
Abstract
Perinatal insults (e.g., obstetric complications, substance exposure) are increasing in prevalence and confer risk for psychotic-like experiences in offspring, contributing to a growing public health burden. Perinatal insults often co-occur, creating methodological challenges in understanding their impacts on psychosis-spectrum phenotypes. Data-driven approaches to organizing perinatal insults and testing their longitudinal effects on psychotic-like experiences in youth increases ecological validity and translational utility. Using data from 11,417 youth ages 9–14 across five years of the Adolescent Brain Cognitive Development (ABCD) Study, data-driven dimensions of perinatal insults were derived through exploratory factor analysis of thirty-one perinatal insults. Latent growth modeling tested the effect of perinatal insult dimensions on trajectories (baseline, rate-of-change, year-four severity) of distressing psychotic-like experiences. Six dimensions of perinatal insults were observed (substance exposure, obstetric complications, birth complications, postnatal challenges, parental age, medical needs). Substance exposure (β = 0.42, 95% CI [0.20, 0.63]), obstetric complications (β = 0.34, 95% CI [0.08, 0.61]), and parental age (β = 1.00, 95% CI [0.76, 1.22]) were associated with elevated baseline psychotic-like experiences. Perinatal insult dimensions were not associated with increasing rates-of-change in psychotic-like experiences. Medical needs (β = −0.12, 95% CI [−0.20, −0.05]) and parental age (β = −0.11, 95% CI [−0.18, −0.03]) were associated with steeper declines in psychotic-like experiences. Perinatal insult dimensions remained associated with elevated psychotic-like experiences at year-four. Data-driven dimensions of perinatal insults are associated with stably elevated psychotic-like experience trajectories across early adolescence. Given the role of psychotic-like experiences in later psychopathology and functioning, early identification of at-risk offspring is critical in reducing the public health burden of these exposures.
Similar content being viewed by others


Introduction
Perinatal insults like substance exposure, obstetric complications, and birth/delivery complications are increasing globally1,2,3,4 (~15% in the United States specifically in the last decade) further compounded by the COVID-19 pandemic5 and looming sociopolitical changes6. Exposure to perinatal insults is associated with psychopathology throughout development7,8, particularly psychosis-spectrum phenotypes9,10,11,12,13,14, imposing significant individual, familial, and economic burden15,16 and rendering this a major public health challenge. Difficulties modeling the heterogeneity of perinatal insults has limited their inclusion in early risk assessment, prevention, and intervention frameworks. This is likely because (1) there is currently no agreement on how to organize perinatal insults into a meaningful and useful framework and (2) it remains unclear how perinatal insult dimensions are associated with trajectories of psychotic-like experiences early in development.
Perinatal insults are typically modeled in two ways: specificity (i.e., testing one insult on an outcome10,17) and cumulative risk (i.e., testing the non-specific sum of insults on an outcome10,18). While numerous factors limit these approaches, a notable reality is that perinatal insults often co-occur within individuals19,20. For example, maternal hypertension is associated with prematurity21 and low birthweight22, whereas exposure to alcohol in utero is associated with concurrent cannabis and tobacco exposure23. This co-occurrence renders interpreting the effect of any one of these insults on psychopathology challenging. It can be difficult to parse whether an observed effect is a function of the measured insult or some other co-occurring but unmeasured exposure. Instead, perinatal insults likely aggregate into data-driven dimensions of conceptually and mechanistically similar environmental experiences with differential effects on psychopathology24. Data-driven dimensions of environmental risks are widely derived in studies of childhood insults, which demonstrate shared and unique effects of childhood insult dimensions on psychopathology25,26,27,28,29. Unfortunately, such an approach remains sparse in considerations of the perinatal period (though see ref. 30). These ecologically valid frameworks hold untapped value to perinatal insult conceptualization and interpretation.
Though specific and cumulative perinatal insults are associated with elevated psychosis phenotypes across development, the literature is overwhelmingly cross-sectional. For example, substance exposure and obstetric complications are risk factors for psychosis-spectrum phenomena independently in childhood10, adolescence13, and adulthood9. While informative, cross-sectional approaches neglect a fundamental principle: childhood through early adolescence represents a sensitive window of development wherein subclinical psychosis-spectrum phenotypes (e.g., psychotic-like experiences) often emerge31,32 and, in some, increase, conferring risk for transitioning to clinical high risk or frank psychosis33,34. Given the extant literature to date, it is unclear whether perinatal insults are associated with increasing psychosis symptoms across this period. Understanding how perinatal insult dimensions, which may serve as potentially modifiable etiological factors, influence trajectories of subclinical psychotic-like experiences throughout a window of development where such phenomena may first be assessed in clinical settings is critical to actionable translation.
Specificity and cumulative risk approaches in modeling perinatal insults have contributed to difficulty identifying mechanisms by which these insults confer risk for future elevations in psychotic-like experiences. While various mechanistic theories on how these risk factors influence psychopathology have gained support (e.g., that psychopathology develops from the cumulative impact of distinct “hits,” i.e., the two-hit hypothesis35; genetic mutation36), no one theory has dominated. Shared among extant theoretical frameworks is the potentially deleterious influence of perinatal insults on early neurodevelopment, which may in turn confer risk for maladaptive downstream outcomes. For example, some perinatal insults such as substance exposure and obstetric complications exert direct influences on neurodevelopment37,38,39,40. Others, like parental age and delivery type indirectly influence neurodevelopment41,42. As such, different dimensions of co-occurring perinatal insults may link to unique theoretical models and mechanisms, and ultimately distinct prevention and intervention efforts. To meaningfully test these models and mechanisms, it is necessary to first derive a framework through which modeling perinatal insults balances excessive splitting (i.e., specificity) and lumping (i.e., cumulative risk) of insults43.
The current longitudinal cohort study leveraged the Adolescent Brain Cognitive Development (ABCD) Study to address these limitations through two primary aims. First, perinatal insult dimensions were derived in a data-driven manner to generate a meaningful, ecologically valid framework by which to test longitudinal effects of perinatal insults. It was hypothesized that data-driven dimensions would largely reflect canonical categorizations of perinatal insults (e.g., obstetric complications, substance exposure) with certain insults being assimilated into dimensions into which they are not typically considered (e.g., unexpected pregnancy and substance exposure). Second, effects of perinatal insult dimensions on longitudinal trajectories of distressing psychotic-like experiences were estimated using annual data in youth from age 9 to 14. Dimensions were expected to have broad positive associations with baseline (age 9–10), rates-of-change, and year-four (age 13–14) severity across psychotic-like experiences.
