression were excluded from the study20. All included patients with SZ received a stable dose of second-generation antipsychotic, with no change in medication or dose for at least two weeks and were clinically stable20.
HCs were recruited from the same geographical areas as the other groups and data collected across all sites. They had no history of psychiatric illness, head trauma, neurological illness, serious medical or surgical illness, substance abuse, and no family history of any psychiatric disorders, which was assessed in a detailed semi-structured interview20,24,37,38,39.
Detailed demographic and clinical characteristics of all groups can be found in Table 1. There were significant differences in age (p = 0.003) and sex (p = 0.026) between the five groups. Therefore, both variables were modelled as covariates in the residualisation of the diffusion data and controlled for in all subsequent statistical analyses.
Image acquisition and preprocessing of diffusion derived data
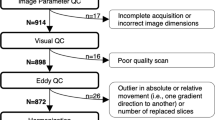
Details of diffusion imaging sequences can be found in the supplement (Supplementary Table 1). Data quality assessment and preprocessing were performed as previously done and described in detail20 (see supplement). The quality inspection resulted in the exclusion of 10 subjects (2 HC, 3 ARMS, 5 FEP). From the resulting preprocessed datasets, the fractional anisotropy (FA) and mean diffusivity (MD) tensor related measures were derived using the FSL software package. Furthermore, fibre density (FD), a non-tensor-derived diffusion marker, measure was calculated as previously described in detail20. Preprocessing has been performed as previously described20,26,39 (for details see supplement).
Harmonisation
Site-related differences in the FA, MD, and FD measurements were controlled with the ComBat harmonisation technique which has shown to remove unwanted variation in DTI data induced by site51. Diffusion imaging data were harmonised prior to heterogeneity analyses controlling for age, sex, and group. ComBat was first developed as a batch adjustment method for genomics data52 and later adapted by Fortin et al.51 in the context of DTI images. The generalised ComBat model has demonstrated to successfully reduce inter-site effects for voxels in the FA, MD, and FD maps and fully remove site effects for all regions of interest (ROIs). They further showed that the use of Empirical Bayes implemented in ComBat improved the estimation and removal of site-effects, making this approach especially robust to harmonise data, whilst preserving the between-subject variability in small sample size studies51. The ComBat harmonisation was implemented in R using the software provided on GitHub (https://github.com/Jfortin1/ComBatHarmonization).
To further account for potentially persisting confounding effects of scanner, age, and sex on the diffusion parameters, residualisation as described in previous studies53,54 was performed (for details see supplement).
Calculation of global heterogeneity
The PBSI is a validated method which allows for quantification of individual neuroimaging profiles and their similarity to those of other members of their group17,55,56. A three-step procedure was used to derive PBSI scores by collapsing all WM tracts and creating FA, MD, and FD profiles for each subject. Subsequently interindividual Spearman’s correlation coefficients were calculated between each of the subjects and the respective profile of the other subjects. Lastly the n-1 interindividual correlation coefficients (n referring to the number of subjects in each sample) were averaged separately resulting in one PBSI score with a maximum of 1 per participant17,55,56. The higher the PBSI score the greater the similarity between the diffusion parameter (FA, MD, or FD) profiles of the subject with those of the same sample. The MATLAB function used to compute the PBSI scores is available at: https://www.mathworks.com/matlabcentral/fileexchange/69158-similarityscore57:
In this study the PBSI scores were computed separately for FA, MD, and FD maps to generate a person-specific neuroimaging profile in correspondence to profiles of members of the same group (PBSI, within-group reference) and individually in reference to the neuroimaging profile of a normative reference group regardless of continuum stage (nPBSI, normative reference). The respective scores provide an estimate of the similarity of the individual neuroimaging profiles indicating the degree of heterogeneity within the groups (PBSI) and in reference to the norm (nPBSI).
Within-group reference
The PBSIFA, PBSIMD and PBSIFD were calculated separately for the five groups (HC, ARMS, FEP, SPT and SZ) representing the degree of within-group profile similarity. For each individual group the three-step procedure of calculating PBSI were performed. The higher the PBSI score the greater the similarity in the neuroanatomical profile of the individual respective to its group. The within-group reference represents the level of heterogeneity of each individual to other members of the same group.
Normative reference
To quantify the similarity of the individuals’ neuroanatomical profile respective to a normative estimate the nPBSIFA, nPBSIMD, and nPBSIFD scores were calculated for each individual subject from the four clinical groups (ARMS, FEP, SPT, SZ) in correlation with the corresponding profiles of the control group (HC). The nPBSI scores resulting from three-step procedure indicate the degree of deviation from the normative range16.
Statistical analysis of global heterogeneity
Differences of PBSIFA, PBSIMD, and PBSIFD scores between the five groups were assessed using analysis of variance (ANOVA) and Welch’s test proven to be robust for unequal sample sizes58,59. Statistically significant results were followed up with post-hoc pairwise comparisons to examine differences between specific groups.
