
Abstract
Climate change has markedly increased adverse effects on human health and economic growth1,2,3. However, few studies have differentiated the impacts of extreme temperatures at the city level and analysed the future implications for human health under various climate change scenarios4,5,6. Here we leverage data on historical relationships among six kinds of climate-sensitive diseases (CSDs) and associated hospitalizations and temperatures across 301 cities (more than 90% of all cities) and more than 7,000 hospitals in China, and use a nonlinear distributed lag model. This study projects hospitalization risks associated with extreme temperatures through to the year 2100 and develops the hospitalization burden economic index to assess the burden under three carbon emission scenarios across cities. Five dimensions, including spatial distribution, disease categories, population age groups, future time horizons and carbon emission development pathways, have been evaluated. Historical data indicate a higher incidence of temperature-related risks among the CSDs in northwestern and southwestern China. Notably, gestation-related disease risks are associated with increased vulnerability to extreme heat in specific regions. The projections show that under current thermal conditions without adaptations, the excess hospitalizations from extreme heat will reach 0.6, 3.8 and 5.1 million by 2100 under the low-, middle- and high-emission scenarios, respectively. These findings highlight the need for targeted mitigation strategies to reduce uneven climate-related hospitalization risks and economic burdens while accounting for differences in city geography, extreme temperatures, population groups and carbon emission development pathways.
Similar content being viewed by others

Main
Climate change increasingly endangers human health across generations, both through direct health impacts and through widespread disruptions to environmental and social systems1,2,3,4. As climate change continues, extreme temperatures constitute the most widespread and global challenge to public health and health care systems5,6. The increasing frequency of extreme temperatures poses increased health risks, characterized by thermoregulatory failure leading to organ-specific pathologies through mechanisms such as acute heat-related illnesses, electrolyte imbalances and the exacerbation of pre-existing conditions (for example, cardiovascular, respiratory and renal disorders), along with adverse maternal and neonatal health outcomes, as well as climate-sensitive diseases (CSDs)7,8,9. Moreover, emerging evidence identifies pregnancy as an important vulnerability window, in which inflammatory and metabolic stressors increase the risk of preterm birth, gestational diabetes and related obstetric complications10. Concurrently, heat exposure increases the incidence of nephrolithiasis through dehydration, disrupts electrolyte homeostasis and accelerates both acute kidney injury progression and chronic decline in renal function7,11,12. Temperature-related admissions, therefore, continue to be the primary indicator of clinical decompensation13.
The health impacts of extreme temperatures vary across populations and regions because of complex physiological, behavioural, environmental and socioeconomic interactions. Numerous studies have highlighted greater risks among the elderly14, newborns15 and rural populations16. Physiological vulnerabilities across age groups differentially exacerbate climate-sensitive health threats. Moreover, inequalities in medical burdens from temperature extremes have been observed across hemispheres14,17 and ethnic groups18. Given the complexity of the issue and the limitations of existing studies, the climate sensitivity of health outcomes to temperature warrants further investigation in broader geographical and demographic contexts.
Cities, as fundamental units of socioeconomic activity and health resource distribution, provide an ideal setting for studying temperature–health dynamics19. Urban populations experience relatively uniform climate conditions, lifestyles and health systems, enabling more precise risk characterization and policy interventions20. Furthermore, cities with lower economic development levels may struggle with inadequate medical resources, whereas developed cities face challenges related to chronic disease burdens and mental health issues. Thus, targeted and localized adaptation strategies are necessary to increase resilience to future climate-driven health threats.
Although global attention to the health impacts of extreme temperatures has increased5,7,21, systematic city-level analyses remain rare. The vast population of China is distributed across diverse environments, geographical conditions and demographic backgrounds, leading to heterogeneity in extreme temperature events and associated health risks. This heterogeneity not only poses widespread challenges but also holds great research importance. The cumulative evidence points to systemic vulnerabilities spanning thermoregulatory stress pathways—from cardiovascular decompensation to metabolic dysregulation—with particular severity observed in respiratory, genitourinary and mental health disorders, whereas more findings highlight pregnancy as an important window of climate-sensitive morbidity, as exemplified by heat-related health risks for stroke, stillbirth9, specific injuries and cardiovascular diseases22. Typically, regional or monitoring sites often lack comprehensive analysis at the city level because of data constraints. Moreover, China faces considerable disparities in regional adaptability, medical infrastructure and socioeconomic conditions. It is necessary to study the impact and preparedness of the health care system in the context of climate change23,24. More importantly, previous studies typically emphasize either heat-related or cold-related health impacts independently, often neglecting the differing medical burdens that extreme heat and cold impose on various disease categories. This gap becomes particularly evident under future climate change and socioeconomic uncertainties. Furthermore, studies that consider both temperature extremes simultaneously at the city level remain scarce, especially those that integrate prospective climate warming scenarios.