Methods
Participants
All data are from the Adolescent Brain Cognitive Development (ABCD) study, an ongoing, longitudinal, population-based, cohort study of youth ages 9–10 at baseline (N = 11,868) and 13–14 (N = 4754, half of participants per ABCD data release schedule) at year-four. Data are collected from 21 research sites geographically distributed across the United States. Full recruitment details are documented elsewhere44; inclusion and exclusion criteria can be found in the supplementary material. Centralized institutional review board approval was obtained from the University of California, San Diego. Written consent/verbal assent was obtained from caregivers and youth. Analyses use data from all waves of the ABCD Study 5.1. Demographic characteristics can be found in Table 1.
Perinatal insult dimensions
Thirty-eight perinatal insults from the caregiver-reported Developmental History Questionnaire45,46,47 were originally identified for analyses. Insults spanned substance exposure, obstetric complications, birth and delivery complications, and various caregiver circumstances (e.g., nutrition, age at conception, unexpected pregnancy), with prevalence rates consistent with those observed in both cross-sectional and prospective studies (cf.18). Items endorsed by fewer than 1% of participants were removed prior to analyses to ameliorate potential model convergence, fit, and interpretation concerns [n = 4 items; proteinuria (0.47%), rubella (0.15%), convulsions (0.15%), blood transfusion (0.47%)]. Items correlated >0.90 were combined (n = 2 items) into one variable to attenuate multicollinearity. A final set of 31 perinatal insults were used for analyses. Full details on perinatal insults, including specific items, scoring, and endorsement/average are provided in Table S1.
Psychopathology outcomes
Psychotic-like experiences (PLEs) were assayed with the youth-reported Prodromal Questionnaire-Brief Child Version (PQ-BC48). The PQ-BC is a 21-item questionnaire that assesses positive PLEs (e.g., perceptual abnormalities, mild delusional thoughts) over the past month and has been validated in the ABCD sample48, providing more range and specificity than psychosis-related subscales from other measures. Analyses used distress scores [0 (not endorsed), 1 (endorsed with no distress) or 2–6 (1+distress score), range: 0–126]; supplemental analyses used sum scores (range: 0–21). Internalizing and externalizing symptoms were assayed with the parent-reported Child Behavior Checklist (CBCL)49. The CBCL is a widely used psychopathology rating scale comprised of 119 total items. Each item is rated on a three-point scale ("not true," "somewhat true," or "very true"). Analyses used raw scores (32 internalizing items, range: 0–96; 27 externalizing items, range: 0–81). The PQ-BC and CBCL are administered annually beginning at the ABCD study baseline visit. Descriptive statistics can be found in Table 1.
Statistical analyses
Overview
Analyses were conducted with R 4.2.0 and MPlus 8.11. To account for non-independence of observations, all models estimated cluster-robust standard errors with the sandwich estimator. Specifically, all models clustered data by family membership to account for siblings/multiple births and stratified data by research site. Additionally, analyses were weighted by poststratification weights provided by the ABCD Study to increase the representativeness of the sample. Together, this approach increases the validity of standard error estimates (thereby decreasing the potential for Type I error) and is consistent with previous work using the ABCD sample50,51.
Exploratory factor analysis & exploratory structural equation modelling
Thirty-one perinatal insults were included. Individuals missing >15% of perinatal insult data were removed from analyses (n = 446) (cf.30). For the remainder of youth, missing perinatal insults were imputed with an established imputation algorithm52. This non-parametric technique to estimating missing data utilizes a random forest imputation algorithm using the observed values to predict missing values, is uniquely suited to impute mixed categorical and continuous datasets, and outperforms other imputation models and case/variable deletion52,53.
Perinatal insult dimensions were derived using exploratory factor analysis (EFA) sensitive to variable type (e.g., continuous vs. dichotomous). Models with 1–10 factors were estimated using the weighted least squares mean and variance adjusted (WLSMV) estimator. The best-fitting model was selected based on a combination of (1) visual analysis of the Scree plot, (2) model fit statistics [Root Mean Squared Error of Approximation (RMSEA <0.05), Comparative Fit Index (CFI >0.95), Tucker-Lewis Index (TLI >0.95), Standardized Root Mean Squared Residual (SRMR <0.08)]54, and (3) conceptual interpretability. Item factor loadings above 0.30 were considered meaningful.
To obtain individual-level factor scores (i.e., scores on perinatal insult dimensions), exploratory structural equation modeling (ESEM)55 was conducted specifying the best-fitting number of factors from the EFA. Items that did not meaningfully load on to any factor (n = 5) were removed prior to ESEM. Factor scores were standardized prior to analyses. Full detail regarding the usefulness of an EFA plus ESEM approach for modeling early life risk factors are in supplemental materials.
Longitudinal modeling
Latent growth modeling (LGM)56 was used to test longitudinal associations between perinatal insult dimensions and trajectories of psychotic-like experiences. LGM is a structural equation modeling technique that estimates between-person differences in within-person change over time. First, unconditional LGMs established whole-sample trajectories for psychotic-like experiences. Second, perinatal insult dimension scores were entered as predictors of baseline (intercept) and rate-of-change (slope) for PLEs. Third, a model specifying the intercept at year four was estimated to evaluate perinatal insult dimension effects on PLEs at the final time-point. Specifying the intercept at the final timepoint, used to determine year-four symptom severity, does not alter model fit. Including both an intercept and slope factor simultaneously controls for baseline and rate-of-change in symptoms. LGMs used the robust maximum likelihood estimator. Model fit was evaluated via RMSEA (<0.05), CFI (>0.95), TLI (>0.95), and SRMR (<0.08)54. Missing psychopathology values were estimated with full information maximum likelihood (FIML) estimation under the robust maximum likelihood estimator. FIML outperforms other approaches to addressing missing data, including listwise and pairwise deletion, resulting in less biased parameter estimates57. All longitudinal models were adjusted for baseline age, race and ethnicity, biological sex, and family history of psychopathology. Results reported here reflect raw psychotic-like experience distress scores. To probe whether perinatal insult dimension conferred similar risk for other domains of psychopathology, we followed the same series of analytic steps with internalizing and externalizing psychopathology (Table S2 and Table S3). Including other demographic covariates (Area Deprivation Index, family income, parental self-reported psychopathology) and running models on standardized psychopathology scores did not substantively change the results (Table S4 and Table S5).
Results
Demographic details are provided in Table 1. Youth were 9.90 (SD = 0.62) at baseline and 14.08 (SD = 0.68) at year four. Forty-eight percent were female, 52% were male and majority (53%) were non-Hispanic White.