The nPBSI scores for FA, MD, and FD of each group were converted into z-scores (z-nPBSI) representing the deviation from the mean of the healthy control group (PBSI-HC). To identify the deviators from the norm the threshold of ±1.5 SD was applied16,18. To determine whether the number of deviators differed between the groups, for each diffusion parameter Fishers’s exact test was performed, and the odds ratio (OR) determined for effect size. T-tests were performed to compare clinical measures between deviators and non-deviators and Mann–Whitney U used to examine the effect of group specific deviators. Subsequently Pearson’s correlation coefficients were calculated to evaluate correlations between deviators and non-deviators with crystallised intelligence (IQ), global functioning (GAF) and clinical scores (SANS, BPRS). This correlation was computed separately for every parameter (FA, MD, and FD) and overall measures (IQ, GAF, SANS & BPRS). To account for multiple comparisons, all p-values were adjusted using false discovery rate; when uncorrected P values are shown these are denoted as punc. All statistical analyses were conducted using R Studio (version 2023.03.0) within the R programming environment (version 4.1.2 and 4.3.1).
Calculation of local heterogeneity
For each parameter and WM tract the coefficient of variation ratio (CVR) was computed across groups to estimate differences in local heterogeneity. We used the escalc() function in R60 to apply the log-CVR function as a mean-scaled variability measure of diffusion parameters between two groups. It is calculated using the following formula:
where xp and xc indicate the reported means for the clinical (ARMS, FEP, SPT, and SZ) and control (HC) group, respectively; the \({\hat{\sigma }}_{p}\) and \({\hat{\sigma }}_{c}\) indicate the unbiased estimates of population SDs; Sp and Sc represent the reported sample SDs; np and nc are the sample sizes. Next, the difference in variability was computed in the same manner between the groups FEP vs. SZ, and ARMS vs FEP. The log CVR was back-transformed into the original scale in order to simplify the interpretation of the results. A CVR of 1 indicates equal variability of diffusion parameters in the WM tracts between the groups, whereas a CVR < 1 indicates a smaller variability in the control group, and CVR > 1 indicates a greater variability in the more symptomatic group, when compared to a less symptomatic group. The results are shown in forestplots (see Figs. 1 and 2 and Supplementary Figs. 2–16), showing the corrected as well as the uncorrected p-values. For p-value adjustment, we used the False Discovery Rate (FDR) method.

Person-based-similarity-index (PBSI) for fractional anisotropy (A), mean diffusivity (B), and fibre density (C) in healthy controls (HC), at-risk-mental-state (ARMS), schizotypy (SPT), first-episode psychosis (FEP), and schizophrenia (SZ). ANCOVA analysis controlling for age and sex followed up by estimated marginal means (EMMs) for pairwise-comparisons, * <0.05, ** <0.01, *** <0.001 = sign. after FDR correction.

Bar chart representing the percentage of individuals within the individual groups (HC, ARMS, SPT, FEP & SZ) who demonstrate marked deviation of the person-based similarity index cortical thickness z-scores from the ‘normative’ neuroanatomical profile (±1.5 SD), per parameter and overall (A). Bar chart representing the percentage of deviators accounted for by individual groups relative to group size, per parameter and overall (B).
Results
Group differences in global heterogeneity
Across groups significant PBSI differences were found for all three diffusion measures FA (F (1,4) = 5.33, p < 0.001), MD (F (1,4) = 6.61, p < 0.001), and FD (F (1,4) = 4.91, p = 0.001). Specific group differences in PBSIFA were found to be most pronounced between SZ-HC (t = −4.37, p = <0.001), SZ-ARMS (t = −3.016, p = 0.012), FEP-HC (t = −2.93, p = 0.012), and SPT-HC (t = −2.39, p = 0.045) (Fig. 1A). For PBSIMD, significant differences were found between SZ-HC (t = −3.85, p < 0.001), SZ-FEP (t = −3.96, p < 0.001), FEP-ARMS (t = 3.92, p < 0.001), ARMS-HC (t = −3.80, p < 0.001) (Fig. 1B). For PBSIFD differences were found between SZ-HC (t = −3.96, p = 0.001), SZ-ARMS (t = −3.35, p = 0.005), SZ-FEP (t = −3.06, p = 0.006), SPT-HC (t = −3.08, p = 0.006), SPT-ARMS (t = −2.47, p = 0.029), and trends were found between FEP-SPT (t = 2.18, p = 0.051) (Fig. 1C). For details on group comparisons see Supplementary Table 2.
Normative referencing of global heterogeneity
Over all three parameters the number of deviators differed significantly across the groups (\({\chi }^{2}\) = 11.86, df = 4, p = 0.018). Subsequent post-hoc comparisons revealed significant differences between the groups SZ-HC (OR = 3.78, p = 0.006), SZ-FEP (OR = 2.74, p = 0.041), and ARMS-HC (OR = 3.22, p = 0.016), yet notwithstanding correction for multiple comparisons.
Within group, SZ showed the greatest percentage of deviators (31.71%) followed by ARMS (22.86%), SPT (22.22%), FEP (20.00%), and HC (11.86%) for FA. For MD, 22.50% deviators were found in SZ, 22.86% in ARMS, 11.11% in SPT, 10.00% in FEP, and 5.09% in HC. And for FD 22.22% in SPT, 20.00% in FEP and ARMS, 17.07% in SZ, and 13.79% in HC (Fig. 2A).