This study first uses a distributed lag nonlinear model (DLNM) and fixed-effects methods, and uses daily hospitalization data from more than 7,000 hospitals in 301 cities (accounting for more than 90% of all cities) across China between 2021 and 2023 to systematically investigate the historical relationship between temperature fluctuations and hospital admissions (reported as relative risk (RR)), differentiating the health impacts of extreme heat and extreme cold across geographical locations and age groups. Specifically, the analysis included five CSD categories (circulatory, respiratory, endocrine/metabolic, psychiatric and genitourinary) and one gestation-related category (pregnancy, childbirth and puerperium-related conditions). This ‘5 + 1’ classification includes five for the general population and one specific to pregnant women, capturing both general and gestation-related climate-related health risks. Then, future excess hospitalization risks associated with extreme heat and cold temperatures under climate uncertainties through 2100 are projected by coupling climate change scenarios with shared socioeconomic pathways (SSPs): SSP1-2.6 (low-emission scenario), SSP2-4.5 (medium-emission scenario) and SSP5-8.5 (high-emission scenario). Finally, this study proposes the hospitalization burden economic index (HBEI) of excess temperature-related hospitalizations while considering future urban economic development trends. These analyses enhance the understanding of temperature-sensitive health outcomes, provide evidence to optimize the allocation of healthcare resources across climates, populations and disease, and further extend these insights into future time frames and alternative carbon emission scenarios.
Impact of temperature on hospitalization
The historical analysis of temperature-related hospitalization patterns across 295 Chinese cities shows distinct geographical and demographic variations in health risks, examining spatial distribution, CSDs and age-specific vulnerability patterns.
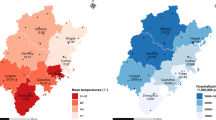
Hospitalization patterns demonstrate regional variations in response to extreme heat (Fig. 1a, Extended Data Fig. 4 and Supplementary Tables 1–4). Northwest and Southwest China, particularly Gansu (about 32°–42° N, 92°–108° E) and Sichuan Provinces (about 26°–34° N, 97°–108° E), show higher RR values for heat-related admissions. A 2-fold difference in heat effects and 1.5-fold difference in cold effects exists between the highest-risk and lowest-risk regions, with southern and eastern cities showing enhanced adaptation or reduced inherent risk25. Cold exposure analysis (Fig. 1b) showed elevated RR (>1.300) in northwestern and southwestern regions, particularly southwestern China—areas with complex terrain dominated by basins and mountains and small temperature variability—and in Gansu and Xinjiang (around 35°–49° N, 73°–96° E) with low temperatures but greater variability. An interesting paradox emerges: regions with the highest cold sensitivity often coincide with heat risk areas, particularly northwest and southwest regions, suggesting compound climate-related health challenges.

a,b, RR of extreme heat (a) and cold (b) for hospital admissions at the 95th and 5th percentile temperatures across 295 cities in China over 2021–2023. The RR of hospitalization associated with extreme heat and cold across Chinese cities is shown, stratified by six kinds of CSD categories: circulatory diseases; respiratory diseases; genitourinary diseases; endocrine, nutritional and metabolic diseases; psychiatric diseases; and GRDs (including pregnancy, childbirth and puerperium-related conditions). The cut-out of islands is the South China Sea Islands. The data for the basis map were sourced from the Standard Map Service Platform (http://bzdt.ch.mnr.gov.cn) supervised by the Ministry of Natural Resources of China. The approval number of the basemap is 2023 (2767). The grey areas on the map indicate regions with no data. c, Age differences in the RR of extreme heat compared with extreme cold across 21 provincial capital cities in different regions. The risk associated with extreme heat (95th percentile) and extreme cold (5th percentile) is shown. d, Estimated results of the associations between different temperature effects (with 95% confidence interval) and hospitalization. Data are presented as regression coefficients with 95% confidence intervals based on regression analyses with varying sample sizes: north (n = 27,894), northeast (n = 36,961), east (n = 81,475), south (n = 37,552), central (n = 44,943), southwest (n = 40,748), northwest (n = 47,750), and national (n = 319,469) observations. *P < 0.1, **P < 0.05, ***P < 0.01.
Extreme temperature exposure had differential hospitalization impacts across disease categories, with respiratory diseases demonstrating pronounced heat-associated RR values (1.056–3.772) (Fig. 1a, Extended Data Fig. 1 and Supplementary Information section 6). Notably, northern China emerged as the epicentre for heat-related circulatory and respiratory hospitalizations, whereas cold extremes disproportionately affected respiratory health in the northwest. Geospatial analysis showed that western China is a multirisk hotspot, exhibiting vulnerability to both heat and cold extremes across endocrine, nutritional and metabolic diseases and genitourinary diseases. Geospatial analysis also showed substantial disparities in gestation-related disease (GRD) hospitalization risks across China. As shown in Fig. 1, extreme heat imposed notably greater RR (1.011–1.274) than cold extremes did (1.002–1.217; RR > 1.1 in only 6 cities), with 151 cities exhibiting heat-related RR values exceeding 1.1. The analysis showed a new geographical lens, revealing ‘GRDs Thermal Risk Demarcation Line’ of China (Extended Data Fig. 6 and Supplementary Information section 7), which separates northern heat-vulnerable clusters from southern cold-sensitive zones. This demarcation framework explains the observed disparities in hospitalization: northern China presented elevated heat-related risks, and southern China presented cold-related risks.