Perinatal insult dimensions
A 6-factor solution for perinatal insult dimensions best explained the co-occurrence of PIs (Fig. 1) (X2(294) = 158.87, p <0.001; RMSEA = 0.02, CFI = 0.96, TLI = 0.94, SRMR = 0.06). These dimensions reflected (1) substance exposure and unexpected pregnancy (“substance exposure”), (2) obstetric complications (“obstetric complications”), (3) birth complications (“birth complications”), where higher scores indicate more exposure within the dimension; (4) postnatal challenges (“postnatal challenges”), where higher scores reflect lower birthweight, earlier birth, and longer incubation time; (5) parental age and alcohol use (“parental age”), with higher scores representing younger parental age at conception; and (6) medical needs (“medical needs”), where higher scores indicate increasing number of medical visits and unspecified obstetric complications. Notably, alcohol exposure cross-loaded onto substance exposure and parental age dimensions. Requiring oxygen at birth cross-loaded onto birth complications and postnatal challenges dimensions. Item loadings (Table S6), model fit statistics for other EFA estimations (Table S7), relationships between perinatal insult dimensions (Table S8) and the EFA scree plot (Figure S1) can be found in the Supplemental Material.

Data-driven dimensions of perinatal insults obtained through exploratory factor analysis. The density of shading corresponds to the eigenvalue for the dimensions (darker=higher). Solid arrows indicate positive correlations between dimensions; dashed arrows indicate negative correlations between dimensions. Specific items, their loadings, eigenvalues for each dimension, and correlations between dimensions are presented in Table S1, Tables S6–S8, and Figure S1.
Psychotic-like experiences
On average, PLE distress decreased over time, with significant variability in intercept, slope, and year-four severity (Fig. 2, Table 2). Three perinatal insult dimensions were associated with greater distressing PLEs at baseline (age 9–10). Parental age had the largest effect (β = 1.00, 95% CI [0.76, 1.22]), followed by substance exposure (β = 0.42, 95% CI [0.20, 0.63]) and obstetric complications (β = 0.34, 95% CI [0.08, 0.61]). Medical needs and parental age dimensions were associated with distressing PLE slopes. Specifically, the medical needs dimension was associated with the steepest declines in PLE distress across time (β = −0.12, 95% CI [−0.20, −0.05]) and lower PLE distress at year-four (age 13–14) (β = −0.25, 95% CI [−0.42, −0.07]). That is, more frequent physician visits and unspecified obstetric complications were associated with faster declines in PLE distress across time that remained lower at the final timepoint. Similarly, the parental age dimension was negatively associated with the slope of PLE distress (β = −0.11, 95% CI [−0.18, −0.03]), such that younger age at conception was associated with faster declines in distressing PLEs across time. Of the dimensions associated with elevated baseline PLE severity, only the obstetric complications dimension was not associated with year-four PLE severity (age 13–14; Fig. 3A and B). Parental age had the largest effect at year-four (β = 0.58, 95% CI [0.39, 0.76]), followed by substance exposure (β = 0.28, 95% CI [0.10, 0.47]). Interestingly, the postnatal challenges dimension was only associated with year-four PLEs (β = 0.22, 95% CI [0.01–0.42]). Results were largely similar when evaluating trajectories of PLE sum scores (note, the parental age dimension association with slope became trend-level, p = 0.06) (Table S9).

Longitduinal trajectory of Psychotic-Like Experiences distress scores at the sample-level across ABCD Study waves. Mean age at Year 0 = 9.91-years-old; mean age at Year 4 = 14.08-years-old.

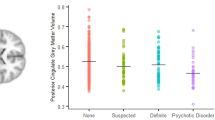
A Associations between perinatal insult dimensions and baseline, slope, and year-four severity of Psychotic-Like Experiences distress scores. B Linear trajectories of Psychotic-Like Experience distress scores by perinatal insult dimension. The sample was divided into tertiles (bottom, middle, and top thirds) for each dimension of perinatal insult for visualization purposes only. For reported analyses, perinatal insult dimension scores were treated as continuous variables. Point estimates and 95% confidence intervals (visualized here) for each group-by-dimension figure and corresponding line graphs in are presented in Supplemental Tables 11–16.
Internalizing and externalizing symptoms
On average, internalizing symptoms remained relatively stable across time (Figure S2a, see Table S2 for full model results). Obstetric complications (β = 0.54, 95% CI [0.35, 0.72]), parental age (β = 0.37, 95% CI [0.24, 0.50]), substance exposure (β = 0.35, 95% CI [0.23, 0.48]), and birth complications (β = 0.26, 95% CI [0.11, 0.42]) dimensions were associated with elevated internalizing symptoms at baseline (age 9–10). Similar to PLEs, parental age was negatively associated with the slope of internalizing symptoms (β = −0.10, 95% CI [−0.14, −0.06]). Substance exposure (β = 0.47, 95% CI [0.31, 0.64]) and obstetric complications (β = 0.45, 95% CI [0.25, 0.64]) dimensions remained associated with elevated symptoms at year-four (age 13-14); birth complications and parental age did not (Figure S3).
On average, externalizing symptoms modestly, but insignificantly, decreased across time (Figure S2b, see Table S2 for full model results). Parental age (β = 0.70, 95% CI [0.56, 0.83]), substance exposure (β = 0.64, 95% CI [0.50, 0.78]), obstetric complications (β = 0.43, 95% CI [0.24, 0.61]), and birth complications (β = 0.25, 95% CI [0.10, 0.40]) dimensions were associated with elevated externalizing symptoms at baseline (age 9-10). Parental age (β = −0.09, 95% CI [−0.12, −0.05]) and birth complications (β = −0.05, 95% CI [−0.09, −0.02]) dimensions were associated with faster declines in trajectories of externalizing symptoms. Except for birth complications, these dimensions continued to be associated with elevated year-four (age 13-14) symptom severity, with substance exposure demonstrating the largest effect (β = 0.60, 95% CI [0.44, 0.76]) (Figure S4).
Discussion
Perinatal insults are robust predictors of psychosis-spectrum phenotypes throughout development. However, existing approaches to modeling perinatal insults have been limited in their conceptual and translational utility as they do not account for the co-occurrence of insults within individuals and have been largely limited to cross-sectional outcomes. The current work leveraged a data-driven approach with a national sample to organize perinatal insults into a meaningful, ecologically valid framework. The present analyses converge on a key finding – starting at age nine, ecologically-valid dimensions of perinatal insults are associated with elevations in psychotic-like experiences that remain stable throughout late childhood into early adolescence.