Across all groups SZ accounted for the most deviators (29.55%) followed by FEP (22.73%), ARMS (18.18%), HC (15.91%), and SPT (13.64%) for FA. For MD most deviators were accounted for by SZ (32.14%) followed by ARMS (28.57%), FEP (17.86%), SPT (10.71%), and HC (10.71%). And for FD 26.32% in FEP, followed by 21.05% in HC, 18.42% in SZ and ARMS, and 15.79% in SPT (Fig. 2B).
Further, for nPBSIMD a significant difference in the number of deviators (\({\chi }^{2}\) = 9.76, df = 4, p = 0.041) was discovered across all groups. Subsequent post-hoc comparisons revealed differences between SZ-HC (OR = 5.32, p = 0.013), and ARMS-HC (OR = 5.42, p = 0.017), again notwithstanding correction for multiple comparisons. For for nPBSIFA (\({\chi }^{2}\) = 5.97, df = 4, p = 0.188), and nPBSIFD (\({\chi }^{2}\) = 1.28, df = 4, p = 0.847) no significant differences in deviators from the norm were detected.
Deviation from the normative reference and clinical implications
The analysis of the relationship between being a deviator (vs non-deviator), crystallised intelligence (IQ), generalised functioning (GAF) and psychopathology (SANS, BPRS) underpins the connection between FA deviators in GAF (t = 2.64, punc = 0.009) and SANS (t = −2.43, punc = 0.016), indicating towards lower GAF scores, and higher SANS scores in FA deviators (Fig. 3B). However, these results are notwithstanding correction for multiple comparisons. No significant correlation for deviators in specific parameters and clinical features could be found for the other measures.

Deviators vs. non-deviators for nPBSIFA, nPBSIMD, and nPBSIFD, and overall parameters in general ability of functioning (GAF) (A), and scale for the assessment of negative symptoms (SANS) (B) scores.
Group differences in local heterogeneity
Only the FDR-corrected statistically significant between-group differences in local heterogeneity will be reported here.
Fractional anisotropy (FA)
As illustrated in Fig. 4A, FEP showed a greater heterogeneity in all WM tracts, except both corticospinal, both cingulum cingulate, left cingulum hippocampus and left arcuate WM tracts, when compared to HC. SZ showed a greater heterogeneity in the right thalamic radiation and the left uncinate WM tract (Fig. 4B), when compared to HC. Also, FEP showed greater heterogeneity than ARMS in all WM tracts, besides the left corticospinal tract. The comparisons of HC vs. ARMS, HC. vs. SPT, and FEP vs. SZ did not show any differences in CVR in any WM tracts when compared to HC (Supplementary Figs. 2–5).

Forest plots of the coefficient of variation ratio (CVR) of fractional anisotropy (FA) between (A) healthy controls (HC) and first episode psychosis (FEP), and (B) between HC and diagnosed schizophrenia (SZ). Colour gradient indicating CVR effect sizes transformed into z-scores for the individual tracts.
Mean diffusivity (MD)
FEP showed greater heterogeneity in the left cingulum hippocampus and the right thalamic radiation WM tract, when compared to HC. Also, SZ showed greater heterogeneity in the right thalamic radiation WM tract than the HC group. There were no effects in ARMS vs. HC, MD for FEP vs. ARMS, SPT vs. HC and FEP vs. SZ in any WM tracts (Supplementary Figs. 6–11).
Fibre density (FD)
None of the local heterogeneity group comparisons showed any statistically significant differences in any of the WM tracts after FDR-correction (Supplementary Figs. 12–16).
Discussion
This study revealed four major findings: firstly, global heterogeneity significantly differed across groups and diffusion parameters. The greatest difference in global heterogeneity was apparent between SZ and HC across all three diffusion parameters. ARMS additionally showed greater heterogeneity in MD relative to HC, SPT, and FEP, yet not SZ, whereas in FA and FD, ARMS differed from SZ. SPT revealed to differ markedly from SZ (FA), ARMS, and SZ (MD), as well as ARMS and HC (FD), yet not FEP. Secondly, the number of deviators differed significantly between groups for MD but not for FA and FD. In particular, MD deviators were highest in SZ (9), followed by FEP (5), ARMS (8), HC (3), and SPT (3) relative to sample size. Thirdly, deviators in FA indicated towards lower GAF, and higher SANS scores, respectively. Finally, greater local heterogeneity (i.e. CVR) in FA was found in almost all WM tracts in FEP relative to HC and ARMS, while SZ patients showed greater local heterogeneity specifically in the right thalamic radiation and the left uncinate when compared to HCs. For MD and in relation to HC, FEP, and SZ patients revealed greater heterogeneity in the right thalamic radiation, and FEP additionally in the left cingulum hippocampus. Differences in WM heterogeneity was observed in global and local measures for all explored diffusion parameters across the psychosis continuum.