Children and adolescents (0–18 years of age) and elderly populations (65 years of age and older) showed fluctuating hospital admissions under heat exposure. Surprisingly, children and adolescents demonstrated high heat sensitivity across multiple urban centres, such as Beijing, Wuhan (about 29°–31° N, 113°–115° E) and Lanzhou (about 35°–37° N, 102°–104° E) (Fig. 1c). Whereas elderly populations experience greater absolute hospitalizations, children and adolescents exhibit substantial rate changes in risk per unit temperature increase (Extended Data Fig. 5). This heightened sensitivity of children and adolescent may stem from fragile bodies and immature regulatory mechanisms26. Analysis of hospital admissions across 21 Chinese provincial capitals showed minimal sex differences in RR for both extreme heat (95th percentile) and extreme cold (5th percentile), with largely consistent RR values between sexes in cities and higher heat vulnerability in northern cities (Extended Data Figs. 2 and 3).
The temperature–hospitalization relationship exhibited complex patterns (Fig. 1d, Supplementary Information sections 1–5 and 8 and Supplementary Tables 1–6), with negative effects at low temperatures and progressively increasing positive coefficients as temperatures rise. Temperature variability showed no significant impact (P = 0.267), indicating absolute temperature levels drive admissions. Regional analysis demonstrated substantial heterogeneity. The eastern (P < 0.001), central (P = 0.001) and northwestern (P < 0.001) regions show significant increases in hospital admissions during extreme cold events, with the eastern (P < 0.001) and central (P < 0.001) regions exhibiting nonlinear relationships. High-temperature impacts are most pronounced in northern (P = 0.007) and northeastern (P = 0.029) China, with the northern (P = 0.039) region showing positive linear effects. Temperature deviation effects are particularly significant in northern (P < 0.001), northeastern (P = 0.018) and eastern China (P = 0.011). The northern region has strong responses to both the temperature range (P = 0.001) and standard deviation (P < 0.001). Similar patterns appear in the northeastern and eastern regions with varying magnitudes and directions. These findings show complex interactions between regional, demographic and climatic factors, requiring targeted monitoring strategies: northwestern and southwestern regions need attention for both temperature extremes, whereas central and northeast regions require extreme heat monitoring, and northern regions should prioritize temperature variability assessments.
Future frequency of extreme temperatures
Global warming has led to an increase in baseline temperatures, and irreversible temperature changes are occurring across regions under three carbon emission scenarios (Extended Data Fig. 7). This study projects the future frequency of temperature extremes, as both extremes could be altered under future climate uncertainties.
Extreme temperature thresholds evolve by scenarios and region across methods (Extended Data Fig. 8). Extreme temperature events are becoming increasingly frequent because of future climate change (Fig. 2). Under the current temperature thresholds (T1), extreme heat events across the nation show varying degrees of increase under the three emission scenarios, with the highest increase under the high-emission scenario (projected to exceed 120 days of extreme heat nationwide by 2100), whereas the increase under the low-emission scenario is more moderate, over half that under the high-emission scenario. Moreover, the frequency of extreme heat events significantly increases across all regions, particularly in the eastern, central and southern regions, as well as in the southwest (Fig. 2a,b). This intensification is especially pronounced under SSP5-8.5. By contrast, the increase in the number of extreme heat days is relatively small in the northern, northeastern and northwestern regions. Furthermore, the frequency of extremely cold days shows a decreasing trend nationwide, with three emission scenarios remaining at relatively low levels. Notably, when T0 is used as the temperature threshold, the frequency of extreme heat events shows a consistent increasing trend under SSP5-8.5. Moreover, the number of extremely cold days gradually decreased but remained relatively high, especially under SSP1-2.6. Under the T2 threshold, which is calculated iteratively, the frequency of extreme temperature events remains relatively stable, showing minimal changes over time.

a, The annual frequency of extreme heat events. b, The annual frequency of extreme cold events.
The impact of extreme heat shocks varies across regions, particularly under high-emission scenarios, in which the increasing frequency of extreme heat events in central, eastern and southern cities requires urgent attention. Furthermore, the disproportionate extreme heat events in the northwest and southwest also warrant vigilance.
Future temperature–hospitalization risks
This study assesses how future extreme temperature events affect hospitalization risk under different emission scenarios, highlighting health risk disparities across Chinese cities and age groups. The results indicate that, on the basis of the extreme threshold T1, the risk of excessive hospitalizations associated with extreme heat is projected to progressively increase from 2030 to 2100 across the three scenarios (Fig. 3a), whereas the risk from extreme cold is negligible and shows a declining trend (Fig. 3b). At the national level, the heat hospitalization risk is expected to increase from 2030 (SSP1-2.6: 0.006; SSP2-4.5: 0.028; and SSP5-8.5: 0.036) to 2100 (SSP1-2.6: 0.023; SSP2-4.5: 0.108; and SSP5-8.5: 0.153). As expected, the risk associated with the high-emission scenario SSP5-8.5 is the highest across all years, increasing by 4.2-fold. Moreover, if the human body gradually adapts to extreme temperatures (T2; Extended Data Fig. 10), the associated risks of extreme heat are projected to decrease by 2100 nationally, with the risk expected to decline to approximately 0.03.