A best-fitting six-dimension solution organized the co-occurrence of specific perinatal insults into a novel framework, distilling into (1) Substance Exposure, (2) Obstetric Complications, (3) Birth Complications, (4) Postnatal Challenges, (5) Parental Age, and (6) Medical Needs. While these dimensions largely reflect canonical categorizations of perinatal insults, several notable differences emerged. First, unexpected pregnancy loaded onto the substance exposure factor, consistent with results from a network approach to dimension-reduction of perinatal insults30. Indeed, this may reflect accidental substance use stemming from not expecting to become pregnant as opposed to clinically significant substance misuse throughout pregnancy. Second, alcohol exposure loaded on two factors – substance exposure and parental age. Given alcohol use loads substantially stronger onto the substance exposure factor, the smaller loading of alcohol exposure on parental age is potentially capturing normative age-related changes in alcohol use58. Finally, requiring oxygen at birth loaded onto both birth complications and postnatal challenges. Taken together, our analyses provide evidence that myriad perinatal insults can be organized into ecologically valid dimensions reflecting the co-occurrence of insults. These dimensions are more nuanced than, and extend beyond, general cumulative risk scores that have been overutilized in the extant literature. Utilizing this organizational framework for mechanistic and applied research could afford more robust and meaningful inferences regarding perinatal insult effects.
Perinatal insult dimensions exhibited broad associations with baseline psychotic-like experiences. Specifically, substance exposure, obstetric complications, and parental age were associated with elevated distressing psychotic-like experiences at baseline. No perinatal insult dimension was associated with fewer symptoms at baseline. Critically, these dimensions largely remained associated with elevated symptoms at the year-four follow-up. Multiple factors may contribute to the stability of elevated psychotic-like experience severity across time. First, healthcare systems may be doing a poor job at identifying offspring at greatest risk for future difficulties59. Understanding the developmental mechanisms through which perinatal insults confer risk for future psychopathology (e.g., alterations to fundamental developmental processes60,61) may mitigate this. Second, the persistence of perinatal insult impact may not be readily appreciated, such that current interventions are not tailored towards addressing underlying causes soon enough60.
However, compared to baseline, at year-four the obstetric complications dimension was no longer associated with PLEs distress. Notably, despite the medical needs dimension not being associated with baseline psychotic-like experiences, higher scores were associated with lower psychotic-like experience severity at year-four. It is interesting that the postnatal challenges dimension – comprised in part of birthweight and prematurity – was not associated with any outcome, contrary to existing research62,63. This may be a function of sampling, given that extremely low birthweight (<1200 grams) and extreme prematurity (<28 weeks gestational age) are ABCD exclusion criteria. Additionally, statistical limitations, including regression to the mean, measurement error in psychopathology rating scales, and reduction in rating scale “novelty” over time may underly these reductions.
Contrary to hypotheses, no perinatal insult dimension was associated with increasing psychotic-like experiences throughout adolescence. Perhaps counterintuitively, when relationships between PI dimensions and slopes were observed, they indicated faster decreases in symptoms across ages 9–14. Specifically, the medical needs factor was associated with greater rate of decline and lower year-four PLE severity. This dimension encapsulates two perinatal risk factors – number of physician visits and unspecified obstetric complications – that may index higher utilization of healthcare systems64,65. That is, youth higher on this dimension may have more access (i.e., well-resourced or due to need) to systems that are equipped to detect PLEs early and intervene accordingly. Future studies focused on healthcare utilization may better clarify the complex factors influencing access to care. Similar accelerated declines were seen between the parental age dimension psychotic-like experiences, where higher factor scores indicate younger ages at conception. Younger parents have more external support (e.g., familial involvement in child rearing, multiple streams of income66,67; or are in more frequent contact with support systems as a function of risks associated with earlier conception68, that may buffer against the impact of parental age on early psychotic-like experiences. Thus, access to care, healthcare contact and utilization, and familial support appear to be effective in attenuating risk for early PLE elevations above and beyond what may be a normative decrease in PLEs observed in the sample.
While perinatal insults have primarily been studied as a risk factor for psychosis-spectrum phenotypes9, the current findings add to the growing literature highlighting perinatal insults as a transdiagnostic psychopathology risk factor7,8. In the present work, perinatal insult dimension effects were not specific to elevated trajectories of psychotic-like experiences but demonstrated unique and shared associations with stably elevated trajectories of internalizing and externalizing symptoms (Table S10). This is unsurprising given the high comorbidity and phenomenological overlap of early psychotic-like experiences with other psychopathologies, especially in early development69,70. Similar patterns across psychopathologies may reflect similar etiopathological mechanisms of perinatal insults (e.g., disrupted neurodevelopment71, increased inflammation72) as clinical phenomenology emerges and differentiates (i.e., prodromal syndromes, frank psychosis). Conversely, it may be that perinatal insult dimensions exert effects on psychopathology at a broader level (e.g., the p-factor73) that is captured in analyses of specific domains of psychopathology. However, it should be considered that differences between perinatal insult dimensions and trajectories of different psychopathology domains may be, in part, a function of different reporters (youth-reported PLEs, caregiver-reported internalizing and externalizing symptoms).
The current results provide evidence that perinatal insult dimensions affect trajectories of psychotic-like experiences in varying ways, suggesting these insults may operate through unique paths or mechanisms. Moving these findings forward, accounting for the co-occurrence of perinatal insults may aid in supporting or clarifying theoretical models proposing how these potentially modifiable environmental factors uniquely confer risk for psychotic-like experiences. For example, one way in which the parental age dimension may influence offspring psychotic-like experiences is through de-novo mutations, which have been shown to be a risk factor for psychosis-spectrum phenotypes74,75. However, the parental age dimension may also confer risk through psychosocial mechanisms (e.g., financial stability, perinatal health literacy) discussed above. Accordingly, for individuals higher on this dimension, advancements in gene therapy or increasing home support may be beneficial in attenuating risk. The substance exposure and obstetric complications dimensions may be more strongly associated with oxidative stress mechanisms. Indeed, substance exposure and obstetric complications are associated with elevated oxidative stress markers and associated cellular damage76,77, which may increase risk for psychopathology in offspring78,79. Efforts to reduce maternal substance use and increase maternal physical health may support a decrease in offspring psychotic-like experiences. Alternatively, certain substances (e.g., alcohol, cannabis) have targeted effects on neurodevelopment, including brain regions implicated in psychosis risk, which may provide a more unifying hypothesis than studying these brain regions in isolation37,80. Finally, it is possible that perinatal insult dimensions in-and-of themselves confer a small degree of risk for later psychotic-like experiences and instead, in non-genetically predisposed youth, serve as a first “hit” that disrupts early development, with behavioral changes not observed until a second, later, “hit” (e.g., trauma, parental psychopathology, substance use) triggers the system35. Alternatively, perinatal insults may be the second “hit,” with genetic proneness (or a co-occurring dimension conferring genetic risk) being the first “hit.” Future studies testing the two-hit hypothesis with gene-by-environment interactions and/or dimensions of perinatal and childhood insults may be informative in allocating resources, prevention, and intervention efforts. Critically, perinatal insults disrupt global structural and functional neurodevelopment (e.g., see refs. 37,81,82), suggesting disrupted neurodevelopment as a shared mechanism. Future work is required to test how perinatal insult dimensions derived here may map onto such theoretical models, influence neurodevelopment and, ultimately, affect functional outcomes that confer risk for psychosis-spectrum phenotypes (e.g., motor, social, and cognitive development).