Global within-group heterogeneity across groups
The analysis of PBSI scores revealed significant global within-group heterogeneity, particularly in the SZ group, and highlighted marked differences between SZ-HC, SZ-ARMS, FEP-HC, and SPT-HC. PBSIFD showed similar patterns but also indicated greater heterogeneity between SPT and ARMS, as well as HC, while FEP did not differ significantly from HC and ARMS. In contrast, PBSIMD revealed higher heterogeneity in ARMS and SZ compared to HC, with additional differences observed between SPT-ARMS, SPT-SZ, and FEP-ARMS, FEP-SZ (Fig. 1).
ARMS and clinical implications
The lack of PBSIFA differences in the ARMS group aligns with previous studies reporting no significant mean FA differences between HC and ARMS23,26. However, evidence suggests that at-risk individuals who convert to full-blown psychosis often show reduced FA, potentially contributing to variability23,26,61. In this study, the small sample size and number of converters (n = 6, mean follow-up of 3.8 years) limited the ability to conduct a meaningful subanalysis.
Interestingly, while no reduction in PBSIFA was observed in ARMS, a reduction in PBSIMD was noted, corresponding to previously reported increases in MD23. This greater global heterogeneity in MD is consistent with recent studies showing that ARMS also exhibit lower PBSI scores for structural measures such as cortical thickness (CT), surface area (SA), and subcortical volume (SV)16,18. These findings suggest that the clinical heterogeneity in ARMS7 may be better reflected in increased global heterogeneity in MD or morphological metrics rather than in FA.
FEP and HC comparisons
The comparable PBSIMD and PBSIFD scores between HC and FEP are notable, especially given the significant reductions in mean FA62 observed in the FEP group. This finding is consistent with the lack of global heterogeneity in morphological metrics reported in patients with bipolar disorder56. It is possible that the global heterogeneity of diffusion markers in FEP patients56 may fall within the range of normal biological diversity, similar to the high prevalence of psychotic symptoms in the general population. However, this interpretation should be approached with caution, given the small sample size of our FEP group and the pronounced increases in local heterogeneity measures observed in FEP patients.
SZ, SPT, and clinical trajectories
The increased global heterogeneity across all diffusion parameters in SZ aligns with previous evidence of increased global heterogeneity in morphological metrics (SA, CT, SV)63,64 and expands the understanding of mean diffusion differences in SZ19,20,65. This increased heterogeneity may be attributed to the high clinical heterogeneity in SZ13. Similarly, SPT individuals showed greater global heterogeneity in FA and FD parameters compared to HC, mirroring the pattern observed in SZ66. Both SZ and SPT groups are characterised by highly variable longitudinal trajectories13,15,67, suggesting that dissecting variability in established diffusion measures could help identify subgroups of SPT and SZ patients with distinct clinical trajectories, ranging from more severe (e.g., reactive compensation or resilience) to milder (e.g., relapses) courses68.
Normative referencing for global heterogeneity
Despite significant differences in the number of normative heterogeneity deviators across the five groups, no statistically significant correlations were found between these deviations and verbal intelligence (IQ), global functioning (GAF), or clinical symptoms (SANS, BPRS) across all groups. As in previous studies69, symptom severity was not associated with deviations from the normative reference. However, consistent with prior research26,35 and our hypothesis, differences in the number of deviators, were observed for nPBSIMD, but not for nPBSIFA or nPBSIFD.
The investigation into the relationship between deviators from the ARMS and FEP groups with IQ and GAF scores, which have been suggested in earlier research on GMV heterogeneity18, did not reflect similar findings in white matter (WM) deviators. Nonetheless, the negative correlations observed between FA deviators and GAF scores are in line with findings by Antoniades et al.18, which linked higher psychopathology to deviators in individuals at clinical high risk (CHR) and those experiencing first-episode psychosis (FEP).
The observation of higher SANS scores in FA deviators aligns with previous research demonstrating a significant relationship between negative symptoms in CHR and multimodal changes in brain morphometry, including increased regional FA in CHR individuals who transitioned to psychosis70. A longitudinal follow-up study with the same individuals could help determine which parameters and respective PBSI scores and nPBSI deviators have the potential to serve as predictive indicators of disease risk.
Previous large-scale investigations into brain morphology (SA, CT, SV) did not find a link between deviations in CHR from a normative reference and psychopathology, nor did they associate these deviations with the transition to psychosis16. Similarly, another large-scale case-control study examining the same morphometric measures did not find an association between regional deviations and the severity of positive symptoms or IQ, suggesting that other structural metrics, such as DTI, may better distinguish between stages of psychosis71. Our findings indicate strong trends suggesting that FA deviators may differentiate individuals with schizophrenia (SZ) from healthy controls (HC), as well as those at ARMS and individuals experiencing FEP. While region-specific deviant DTI measures do not seem helpful for SZ-HC classification72, larger studies are needed to determine whether global diffusion heterogeneity can identify subgroups with common psychopathology.