a,b, Excess hospitalization risk of future extreme heat events (a) and extreme cold events (b) under three emission scenarios. c,d, Future excess hospitalization risk from extreme heat (c) and extreme cold (d) across three age groups under three emission scenarios.
The excess hospitalization risk varies by location and population (Fig. 3a,b). Under the high-emission scenario, the hospitalization risk rises from 0.046 to 0.178 in central, northwestern, southern and southwestern regions, and from 0.023 to 0.121 in the eastern, northern and northeastern regions. Under the low-emission scenario, the increases are more modest, from 0.006 to 0.024 and 0.006 to 0.020, respectively. Across all the scenarios, the impact remains relatively small in the eastern and northern regions, with overall hospitalization risks nearly half those of the other regions. Moreover, under T2, the increasing trend in heat-related risk was no longer apparent, while cold-related risk showed a decreasing trend in each regions (Extended Data Fig. 10). Excess risks from extreme temperatures vary by age group, with elderly populations (65 years of age and older) and children and adolescents (<18 years of age) being most vulnerable (Fig. 3c,d). In the southwestern and northwestern regions, risks are the highest for the elderly, whereas in the central, southern and eastern regions, both age groups face similarly high risks under higher-emission scenarios. Before 2030–2060, extreme cold has a limited impact in most areas, except for slight risks under medium- to low-emission scenarios in southern, northwestern and southwestern China.
Notably, when calculations are performed on the basis of fixed temperature thresholds (T0: 27.5 °C for hot temperatures, and 12.5 °C for cold temperatures), some intriguing observations emerge. Except for southern China, the risks associated with cold temperatures (below 12.5 °C) surpass those related to hot temperatures (above 27.5 °C) in all regions (Extended Data Fig. 9). In the southern regions, however, risks from cold are lower than those from heat, except under the low-emission scenario.
Future heat-related medical burdens
As Chinese cities face escalating and varied risks from extreme temperature events, it is imperative to address both current and prospective health care burdens. On the basis of calculations using average city-level hospitalization costs in China in 2021–2023, future excess hospitalization costs due to extreme heat are projected to rise—most sharply under the SSP5-8.5 scenario (Extended Data Fig. 11). Nationally, by 2100, excess costs are estimated at approximately USD 554 million under SSP1-2.6, 3,780 million USD under SSP2-4.5, and 5190 million USD under SSP5-8.5. Under SSP5-8.5, more than 5.1 million hospitalizations nationwide are projected to be hospitalized due to heat exposure (compared with 3.8 million under SSP2-4.5, and 0.6 million under SSP1-2.6), with the eastern, southern and southwestern regions showing relatively higher hospitalization counts among the seven regions (Extended Data Fig. 13). These increasing costs show disproportionate trends relative to projected regional gross domestic product (GDP) growth (Extended Data Fig. 11). Moreover, as shown in Extended Data Fig. 13, the number of hospitalized individuals due to high temperatures is projected to first increase and then decrease across different regions, with the inflection points varying by region. Under the SSP5-8.5 scenario, the rate of increase is notably faster.
The future heat-related HBEI is projected to rise progressively, with a complex geographical distribution (Fig. 4a). Hospitalization costs show an inverted U-shaped relationship with economic development, with moderately developed regions—particularly in the southwest—bearing the highest burdens. After 2070, the HBEI under SSP2-4.5 exceeds that under SSP1-2.6 and SSP5-8.5. This is because, although absolute excess hospitalization costs under SSP2-4.5 remain relatively low, GDP growth is also slower, resulting in a higher economic burden index (Extended Data Fig. 11). Furthermore, by incorporating city-level healthcare capacity—measured by the number of hospitals—this study examines how economic burdens relate to available medical resources under extreme temperature events (Extended Data Fig. 12).

a, The HBEI of heat-related hospitalizations in China in the years 2030, 2070 and 2100, reflecting the proportion of excess hospitalization costs due to extreme temperatures relative to the total GDP. The grey areas on the map indicate regions with no data. b, Heat-attributable HBEI across three age groups and multiple regions.
Under different emission scenarios, the future spatial distribution of heat-related HBEI across Chinese cities exhibits substantial variation, with clustering patterns in certain typical regions (Fig. 4a). Under the most optimistic scenario (SSP1-2.6), the increase in hospitalization burden is relatively mild (with most cities having an HBEI below 5), except for some cities in the southwestern region around 2070, in which the burden warrants attention. By contrast, under the most pessimistic scenario (SSP5-8.5), the spatial pattern of hospitalization burden is more dispersed and shows a gradual, outward spread of increasing burden. Starting from 2030, cities in the southwestern and northwestern regions will face relatively high hospitalization burdens (larger than 20 in some cities). Moreover, the northeastern region shows a notably higher burden than under SSP1-2.6. The intermediate scenario (SSP2-4.5) shows a broader and more complex distribution of high-burden areas. By 2030, cities in the northeast and central–southern Yangtze River Basin will begin to face greater medical burdens. By 2070, this trend intensifies, with high-burden zones expanding across the northeast and central regions, leading to greater spatial heterogeneity. By 2100, the situation changes more gradually, suggesting that under this scenario, temperature-related hospitalization burdens will affect a broader range of regions and pose increasing challenges.