Considered holistically, in perinatal insult-exposed youth, early identification combined with structured support systems may be critical in offsetting future stable psychotic-like experience elevations a decade later. Though the mechanisms through which dimensions of perinatal insults are associated with these elevations in psychotic-like experiences prior to and throughout adolescence warrant future research, the perinatal period is a window of time where caregivers are in frequent contact with healthcare systems and may be ripe for identification efforts and implementation of perinatal stepped care models60.
Several limitations and future directions are worth addressing. First, all perinatal insult data was retrospectively reported 9–10 years after pregnancy. While this may have introduced a non-negligible degree of recall bias, previous longitudinal research has demonstrated that most perinatal risk factors (including binary metrics of substance use, obstetric, and birth complications) can be reliably recalled a decade post-partum compared to medical records at birth83,84,85, though some insults (e.g., continuous metrics of substance use, unexpected pregnancy) are more variable84,86. Second, the current approach to testing trajectories of psychopathology does not account for potential latent trajectory groups within the ABCD sample (i.e., subgroups of individuals characterized by different patterns of PLE trajectories)87,88. Future research testing whether perinatal insult dimensions are differentially associated with trajectory subgroups may be informative in further parsing psychopathology risk. Third, while the relative timing of some insults is known, specific information on the temporality of perinatal insults is not available. For example, for some insults (e.g., certain substances or obstetric complications), when and how long they occurred may shift their placement in or alter the structure of the dimensional model. Fourth, certain potent perinatal insults are not captured by the ABCD study that may give more depth to perinatal insult dimensions, such as caregiver stress89, inflammation during pregnancy90, and perinatal socioeconomic status91. Replicating and extending findings in other longitudinal datasets with perinatal data collection will be critical in refining this framework. Fifth, the removal of four perinatal insults with less than 1% endorsement may have excluded rare, but highly potent risk factors for psychopathology (e.g., rubella, convulsions)92,93. Longitudinal research with help-seeking birthing persons may increase the representation of these insults. Sixth, future work would benefit from systematically testing interactions among perinatal insult dimensions, as such interactions may suggest synergistic or buffering effects on trajectories of psychotic-like experiences. Finally, these results should be considered in the context of the United States. Future research will benefit from testing whether these perinatal dimensions and their effects on psychopathology are similar cross-culturally.
Increasing rates of perinatal insults as a function of global sociopolitical changes necessitates a refined understanding of how these exposures are organized and confer risk for psychopathology longitudinally. The current study demonstrates that perinatal insults can be meaningfully organized into a dimensional framework that accounts for their co-occurrence, extending beyond widely used but limited approaches. Dimensions of perinatal insults exhibited unique and shared associations with stable elevations across multiple domains of psychopathology during a highly developmentally sensitive window. Early and frequent healthcare contact and utilization, as well as familial support, may be efficacious in attenuating risk for early PLE elevations. Efforts to understand the mechanisms by which these insults result in psychopathology elevations by age 9–10 with the use of prospective birth cohorts (e.g., Healthy Brain and Child Development, Avon Longitudinal Study of Parents and Children) and increasing availability of early identification and support services to expectant and new caregivers holds untapped potential in reducing the public health burden of these exposures.
Data availability
Adolescent Brain Cognitive Development (ABCD) Study data are publicly-available through the National Data Archive.
Change history
20 November 2025
A Correction to this paper has been published: https://doi.org/10.1038/s41537-025-00691-1
References
Blue Cross Blue Shield Association. Trends in Pregnancy and Childbirth Complications in the U.S. (2020).
Jikamo, B., Adefris, M., Azale, T. & Alemu, K. Incidence, trends and risk factors of preeclampsia in sub-Saharan Africa: a systematic review and meta-analysis. PAMJ - One Health 11, 1–13 (2023).
Kumar, P., Srivastava, S., Maurya, C. & Dhillon, P. An assessment of the role of socio-economic, maternal and service utilization factors in increasing self-reported maternal complications in India. BMC Pregnancy Childbirth 21, 519 (2021).
Carvalho-Sauer, R. et al. Maternal and perinatal health indicators in Brazil over a decade: assessing the impact of the COVID-19 pandemic and SARS-CoV-2 vaccination through interrupted time series analysis. Lancet Reg. Health - Am 35, 100774 (2024).
Metz, T. D. et al. Association of SARS-CoV-2 Infection With Serious Maternal Morbidity and Mortality From Obstetric Complications. JAMA 327, 748 (2022).
Brubaker, L. & Bibbins-Domingo, K. Health Care Access and Reproductive Rights. JAMA 328, 1707 (2022).
Allen, N. B., Lewinsohn, P. M. & Seeley, J. R. Prenatal and perinatal influences on risk for psychopathology in childhood andadolescence. Dev. Psychopathol. 10, 513–529 (1998).
Tien, J., Lewis, G. D. & Liu, J. Prenatal risk factors for internalizing and externalizing problems in childhood. World J. Pediatr. WJP 16, 341–355 (2020).
Davies, C. et al. Prenatal and perinatal risk and protective factors for psychosis: a systematic review and meta-analysis. Lancet Psychiatry 7, 399–410 (2020).
Staines, L. et al. Examining the association between prenatal and perinatal adversity and the psychotic experiences in childhood. Psychol. Med. 1–12 https://doi.org/10.1017/S0033291724000187 (2024).
Zammit, S. et al. Investigating whether adverse prenatal and perinatal events are associated with non-clinical psychotic symptoms at age 12 years in the ALSPAC birth cohort. Psychol. Med. 39, 1457–1467 (2009).
Dorrington, S. et al. Perinatal maternal life events and psychotic experiences in children at twelve years in a birth cohort study. Schizophr. Res. 152, 158–163 (2014).