In line with recent studies on GMV heterogeneity, we hypothesised that clinical measures such as IQ scores would positively correlate with PBSI scores64. Although white matter tract integrity has been shown to explain 10% of intelligence differences73, our sample did not show differences in IQ relative to their deviance status. This may be attributed to the nature of the IQ test (MWTB) used in this study, which lacks time constraints and thus does not account for information processing speed—a factor known to play a vital role in general functioning73. Consequently, more comprehensive evaluations of general functioning should be conducted in the future. The significant results indicating lower GAF scores in deviators suggest a link to general functioning, which could be further specified with more differentiated tests.
Local WM heterogeneity
On a local scale, the FA parameter exhibits the most statistically significant tract-specific differences in heterogeneity among group comparisons. Despite its previously demonstrated specificity for early-stage psychosis26,34,35, the FA parameter did not show statistically significant differences in local heterogeneity between HC-ARMS or HC-SPT, which are considered early stages on the psychosis risk continuum. Significant local differences in white matter (WM) heterogeneity were observed only between HC-FEP, HC-SZ, and ARMS-FEP.
The FEP group, which exhibited a greater number of WM tracts with significant heterogeneity compared to HC, contrasts with the SZ group, which showed fewer tracts with such distinctions. This discrepancy could potentially be explained by patterns of volume loss, particularly in the thalamus, where reductions in specific nuclei vary depending on the stage of disease progression74. For instance, medial nuclei reductions are suggested to occur earlier, while lateral nuclei impairments emerge at later stages. Consequently, the more widespread heterogeneity observed in FEP could result from the dynamic progression of psychopathology, with consistently changing symptoms, whereas SZ, representing a more stabilised disease state, may display less extensive heterogeneity.
The possibility that these differences are solely due to antipsychotic effects seems unlikely, as recent research has shown higher variability in WM tracts among individuals with FEP before the initiation of antipsychotic treatment75. The persistent FA abnormalities in SZ may indicate the presence of different schizophrenia subtypes. The higher prevalence of FA differences in heterogeneity, compared to MD and FD, aligns with previous research that reported the largest effect sizes for lower average FA in 80% of the investigated ROIs in schizophrenia19. While MD has been associated with increased values in patients, our findings suggest that the decrease in FA affects a broader range of WM tracts, while the increase in MD, occurring alongside changes in FD, follows a similar pattern but in fewer tracts19.
The lack of local heterogeneity differences between HC and ARMS is consistent with findings in GMV, where no regional differences in SA, CT, or SV heterogeneity were observed between HC and CHR16. Local variability differences may become evident only when symptom severity reaches the level of FEP, potentially allowing us to discern underlying biological processes that point to distinct biological subtypes14. The greater local WM heterogeneity observed in our study is consistent with previous research on grey matter heterogeneity, which suggests that collapsing patients with differing biological signatures into a single diagnostic group13 may lead to increased variability. Our results align with recent reports on structural GM heterogeneity, yet further investigation is needed to explore the potential of local heterogeneity as a marker for subtype delineation15.
Limitations
Although our study covered several stages on the psychosis risk spectrum more large-scale longitudinal studies are required to ascertain how WM heterogeneity can differentiate between underlying subtypes.
The small sample size relative to the number of centres may have introduced scanner effects that COMBAT harmonisation could not fully address, and had to be further residualised for differences in HC across scanners, which should be considered when interpreting the results. Although images with significant motion artifacts were excluded, the greater variability observed in the patient and psychosis risk groups might still reflect residual movement-related noise. Additionally, since the groups were not evenly distributed across scanners, the results should be interpreted with caution. As this was a post-hoc study, we were able to include some common measures of crystallised intelligence, global functioning, and psychopathology, yet due to sample size constraints and missing data we could not draw conclusions regarding medication. More homogeneous and comprehensive cognitive test batteries, comprehensive information of medication, and clinical evaluation across all groups are required to yield conclusive results on the effects of WM heterogeneity on clinical symptoms. More data driven studies would allow for an unconfined subgroup analysis and normative modelling which hold the potential for predictive risk assessments, and thus could inspire novel paths to disease prevention.
Conclusion
This study highlights differences in global and local white matter heterogeneity across the psychosis continuum, with the most pronounced differences observed between schizophrenia (SZ) and healthy controls (HC) for all diffusion parameters. The number of deviators in mean diffusivity (MD) differed significantly across groups, with SZ exhibiting the highest number. Local heterogeneity in white matter tracts was particularly notable in FEP and SZ, indicating potential variations in disease trajectories. These findings support the heuristic framework of staging models which emphasise that the developmental trajectory of psychosis is neither fixed nor linear10 and underscore the importance of considering global and local variability in understanding psychosis-related brain changes. While these findings offer valuable insights into the neurobiological variability of psychosis, they are primarily hypothesis-generating for future research. Larger samples and more comprehensive cognitive assessments are needed to validate these observations and explore potential clinical subtypes.
Data availability
The data that support the findings of this study and code to reproduce the results shown in the paper are available from the corresponding author upon reasonable request. We used R version 4.1.2 and 4.3.1.
References
Collaborators GBDMD. Global, regional, and national burden of 12 mental disorders in 204 countries and territories, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet Psychiatry 9, 137–150 (2022).
Grant, P., Green, M. J. & Mason, O. J. Models of Schizotypy: The Importance of Conceptual Clarity. Schizophr. Bull. 44, S556–S563 (2018).