Excess hospitalization burdens vary across regions and age groups (Fig. 4b). Under higher-emission pathways (SSP2-4.5 and SSP5-8.5), the population 65 years of age and older faces an absolutely higher burden across all regions. For that population, the national average HBEI is projected to rise from 2.4 in 2030 to 12.3 by 2100 under SSP5-8.5. By contrast, HBEI for the 0–18 years age group is very low, all at or below 1. Moreover, the southern and southwestern are projected to face a particularly high healthcare burden in the future—especially in the mid- to long-term—driven mainly by the ageing population, whereas the burden in the northeastern, northern and eastern regions remains relatively lower.
Discussion and implications
Moving beyond traditional single-focus analyses of temperature–health correlations, this research leverages a broader geographical context and hospital admission data to project future hospitalization risks and burdens under different climate change scenarios. Integrating analyses across five dimensions—spatial, disease, age group, temporal and emission pathways—it shows unexpected vulnerability patterns historically and integrates these with future projections. The findings highlight the complex spatial distribution of temperature-related hospitalizations and age-specific vulnerabilities, providing critical insights into climate-health impacts. Economic metrics further quantify societal costs, capturing both health damage and financial losses.
One of the key contributions of this study is the use of unique, high-resolution hospitalization data covering more than 7,000 hospitals at the Chinese city level to show the spatial distribution patterns of the relationships between various temperature indicators and hospitalization risk. This approach not only more accurately reflects the risks posed by varying temperature conditions across diverse climatic environments but also uncovers the impacts of extreme temperatures from the perspective of the health system process—specifically, at a stage before mortality outcomes. Importantly, from the city perspective, heat- and cold-related hospitalization risks exhibit complex spatial distributions, which may be attributed to the combined effects of environmental and climatic characteristics, as well as to the socioeconomic conditions of cities. Geospatial disparities in GRD heat vulnerability (Fig. 1a; gestation-related) mirror the ‘GRD Thermal Risk Demarcation Line’ (Extended Data Fig. 6), distinguishing heat-vulnerable northern cities from cold-prone southern regions. These patterns probably arise from compounded physiological stresses—elevated cardiovascular load and heat-induced placental dysfunction in third-trimester populations27. Although cold impacts are modest, this spatial stratification underscores the need for region-specific, climate-resilient maternal health strategies10.
Consistent with previous research19,21, less-developed regions bear greater climate-related healthcare burdens than developed areas. Our projections, incorporating future development disparities under SSPs, highlight these differential burdens. Notably, regions with either higher or lower levels of economic development face relatively smaller hospitalization burdens, potentially because of alignment between healthcare demands and resources: wealthier areas have superior infrastructure, whereas barriers to care access may suppress use in poorer regions. Cities with larger populations and higher levels of economic development (such as Beijing–Tianjin–Hebei, Yangtze River Delta and Pearl River Delta city clusters, which collectively account for nearly half of the national GDP and over a quarter of the population) face relatively lower excess hospitalization risks and burdens during extreme temperature periods. This phenomenon may be attributed to the fact that economically developed regions typically possess more abundant resources and well-established infrastructure, thus enabling their ability to effectively mitigate the negative impacts of climate change. By contrast, cities with larger populations but lower economic development (such as southwestern region of China, excluding Chongqing, which accounts for a relatively small share of the national GDP but more than 14–15% of the population and is characterized by mountainous and plateau terrains) experience significantly greater excess hospitalization risks and burdens, further exacerbating the pressure on their health care systems. Also consistent with previous studies, climate risks varied across age groups and diseases, probably because of differing sensitivities and response mechanisms. Although elderly populations are traditionally identified as most vulnerable, children and adolescents (0–18 years of age) in multiple urban centres also exhibit high heat sensitivity, linked to immature thermoregulatory and metabolic systems, increasing the risks of dehydration and electrolyte imbalance11,15,16,28. Analysis shows that individuals 65 years of age and older currently bear the greatest hospitalization burden, projected to worsen under SSP2-4.5, highlighting how ageing exacerbates health care burdens in this scenario.
Although the study focuses on China, its methodological framework and findings offer implications for global climate-health research and policy development. The varied temperature–hospitalization relationships across different geographic contexts—from coastal to inland regions and across different latitudinal and longitudinal gradients—provide valuable reference points for establishing global extreme climate health early warning systems tailored to diverse geographical characteristics. The findings demonstrate that regions with similar geographical or climatic conditions worldwide could benefit from comparable adaptation strategies, regardless of national boundaries. The economic stratification analysis of this study provides a universal framework for countries across different development stages to anticipate hospitalization burdens under climate change scenarios. Furthermore, the integrated methodological approach combining high-resolution hospitalization data with climate projections establishes a universal framework adaptable to diverse healthcare systems worldwide. This approach advocates for a collaborative global extreme climate health early warning collaboration system that transcends geographical, economic and political boundaries—in which region-specific vulnerability profiles inform resource allocation, whereas standardized metrics enable cross-regional comparison and collaboration.