Kotlicka-Antczak, M., Pawełczyk, A., Rabe-Jabłońska, J., Śmigielski, J. & Pawełczyk, T. Obstetrical complications and Apgar score in subjects at risk of psychosis. J. Psychiatr. Res. 48, 79–85 (2014).
Bolhuis, K. et al. Maternal and paternal cannabis use during pregnancy and the risk of psychotic-like experiences in the offspring. Schizophr. Res. 202, 322–327 (2018).
O’Neil, S. et al. The High Costs of Maternal Morbidity Show Why We Need Greater Investment in Maternal Health. https://doi.org/10.26099/NZ8S-4708 (2021).
Lee, E. et al. Health Care Needs and Costs for Children Exposed to Prenatal Substance Use to Adulthood. JAMA Pediatr 178, 888 (2024).
Lees, B. et al. Association of Prenatal Alcohol Exposure With Psychological, Behavioral, and Neurodevelopmental Outcomes in Children From the Adolescent Brain Cognitive Development Study. Am. J. Psychiatry 177, 1060–1072 (2020).
Roffman, J. L. et al. Association of adverse prenatal exposure burden with child psychopathology in the Adolescent Brain Cognitive Development (ABCD) Study. PLOS ONE 16, e0250235 (2021).
Orri, M. et al. Perinatal adversity profiles and suicide attempt in adolescence and young adulthood: longitudinal analyses from two 20-year birth cohort studies. Psychol. Med. 52, 1255–1267 (2022).
Lebel, C. A. et al. Characterizing adverse prenatal and postnatal experiences in children. Birth Defects Res. 111, 848–858 (2019).
Stevens, W. et al. Short-term costs of preeclampsia to the United States health care system. Am. J. Obstet. Gynecol. 217, 237–248.e16 (2017).
Tsujimoto, Y. et al. Association of low birthweight and premature birth with hypertensive disorders in pregnancy: a systematic review and meta-analysis. J. Hypertens. 40, 205–212 (2022).
Tran, E. L., England, L. J., Park, Y., Denny, C. H. & Kim, S. Y. Systematic Review: Polysubstance Prevalence Estimates Reported during Pregnancy, US, 2009–2020. Matern. Child Health J. 27, 426–458 (2023).
McLaughlin, K. A., Sheridan, M. A., Humphreys, K. L., Belsky, J. & Ellis, B. J. The value of dimensional models of early experience: Thinking clearly about concepts and categories. Perspect. Psychology. Sci. 16, 1463–1472 (2021).
Brieant, A. et al. Characterizing the dimensional structure of early-life adversity in the Adolescent Brain Cognitive Development (ABCD) Study. Dev. Cogn. Neurosci. 61, 101256 (2023).
Nikolaidis, A. et al. Heterogeneity in caregiving-related early adversity: Creating stable dimensions and subtypes. Dev. Psychopathol. 34, 621–634 (2022).
Pollmann, A., Fritz, J., Barker, E. & Fuhrmann, D. Networks of Adversity in Childhood and Adolescence and Their Relationship to Adult Mental Health. Res. Child Adolesc. Psychopathol. https://doi.org/10.1007/s10802-022-00976-4 (2022).
Russell, J. D., Heyn, S. A., Peverill, M., DiMaio, S. & Herringa, R. J. Traumatic and Adverse Childhood Experiences and Developmental Differences in Psychiatric Risk. JAMA Psychiatry https://doi.org/10.1001/jamapsychiatry.2024.3231 (2024).
Sheridan, M. A., Shi, F., Miller, A. B., Salhi, C. & McLaughlin, K. A. Network structure reveals clusters of associations between childhood adversities and development outcomes. Dev. Sci. 23, 1–16 (2020).
Larson, E. R. & Moussa-Tooks, A. B. Dimensions of perinatal and childhood adversities both merge and remain distinct. Child Abuse Negl. 161, 1–12 (2025).
Lindgren, M. & Therman, S. Psychotic-like experiences in a nationally representative study of general population adolescents. Schizophr. Res. 270, 237–245 (2024).
Kelleher, I. et al. Prevalence of psychotic symptoms in childhood and adolescence: a systematic review and meta-analysis of population-based studies. Psychol. Med. 42, 1857–1863 (2012).
Burton, I. J., Tibbo, P. G., Ponto, N. & Crocker, C. E. Heterogeneity in assessing the risk of developing a psychotic disorder given a previous subclinical psychotic-like experience in children and adolescents: A systematic review and meta-analysis. Psychiatry Res. 342, 116207 (2024).
Healy, C. et al. Childhood and adolescent psychotic experiences and risk of mental disorder: a systematic review and meta-analysis. Psychol. Med. 49, 1589–1599 (2019).
Davis, J. et al. A review of vulnerability and risks for schizophrenia: Beyond the two hit hypothesis. Neurosci. Biobehav. Rev. 65, 185–194 (2016).
Gejman, P. V., Sanders, A. R. & Duan, J. The role of genetics in the etiology of schizophrenia. Psychiatr. Clin. North Am. 33, 35–66 (2010).
Ross, E. J., Graham, D. L., Money, K. M. & Stanwood, G. D. Developmental Consequences of Fetal Exposure to Drugs: What We Know and What We Still Must Learn. Neuropsychopharmacology 40, 61–87 (2015).
Kovács, M. V., Charchat-Fichman, H., Landeira-Fernandez, J., Medina, A. E. & Krahe, T. E. Combined exposure to alcohol and cannabis during development: Mechanisms and outcomes. Alcohol 110, 1–13 (2023).
Wang, B., Zeng, H., Liu, J. & Sun, M. Effects of Prenatal Hypoxia on Nervous System Development and Related Diseases. Front. Neurosci. 15, 755554 (2021).
Gumusoglu, S. B., Chilukuri, A. S. S., Santillan, D. A., Santillan, M. K. & Stevens, H. E. Neurodevelopmental Outcomes of Prenatal Preeclampsia Exposure. Trends Neurosci 43, 253–268 (2020).
Janecka, M. et al. Advanced paternal age effects in neurodevelopmental disorders—review of potential underlying mechanisms. Transl. Psychiatry 7, e1019–e1019 (2017).
Kenkel, W. Birth signalling hormones and the developmental consequences of caesarean delivery. J. Neuroendocrinol. 33, e12912 (2021).
Smith, K. E. & Pollak, S. D. Rethinking Concepts and Categories for Understanding the Neurodevelopmental Effects of Childhood Adversity. Perspect. Psychol. Sci. 16, 67–93 (2021).
Garavan, H. et al. Recruiting the ABCD sample: Design considerations and procedures. Dev. Cogn. Neurosci. 32, 16–22 (2018).