Sabaroedin, K., Tiego, J. & Fornito, A. Circuit-Based Approaches to Understanding Corticostriatothalamic Dysfunction Across the Psychosis Continuum. Biol. Psychiatry 93, 113–124 (2023).
Millan, M. J. et al. Altering the course of schizophrenia: progress and perspectives. Nat. Rev. Drug Discov. 15, 485–515 (2016).
Lawrie, S. M., Hall, J., McIntosh, A. M., Owens, D. G. & Johnstone, E. C. The ‘continuum of psychosis’: scientifically unproven and clinically impractical. Br. J. Psychiatry 197, 423–425 (2010).
Voineskos, A. N., Jacobs, G. R. & Ameis, S. H. Neuroimaging Heterogeneity in Psychosis: Neurobiological Underpinnings and Opportunities for Prognostic and Therapeutic Innovation. Biol. Psychiatry 88, 95–102 (2020).
Theisen, C. et al. The heterogeneity of attenuated and brief limited psychotic symptoms: association of contents with age, sex, country, religion, comorbidities, and functioning. Front. Psychiatry 14, 1209485 (2023).
Griffiths, S. L., Lalousis, P. A., Wood, S. J. & Upthegrove, R. Heterogeneity in treatment outcomes and incomplete recovery in first episode psychosis: does one size fit all? Transl. Psychiatry 12, 485 (2022).
Zhang, Y. et al. Altered Resting-State Brain Activity in Schizophrenia and Obsessive-Compulsive Disorder Compared With Non-psychiatric Controls: Commonalities and Distinctions Across Disorders. Front. Psychiatry 12, 681701 (2021).
Spooner, R., Hartmann, J. A., McGorry, P. D., Nelson, B. New paradigms to study psychosis risk. Risk Factors Psychosis. 2020, 399–416 (2020).
Beresniewicz, J., et al. White Matter Microstructural Differences between Hallucinating and Non-Hallucinating Schizophrenia Spectrum Patients. Diagnostics. 11, https://doi.org/10.3390/diagnostics11010139 (2021).
Feczko, E. et al. The Heterogeneity Problem: Approaches to Identify Psychiatric Subtypes. Trends Cogn. Sci. 23, 584–601 (2019).
Wolfers, T. et al. Mapping the Heterogeneous Phenotype of Schizophrenia and Bipolar Disorder Using Normative Models. JAMA Psychiatry 75, 1146–1155 (2018).
Brugger, S. P. & Howes, O. D. Heterogeneity and Homogeneity of Regional Brain Structure in Schizophrenia: A Meta-analysis. JAMA Psychiatry 74, 1104–1111 (2017).
Alnaes, D. et al. Brain Heterogeneity in Schizophrenia and Its Association With Polygenic Risk. JAMA Psychiatry 76, 739–748 (2019).
Baldwin, H. et al. Neuroanatomical heterogeneity and homogeneity in individuals at clinical high risk for psychosis. Transl. Psychiatry 12, 297 (2022).
Doucet, G. E. et al. Person-Based Brain Morphometric Similarity is Heritable and Correlates With Biological Features. Cereb. Cortex 29, 852–862 (2019).
Antoniades, M. et al. Personalized Estimates of Brain Structural Variability in Individuals With Early Psychosis. Schizophr. Bull. 47, 1029–1038 (2021).
Kelly, S. et al. Widespread white matter microstructural differences in schizophrenia across 4322 individuals: results from the ENIGMA Schizophrenia DTI Working Group. Mol. Psychiatry 23, 1261–1269 (2018).
Stampfli, P. et al. Subtle white matter alterations in schizophrenia identified with a new measure of fiber density. Sci. Rep. 9, 4636 (2019).
Griffa, A. et al. Brain connectivity alterations in early psychosis: from clinical to neuroimaging staging. Transl. Psychiatry 9, 62 (2019).
Carletti, F. et al. Alterations in white matter evident before the onset of psychosis. Schizophr. Bull. 38, 1170–1179 (2012).
von Hohenberg, C. C. et al. White matter microstructure in individuals at clinical high risk of psychosis: a whole-brain diffusion tensor imaging study. Schizophr. Bull. 40, 895–903 (2014).
Schmidt, A. et al. Structural Network Disorganization in Subjects at Clinical High Risk for Psychosis. Schizophrenia Bull. 43, 583–591 (2016).
Surbeck, W. et al. Anatomical integrity within the inferior fronto-occipital fasciculus and semantic processing deficits in schizophrenia spectrum disorders. Schizophr. Res 218, 267–275 (2020).
Smigielski, L. et al. White matter microstructure and the clinical risk for psychosis: A diffusion tensor imaging study of individuals with basic symptoms and at ultra-high risk. Neuroimage Clin. 35, 103067 (2022).
Reis Marques, T. et al. White matter integrity as a predictor of response to treatment in first episode psychosis. Brain 137, 172–182 (2014).
Omlor, W., et al. Estimating multimodal brain variability in schizophrenia spectrum disorders: A worldwide ENIGMA study. bioRxiv, https://doi.org/10.1101/2023.09.22.559032 (2023).