The findings have several policy implications. Regional heterogeneity highlights diverse climate and economic impacts on health risks, suggesting city-level assessments. Hospitalization rates provide information on health management, prevention and early intervention strategies. Prospective results emphasize persistent health impacts due to temperature extremes, underscoring urgent mitigation efforts against global warming. Finally, global inequality highlights the necessity for international collaboration, as regions with limited resources disproportionately suffer from inadequate climate responses, stressing the need for a comprehensive, equitable global climate action framework.
This study uses high-resolution data from 301 Chinese cities to understand spatially heterogeneous temperature-related hospitalization risks and their future shifts under climate change and socioeconomic scenarios, with implications for targeted public health adaptation. These conclusions may be interpreted with some limitations. The temperature–hospitalization relationships are based on a relatively short observation period (2021–2023). Although this includes more than 1,000 daily data points per site and ensures robust current estimates, it assumes that exposure–response patterns remain stable over time. This approach may overlook future changes in population vulnerability, healthcare systems and adaptive capacity, potentially underestimating long-term resilience. Meanwhile, future studies should incorporate dynamic adaptation processes and broader environmental exposures, such as PM10, SO2, NO2 and CO, while accounting for possible multicollinearity. Moreover, examining finer demographic subgroups could reveal important variations in temperature-related health risks9.
Methods
Hospitalization data
This study collected hospitalization records covering more than 7,000 hospitals in China from the National Clinical Pathway Implementation Monitoring Platform of China. This dataset, which involves standardized clinical pathways, has been required for submission by all participating hospitals since 1 January 2021. The data indicators included demographic information (sex, age, admission time), hospitalization metrics (actual hospitalization days, medical payment method, health insurance settlement method) and 24 types of cost fields, including total hospitalization cost, out-of-pocket hospitalization cost and medical service fee. In the baseline analysis, this study established a ‘5 + 1’ CSD framework consisting of (1) five population-wide disease categories (from the International Classification of Diseases, 10th revision (ICD-10): circulatory diseases (I00–I99), respiratory diseases (J00–J99), endocrine, nutritional and metabolic diseases (E00–E90), psychiatric disorders (F00–F99 and genitourinary diseases (N00–N99)) represented by approximately 78 million data observations; and (2) a special maternal health cohort evaluating GRDs (ICD-10: O10–O16, O20–O29, O30–O48 and O60–O75). We used the ICD-10 version for standardized diagnostic classification. Age-stratified analyses were conducted across three subgroups (children and adolescents: 0–18 years of age; adults: 19–64 years of age; elderly: ≥65 years of age), with all subsequent analyses of temperature–hospitalization risk and age-specific effects pertaining to these five main categories of disease unless explicitly stated. Daily averages were processed across 301 prefecture-level cities from 1 January 2021 to 31 December 2023. These 301 cities emerged from a comprehensive data quality assessment, in which all cities with complete hospitalization records were included and deemed adequate for reliable temperature–hospitalization relationship estimation.
Meteorological data
Weather data were obtained from the National Meteorological Information Centre of China. The raw data include daily temperature metrics, precipitation and relative humidity. This study included 699 meteorological stations and adopted the inverse distance weighting method to derive daily weather data for each city. The process involved identifying geometric centres of each prefecture-level city, calculating distances between monitoring stations and city centres, and selecting stations within a 200-km radius. On the basis of inverse distance to the city centre, weighted averages of daily records were calculated.
Future data
Temperature data used for forecasting were sourced from the CMIP6 dataset, representing Phase 6 of the Coupled Model Intercomparison Project with extensive model participation and comprehensive experimental designs. This dataset covers both historical (1986–2014) and future (2015–2100) periods. Within the CMIP6 dataset, various experimental scenarios are shown through combinations of SSPs and representative concentration pathways. The three principal scenarios include (1) SSP1-2.6: low forcing scenario with 2.6 W m−2 radiative forcing by 2100; (2) SSP2-4.5: medium forcing scenario reaching 4.5 W m−2 by 2100; (3) SSP5-8.5: high forcing scenario leading to 8.5 W m−2 radiative forcing by 2100 (ref. 29).
Population projection
The SSPs describe alternative future trajectories of societal and economic development, and are widely used in Intergovernmental Panel on Climate Change assessment reports, climate and health research, and impact assessments. The gridded population projections for China from 2010 to 2099 under five SSPs at a resolution of 1 km × 1 km were extracted from the SSP spatial population scenario database30. Population projections for each district were computed by aggregating grid cell populations.