Merikangas, K. R., Avenevoli, S., Costello, E. J., Koretz, D. & Kessler, R. C. National Comorbidity Survey Replication Adolescent Supplement (NCS-A): I. Background and Measures. J. Am. Acad. Child Adolesc. Psychiatry 48, 367–379 (2009).
Kessler, R. C. et al. Design and field procedures in the US National Comorbidity Survey Replication Adolescent Supplement (NCS-A). Int. J. Methods Psychiatr. Res. 18, 69–83 (2009).
Kessler, R. C. et al. National Comorbidity Survey Replication Adolescent Supplement (NCS-A): III. Concordance of DSM-IV/CIDI Diagnoses With Clinical Reassessments. J. Am. Acad. Child Adolesc. Psychiatry 48, 386–399 (2009).
Karcher, N. R. et al. Assessment of the Prodromal Questionnaire–Brief Child Version for Measurement of Self-reported Psychoticlike Experiences in Childhood. JAMA Psychiatry 75, 853 (2018).
Achenbach, T. M. Manual for the Child Behavior Checklist/4-18 and 1991 Profile. (Dept. of Psychiatry, University of Vermont, Burlington, VT, 1991).
Jeong, H. J. et al. General and Specific Factors of Environmental Stress and Their Associations With Brain Structure and Dimensions of Psychopathology. Biol. Psychiatry Glob. Open Sci. S2667174322000593. https://doi.org/10.1016/j.bpsgos.2022.04.004 (2022).
Reimann, G. E. et al. Atypical Functional Network Properties and Associated Dimensions of Child Psychopathology During Rest and Task Performance. Biol. Psychiatry Glob. Open Sci. S266717432200091X. https://doi.org/10.1016/j.bpsgos.2022.07.007 (2022).
Stekhoven, D. J. & Bühlmann, P. MissForest—non-parametric missing value imputation for mixed-type data. Bioinformatics 28, 112–118 (2012).
Waljee, A. K. et al. Comparison of imputation methods for missing laboratory data in medicine. BMJ Open 3, e002847 (2013).
Hu, L. & Bentler, P. M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Model. Multidiscip. J. 6, 1–55 (1999).
Marsh, H. W., Morin, A. J. S., Parker, P. D. & Kaur, G. Exploratory Structural Equation Modeling: An Integration of the Best Features of Exploratory and Confirmatory Factor Analysis. Annu. Rev. Clin. Psychol. 10, 85–110 (2014).
Bollen, K. A. & Curran, P. J. Latent Curve Models: A Structural Equation Perspective. (Wiley-Interscience, Hoboken, N.J, 2006).
Enders, C. & Bandalos, D. The Relative Performance of Full Information Maximum Likelihood Estimation for Missing Data in Structural Equation Models. Struct. Equ. Model. Multidiscip. J. 8, 430–457 (2001).
Britton, A., Ben-Shlomo, Y., Benzeval, M., Kuh, D. & Bell, S. Life course trajectories of alcohol consumption in the United Kingdom using longitudinal data from nine cohort studies. BMC Med. 13, 47 (2015).
Karcher, N. R. et al. Youth Mental Health Screening and Linkage to Care. Psychiatr. Serv. Wash. DC 74, 727–736 (2023).
Liu, C. H., Keshavan, M. S., Tronick, E. & Seidman, L. J. Perinatal Risks and Childhood Premorbid Indicators of Later Psychosis: Next Steps for Early Psychosocial Interventions. Schizophr. Bull. 41, 801–816 (2015).
Mwaniki, M. K., Atieno, M., Lawn, J. E. & Newton, C. R. Long-term neurodevelopmental outcomes after intrauterine and neonatal insults: a systematic review. The Lancet 379, 445–452 (2012).
Mathewson, K. J. et al. Mental health of extremely low birth weight survivors: A systematic review and meta-analysis. Psychol. Bull. 143, 347–383 (2017).
Johnson, S. & Marlow, N. Preterm Birth and Childhood Psychiatric Disorders. Pediatr. Res. 69, 11R–18R (2011).
Harris, A. et al. Emergency Room Utilization After Medically Complicated Pregnancies: A Medicaid Claims Analysis. J. Womens Health 2002 24, 745–754 (2015).
Bennett, W. L. et al. Utilization of Primary and Obstetric Care After Medically Complicated Pregnancies: An Analysis of Medical Claims Data. J. Gen. Intern. Med. 29, 636–645 (2014).
Goisis, A. Maternal Age at First Birth and Parental Support: Evidence From the UK Millennium Cohort Study. Popul. Res. Policy Rev. 42, 75 (2023).
Al-Mutawtah, M., Campbell, E., Kubis, H.-P. & Erjavec, M. Women’s experiences of social support during pregnancy: a qualitative systematic review. BMC Pregnancy Childbirth 23, 782 (2023).
Fraser, A. M., Brockert, J. E. & Ward, R. H. Association of Young Maternal Age with Adverse Reproductive Outcomes. N. Engl. J. Med. 332, 1113–1118 (1995).
Fusar-Poli, P., Nelson, B., Valmaggia, L., Yung, A. R. & McGuire, P. K. Comorbid Depressive and Anxiety Disorders in 509 Individuals With an At-Risk Mental State: Impact on Psychopathology and Transition to Psychosis. Schizophr. Bull. 40, 120–131 (2014).
Giocondo, J. G. et al. Psychotic-like Experiences and Common Mental Disorders in Childhood and Adolescence: Bidirectional and Transdiagnostic Associations in a Longitudinal Community-based Study. Schizophr. Bull. Open 2, sgab028 (2021).
Van Den Bergh, B. R. H., Dahnke, R. & Mennes, M. Prenatal stress and the developing brain: Risks for neurodevelopmental disorders. Dev. Psychopathol. 30, 743–762 (2018).
Frazier, J. A. et al. Perinatal Factors and Emotional, Cognitive, and Behavioral Dysregulation in Childhood and Adolescence. J. Am. Acad. Child Adolesc. Psychiatry 62, 1351–1362 (2023).
Leusin, F. et al. Perinatal and neonatal factors and mental disorders in children and adolescents: looking for the contributions of the early environment to common and dissociable aspects of psychopathology. Eur. Child Adolesc. Psychiatry 33, 3571–3581 (2024).
Feng, Y.-C. A. et al. Paternal age, de novo mutation, and age at onset among co-affected schizophrenia sib-pairs: whole-genome sequencing in multiplex families. Mol. Psychiatry 30, 3560–3567 (2025).
Taylor, J. L. et al. Paternal-age-related de novo mutations and risk for five disorders. Nat. Commun. 10, 1–9 (2019).