DeRosse, P. & Karlsgodt, K. H. Examining the Psychosis Continuum. Curr. Behav. Neurosci. Rep. 2, 80–89 (2015). 2015/06/01.
Madigand, J., Tréhout, M., Delcroix, N., Dollfus, S. & Leroux, E. Corpus callosum microstructural and macrostructural abnormalities in schizophrenia according to the stage of disease. Psychiatry Res. Neuroimaging 291, 63–70 (2019).
Koshiyama, D. et al. White matter microstructural alterations across four major psychiatric disorders: mega-analysis study in 2937 individuals. Mol. Psychiatry 25, 883–895 (2019).
Sagarwala, R. & Nasrallah, H. A. White matter pathology is shared across multiple psychiatric brain disorders: Is abnormal diffusivity a transdiagnostic biomarker for psychopathology? Biomark. Neuropsychiatry. 2, https://doi.org/10.1016/j.bionps.2019.100010 (2020).
Wang, P. et al. Structural-functional connectivity deficits of callosal-white matter-cortical circuits in schizophrenia. Psychiatry Res. 330, 115559 (2023).
Acosta-Cabronero, J., Alley, S., Williams, G. B., Pengas, G., Nestor, P. J. Diffusion Tensor Metrics as Biomarkers in Alzheimer’s Disease. PLoS One 7, https://doi.org/10.1371/journal.pone.0049072 (2012).
Di Biase, M. A. et al. White matter changes in psychosis risk relate to development and are not impacted by the transition to psychosis. Mol. Psychiatry 26, 6833–6844 (2021).
Vitolo, E. et al. White matter and schizophrenia: A meta-analysis of voxel-based morphometry and diffusion tensor imaging studies. Psychiatry Res. Neuroimaging 270, 8–21 (2017).
Schmidt, A. et al. Brain Diffusion Changes in Emerging Psychosis and the Impact of State-Dependent Psychopathology. Neurosignals 23, 71–83 (2015).
Kirschner, M. et al. Ventral Striatal Dysfunction and Symptom Expression in Individuals With Schizotypal Personality Traits and Early Psychosis. Schizophr. Bull. 44, 147–157 (2018).
Cavelti, M. et al. Formal thought disorder is related to aberrations in language-related white matter tracts in patients with schizophrenia. Psychiatry Res. Neuroimaging 279, 40–50 (2018).
Riecher-Rossler, A. et al. The Basel early-detection-of-psychosis (FEPSY)-study–design and preliminary results. Acta Psychiatr. Scand. 115, 114–125 (2007).
Riecher-Rossler, A. et al. [The Basel Screening Instrument for Psychosis (BSIP): development, structure, reliability and validity]. Fortschr. Neurol. Psychiatr. 76, 207–216 (2008).
Yung, A. R. et al. Mapping the onset of psychosis: the Comprehensive Assessment of At-Risk Mental States. Aust. N. Z. J. Psychiatry 39, 964–971 (2005).
Breitborde, N. J., Srihari, V. H. & Woods, S. W. Review of the operational definition for first-episode psychosis. Early Inter. Psychiatry 3, 259–265 (2009).
Yung, A. R. et al. Prediction of psychosis. Br. J. Psychiatry 172, 14–20 (1998).
Lukoff, D. & Libermann, R. P. KH N. Symptom monitoring in the rehabilitation of schizophrenic patients. Schizophr. Bull. 12, 578–602 (1986).
American Psychiatric Association. Diagnostic and statistical manual of mental disorders (American Psychiatric Association, 2000).
Winkelbeiner, S. et al. Decreased blood flow in the right insula and middle temporal gyrus predicts negative formal thought disorder in schizophrenia. Schizophr. Res. 201, 432–434 (2018).
Sheehan, D. V. et al. The Mini-International Neuropsychiatric Interview (M.I.N.I.): the development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. J. Clin. Psychiatry 59, 22–33 (1998). quiz 34-57.
Kirschner, M. et al. Deficits in context-dependent adaptive coding in early psychosis and healthy individuals with schizotypal personality traits. Brain 141, 2806–2819 (2018).
Raine, A. The SPQ: a scale for the assessment of schizotypal personality based on DSM-III-R criteria. Schizophr. Bull. 17, 555–564 (1991).
Fortin, J. P. et al. Harmonization of multi-site diffusion tensor imaging data. Neuroimage 161, 149–170 (2017).
Johnson, W. E., Li, C. & Rabinovic, A. Adjusting batch effects in microarray expression data using empirical Bayes methods. Article. Biostatistics 8, 118–127 (2007).
Koutsouleris, N. et al. Disease prediction in the at-risk mental state for psychosis using neuroanatomical biomarkers: results from the FePsy study. Schizophr. Bull. 38, 1234–1246 (2012).
Bedford, P. et al. The effect of lysergic acid diethylamide (LSD) on whole-brain functional and effective connectivity. Neuropsychopharmacology 48, 1175–1183 (2023).
Doucet, G. E. et al. Personalized estimates of morphometric similarity in bipolar disorder and schizophrenia. NPJ Schizophr. 6, 39 (2020).