GDP projection
A set of gridded GDP projection data for Chinese cities was obtained, including historical data (represented by 2005) and future projections from 2030 to 2100 at decadal intervals for all five SSP scenarios31. These data used the LitPop approach to downscale the 2005 global national GDP and gross regional product of more than 800 provinces (in 2005 PPP dollars) to a spatial resolution of 30 arc seconds (approximately 1 km at the equator). The study downscaled national and supranational GDP growth projections under the three SSPs from 2030 to 2100 to a 1-km grid resolution.
Calculation of the frequency of future extreme temperature events
This study considers the temperature-related adaptability calculation, which included three main scenarios. The impacts of future extreme temperature events (2030–2100) were evaluated using threshold values derived from historical temperature data32,33. Three representative approaches for defining extreme temperature thresholds were considered.
Threshold 0 (T0)
This approach assumes that temperatures above 27.5 °C are categorized as hot, and those below 12.5 °C are categorized as cold34,35. Any temperature outside this range is considered nonoptimal. In this framework, the total number of days from 2030 to 2100 with daily mean temperatures exceeding 27.5 °C was counted as heat days, whereas the total number of days with temperatures below 12.5 °C was counted as cold days.
Threshold 1 (T1)
This approach uses the temperature distribution from the last 10-year period (2020–2029) to define thresholds. The 95th percentile of temperatures during this period served as the heat threshold, whereas the 5th percentile served as the cold threshold. These thresholds were fixed and applied consistently across future years. Any day between 2030 and 2100 with temperatures exceeding the heat threshold or falling below the cold threshold was classified as a heat or cold day, respectively. This scenario assumed no temperature adaptation, reflecting how current conditions would respond to future challenges.
Threshold 2 (T2)
In this approach, the thresholds for heat and cold were dynamically updated on the basis of the 10-year period immediately preceding each year of interest. For example, the heat and cold thresholds for 2030 were derived from the 2020–2029 temperature distribution, whereas those for 2050 were derived from the 2040–2049 distribution. A day was classified as a heat or cold day if its temperature exceeded or fell below the corresponding threshold for its preceding 10-year period. In this scenario, heat and cold thresholds vary with time, representing an adaptive process in response to evolving temperature conditions. Among these, only the T2 scenario is allowed for potential temperature adaptation.
Temperature effect measurements
This study developed a comprehensive three-dimensional framework to investigate the relationship between temperature effects and hospitalization. This framework encompasses temperature frequency effects, temperature intensity effects and temperature variability effects, each of which captures distinct aspects of temperature variations through mathematically defined metrics.
This analysis quantified frequency effects through two primary metrics. The first metric, extreme temperature days, measures the occurrence of extreme temperatures
where I(·) is an indicator function and P95 and P5 represent the 95th and 5th percentile temperature thresholds, respectively. The second metric, consecutive extreme days, measures the maximum duration of consecutive extreme temperatures:
Temperature intensity effects are quantified through two measures. The temperature deviation calculates the difference between the daily temperature and the average temperature over a time window:
The temperature range captures the maximum temperature variation within the time window:
For the temperature variability effects, two statistical measures were used. The temperature standard deviation is calculated as
The temperature coefficient of variation is expressed as a percentage:
In these formulations, i denotes the regional index, t represents the time index, w indicates the time window length and Tempi,d represents the temperature observed on day d before the time t. The ‘Threshold’ can be equal to either ‘Thresholdhigh’ or ‘Thresholdlow’, which represent the high and low temperature thresholds, respectively. This comprehensive framework allows us to systematically evaluate how different aspects of temperature variation affect hospitalization.
Distributed lag nonlinear model
This study used a DLNM model to estimate the impact of temperature exposure. The DLNM assesses the lag effects and nonlinear relationships of environment–exposure–response associations36. The hospitalization is not only related to the exposure level on the same day but may also be influenced by exposure over a longer period37,38,39.
First stage
Exposure–response and lag–response curves were calculated using time-series Poisson regression for specific cities. The basis function response equations are shown below:
where Yi,t denotes the number of hospitalizations in city i at time t, and α is the intercept term. S(t; β) is a time-smoothing function with parameter vector β to control for seasonal and long-term trends. γDowi,t denotes the day-of-week effect. cb(Tt; θ) is a cross-basis function of temperature, with parameter vector θ. We used a three-fold b-spline with eight degrees of freedom per year to control for seasonal and long-term trends, with weekly variables for cycle-specific effects. The exposure-response curve was modelled with a quadratic b-spline with interior knots at the 10th, 75th and 90th percentiles, whereas the lag-response curve used a natural cubic b-spline with knots at equally spaced logarithmic values. A 3-day lag period was specified on the basis of established literature. Considering the DLNM model setup, we selected 295 cities with no more than 20% overall missing data and no continuous gaps longer than 30 days to analyse the overall association across five disease categories. For individual diseases and age groups, cities meeting the same criteria were selected accordingly.
Second stage
City-specific results were pooled by multivariate meta-analysis to calculate the lowest-risk temperatures and attributable disease burdens. The analysis included environmental and socioeconomic cofactors (annual PM2.5 concentrations (particulate matter 2.5 μm or less in diameter), the resident population, education levels, healthcare infrastructure (hospital beds per capita), unemployment rates and economic development indicators (measured by GDP per capita)) as metapredictors. The empirical confidence intervals were calculated by Monte Carlo simulations.