Duhig, K., Chappell, L. C. & Shennan, A. H. Oxidative stress in pregnancy and reproduction. Obstet. Med. 9, 113–116 (2016).
Viola, T. W. et al. Effects of substance use disorder on oxidative and antioxidative stress markers: A systematic review and meta-analysis. Addict. Biol. 28, 1–14 (2023).
Rommel, A.-S. et al. Associations between urinary biomarkers of oxidative stress in the third trimester of pregnancy and behavioral outcomes in the child at 4 years of age. Brain. Behav. Immun. 90, 272–278 (2020).
Pham, C. et al. Maternal oxidative stress during pregnancy associated with emotional and behavioural problems in early childhood: implications for foetal programming. Mol. Psychiatry 28, 3760–3768 (2023).
Peterson, B. S. et al. Associations of Maternal Prenatal Drug Abuse With Measures of Newborn Brain Structure, Tissue Organization, and Metabolite Concentrations. JAMA Pediatr 174, 831 (2020).
Costas-Carrera, A., Garcia-Rizo, C., Bitanihirwe, B. & Penadés, R. Obstetric Complications and Brain Imaging in Schizophrenia: A Systematic Review. Biol. Psychiatry Cogn. Neurosci. Neuroimaging 5, 1077–1084 (2020).
Du, J. et al. Association between parental age, brain structure, and behavioral and cognitive problems in children. Mol. Psychiatry 27, 967–975 (2022).
Ramos, A. M. et al. Maternal Consistency in Recalling Prenatal Experiences at 6 Months and 8 Years Postnatal. J. Dev. Behav. Pediatr. 41, 698–705 (2020).
Liu, J., Tuvblad, C., Li, L., Raine, A. & Baker, L. A. Medical Record Validation of Maternal Recall of Pregnancy and Birth Events From a Twin Cohort. Twin Res. Hum. Genet. 16, 845–860 (2013).
Keenan, K. et al. Concordance between maternal recall of birth complications and data from obstetrical records. Early Hum. Dev. 105, 11–15 (2017).
Guzzo, K. B. & Hayford, S. R. Revisiting Retrospective Reporting of First-Birth Intendedness. Matern. Child Health J. 18, 2141–2147 (2014).
Jia, L. et al. The developmental and dynamic relationship between psychopathology and psychotic-like experiences trajectories in children and adolescents. J. Affect. Disord. S0165032724015878. https://doi.org/10.1016/j.jad.2024.09.100 (2024).
Musci, R. J. et al. Psychosis Symptom Trajectories Across Childhood and Adolescence in Three Longitudinal Studies: An Integrative Data Analysis with Mixture Modeling. Prev. Sci. 24, 1636–1647 (2023).
Glover, V. Annual Research Review: Prenatal stress and the origins of psychopathology: an evolutionary perspective. J. Child Psychol. Psychiatry 52, 356–367 (2011).
Mac Giollabhui, N. et al. Maternal inflammation during pregnancy and offspring psychiatric symptoms in childhood: Timing and sex matter. J. Psychiatr. Res. 111, 96–103 (2019).
Badini, I. et al. Socioeconomic status and risk for child psychopathology: exploring gene–environment interaction in the presence of gene–environment correlation using extended families in the Norwegian Mother, Father and Child Birth Cohort Study. J. Child Psychol. Psychiatry 65, 176–187 (2024).
Brown, A. S., Cohen, P., Greenwald, S. & Susser, E. Nonaffective Psychosis After Prenatal Exposure to Rubella. Am. J. Psychiatry 157, 438–443 (2000).
Kariuki, S. M., Newton, C. R. J. C., Prince, M. J. & Das-Munshi, J. The Association Between Childhood Seizures and Later Childhood Emotional and Behavioral Problems: Findings From a Nationally Representative Birth Cohort. Psychosom. Med. 78, 620–628 (2016).
Acknowledgements
This work was supported by the National Institute of Mental Health (T32 MH103213 to ERL and K23 MH135215 to ABM). The ABCD Study® is supported by the National Institutes of Health and additional federal partners under award numbers U01DA041048, U01DA050989, U01DA051016, U01DA041022, U01DA051018, U01DA051037, U01DA050987, U01DA041174, U01DA041106, U01DA041117, U01DA041028, U01DA041134, U01DA050988, U01DA051039, U01DA041156, U01DA041025, U01DA041120, U01DA051038, U01DA041148, U01DA041093, U01DA041089, U24DA041123, U24DA041147. A full list of supporters is available at https://abcdstudy.org/federal-partners.html. A listing of participating sites and a complete listing of the study investigators can be found at https://abcdstudy.org/consortium_members/. The funding organization had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication. ABCD consortium investigators designed and implemented the study and/or provided data but did not necessarily participate in the analysis or writing of this report. This manuscript reflects the views of the authors and may not reflect the opinions or views of the NIH or ABCD consortium investigators. We thank the youth and their families who contributed their time and data to the Adolescent Brain Cognitive Development Study. Data used in the preparation of this article were obtained from the Adolescent Brain Cognitive Development (ABCD) Study (https://abcdstudy.org), held in the NIMH Data Archive (NDA). This is a multisite, longitudinal study designed to recruit more than 10,000 children age 9–10 and follow them over 10 years into early adulthood. Accordingly, the ABCD data repository grows and changes over time. The ABCD data used in this report came from https://doi.org/10.15154/z563-zd24 and can be accessed and used by other researchers through NDA.
Author information
Authors and Affiliations
Contributions
E.R.L., N.R.K., and A.B.M. conceptualized and designed the study. E.R.L. and A.B.M. conducted formal data analyses. E.R.L., N.R.K., and A.B.M. interpreted the results. A.B.M. and N.R.K. provided supervision throughout the project. E.R.L. and A.B.M. drafted the manuscript. E.R.L., N.R.K., and A.B.M. critically revised the manuscript. All authors agree to the final version. Each author is accountable for all aspects of the work.
Corresponding author
Ethics declarations
Ethical approval
Centralized institutional review board approval for the Adolescent Brain Cognitive Development (ABCD) study was obtained from the University of California, San Diego. Written consent/verbal assent was obtained from caregivers and youth. The current project obtained local Indiana University IRB approval (IRB #19488) to conduct secondary data analysis with the ABCD study.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Larson, E.R., Karcher, N.R. & Moussa-Tooks, A.B. Perinatal insult dimensions and developmental trajectories of psychotic-like experiences. Schizophr 11, 115 (2025). https://doi.org/10.1038/s41537-025-00662-6
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41537-025-00662-6