Doucet, G. E., Glahn, D. C. & Frangou, S. Person-based similarity in brain structure and functional connectivity in bipolar disorder. J. Affect Disord. 276, 38–44 (2020).
Doucet, G. similarityscore. Central File Exchange https://www.mathworks.com/matlabcentral/fileexchange/69158-similarityscore (2023).
Derrick B., White P. Why Welch’s test is Type I error robust. TQMP, https://doi.org/10.20982/tqmp.12.1.p030 (2016).
Ahad, N. A. & Yahaya, S. S. S. Sensitivity analysis of Welch’s t-test. AIP Conf. Proc. 1605, 888–893 (2014).
Viechtbauer, W. Conducting Meta-Analyses in R with the metafor Package. J. Stat. Softw. 36, 1–48 (2010).
Kristensen, T. D. et al. Global fractional anisotropy predicts transition to psychosis after 12 months in individuals at ultra-high risk for psychosis. Acta Psychiatr. Scand. 144, 448–463 (2021).
Melicher, T. et al. White matter changes in first episode psychosis and their relation to the size of sample studied: a DTI study. Schizophr. Res 162, 22–28 (2015).
Fang, K., Wen, B., Niu, L., Wan, B. & Zhang, W. Higher brain structural heterogeneity in schizophrenia. Front Psychiatry 13, 1017399 (2022).
Joo, S. W., et al. Structural variability of the cerebral cortex in schizophrenia and its association with clinical symptoms. Psychol Med. 54, 399–408 (2023).
Lee, S. H. et al. Extensive white matter abnormalities in patients with first-episode schizophrenia: a Diffusion Tensor Iimaging (DTI) study. Schizophr. Res 143, 231–238 (2013).
Kwapil, T. R., Barrantes-Vidal, N. & Silvia, P. J. The dimensional structure of the Wisconsin Schizotypy Scales: factor identification and construct validity. Schizophr. Bull. 34, 444–457 (2008).
Barrantes-Vidal, N., Grant, P. & Kwapil, T. R. The role of schizotypy in the study of the etiology of schizophrenia spectrum disorders. Schizophr. Bull. 41, S408–S416 (2015). Suppl 2(Suppl 2).
Palaniyappan, L. Clusters of psychosis: compensation as a contributor to the heterogeneity of schizophrenia. J. Psychiatry Neurosci. 48, E325–E329 (2023).
Haas, S. S., et al. Normative modeling of brain morphometry in Clinical High-Risk for Psychosis. bioRxiv, https://doi.org/10.1101/2023.01.17.523348 (2023).
Metzak, P. D., Devoe, D. J., Iwaschuk, A., Braun, A. & Addington, J. Brain changes associated with negative symptoms in clinical high risk for psychosis: A systematic review. Neurosci. Biobehav Rev. 118, 367–383 (2020).
Group ECHRfPW, Haas, S. S. et al. Normative Modeling of Brain Morphometry in Clinical High Risk for Psychosis. JAMA Psychiatry 81, 77–88 (2024).
Elad, D. et al. Improving the predictive potential of diffusion MRI in schizophrenia using normative models-Towards subject-level classification. Hum. Brain Mapp. 42, 4658–4670 (2021).
Penke, L. et al. Brain white matter tract integrity as a neural foundation for general intelligence. Mol. Psychiatry 17, 1026–1030 (2012).
Thalhammer, M., et al. Distinct Volume Alterations of Thalamic Nuclei Across the Schizophrenia Spectrum. Schizophr Bull. https://doi.org/10.1093/schbul/sbae037 (2024).
Lee, M., et al. Cognitive Function and Variability in Antipsychotic Drug-Naive Patients With First-Episode Psychosis: A Systematic Review and Meta-Analysis. JAMA Psychiatry. https://doi.org/10.1001/jamapsychiatry.2024.0016 (2024).
Acknowledgements
This work was supported by a grant from the Swiss National Science Foundation (AS, Nr: 320030_200801).
Author information
Authors and Affiliations
Contributions
G.C.I., S.U., and A.S. contributed to the conception and the design of the work, all authors contributed in the acquisition or in the interpretation of the data for the work; G.C.I. performed the literature research, data processing, statistical analysis and wrote the first draft of the manuscript; S.U. performed the statistical analyses and contributed to the manuscript; P.S. performed the preprocessing of the data; G.C.I. and A.S. finalised the draft; A.S. supervised the data processing and analysis; all authors revised it critically for important intellectual content; all authors gave their final approval of the version to be published.
Corresponding author
Ethics declarations
Competing interests
The authors declare that there are no competing financial or non-financial interests in relation to the subject of this study. P.H. has received grants and honoraria from Novartis, Lundbeck, Mepha, Janssen, Boehringer Ingelheim, and Neurolite outside of this work. No other disclosures were reported.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Iseli, G.C., Ulrich, S., Stämpfli, P. et al. Parsing heterogeneity in global and local white matter integrity at different stages across the psychosis continuum. Schizophr 10, 106 (2024). https://doi.org/10.1038/s41537-024-00516-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41537-024-00516-7