Econometric model
A two-way fixed effects panel regression model estimated temperature effects on hospitalization:
where Ycd is the average hospitalization case for the c city group at date d, the independent variable is the mean temperature \({Meantemp}_{cd}^{\text{h}}\), and h denotes the different temperature bins. This analysis divided the distribution of city-level daily temperature, measured in degrees Celsius, into 9 bins: (below −7 °C), [−7 °C to −2 °C), [−2 °C to 3 °C), [3 °C to 8 °C), [8 °C to 13 °C), [13 °C to 18 °C), [18 °C to 23 °C), [23 °C to 28 °C) and [32 °C and above). The lowest and highest temperature bins represent extremely cold (below the 5th percentile of the temperature distribution) and extreme heat (above the 95th percentile of the distribution), respectively. The temperature bin [8 °C −13 °C) is considered the optimal temperature and is excluded from the model as a reference group to avoid perfect multicollinearity. This semiparametric approach imposes minimal restrictions and allows for a flexible estimation of the nonlinear effects of temperature on costs. To illustrate, the (below −7 °C) bin equals 1 if the daily temperature falls within this range and equals 0 otherwise, thereby measuring the marginal effects of each temperature bin relative to the optimal temperature. Owing to the small number of missing values in the data, we excluded only some of the extreme values in our econometric model to ensure data completeness. The analysis was conducted on the basis of data from 301 cities.
Considering that the short-term impact of temperature on costs is endogenous, this study discussed various specifications to identify its causality as accurately as possible. First, to avoid omitted variable bias, this process sequentially added a series of control variables related to both temperature and medical costs into the model, where Xcd represents a set of weather-related variables such as precipitation, relative humidity and wind speed, and Pollucd represents a set of air pollution-related variables, including PM2.5 and ozone emissions. Second, in some specifications, to account for the serial correlation of temperature and to disentangle the effects of specific dates from the cumulative effects of past temperatures, 21 temperature lags were incorporated into the model. These lags were identified in the same semiparametric manner using temperature bins. Moreover, to better capture cumulative effects, the temperature bin lags were replaced with continuous linear temperature lags. The cumulative effect over the exposure window was assessed by aggregating the lagged coefficients and applying joint significance tests, which allowed evaluation of the overall impact of temperature across multiple lags.
Furthermore, this analysis controlled for time fixed effects and city fixed effects to restrict time trends and adjust for regional differences. Time fixed effects control for confounding factors that vary over time but are constant across cities, such as national policies, economic shocks or broad seasonal trends. City fixed effects adjust for time-invariant regional differences and baseline climate characteristics, thus ensuring that the model captures within-city variations in temperature rather than between-city differences. As time fixed effects may not fully account for short-term fluctuations such as seasonal variations or weekly cyclical patterns, this study also included seasonal and weekday dummy variables. These variables address more granular fluctuations that time fixed effects might miss, providing a more robust model.
Hospitalization burden economic index (HBEI)
The HBEI is calculated as the ratio of hospitalization costs attributed to extreme temperatures in a specific region to the adjusted GDP of the region (GDP minus hospitalization costs). This study considers the proportion of an individual’s medical expenses relative to their remaining disposable income as a measure of financial burden40,41,42. The hospitalization costs are calculated by multiplying the disease excess hospitalizations due to heat and cold by the average hospitalization cost. The average hospitalization cost is calculated on the basis of the mean of inpatient expenses due to CSDs from 2021 to 2023 and is determined separately for each subgroup.
City level
The average hospitalization cost for each of the five major disease categories was calculated across all individuals within the observation period.
Age group level
The average cost for each age group was calculated on the basis of city-specific hospitalization data for different age groups. The GDP levels of each region are based on the total GDP values obtained through projections. The ratio is then multiplied by 10,000 to standardize the values for easier interpretation, as regional total GDP is typically on the scale of trillions. Under this calculation, the HBEI represents the contribution of hospitalization costs due to extreme heat or cold to the total city GDP. Generally, a lower HBEI during extreme events indicates a lower resilience of the city or population to such events, whereas a higher HBEI suggests greater adaptive capacity or emergency response capability.
Moreover, this study acknowledges that the hospitalization cost estimates in this study are based on current expenditure levels, whereas future hospitalization costs are influenced by a range of additional factors, such as advances in medical technology, policy and regulatory changes, and climate change itself43,44. Therefore, alongside projecting future hospitalization costs associated with extreme heat, this analysis also calculated 95th percentile confidence intervals for hospitalization costs related to five major CSD categories under three carbon emission pathways, accounting for future climate change scenarios. This study clarified that the calculations do not incorporate assumptions regarding technological progress or other adaptive measures. Furthermore, in HBEI calculation, this study replaced the projected excess hospitalization costs due to heat with the projected excess number of hospitalizations to assess the robustness of the HBEI. This approach acknowledges that, beyond the financial burden, a sudden surge in patient numbers within a short time frame can severely affect hospital services, compromise urban public health systems, and challenge the overall resilience of cities.
Forecasting methods
The specific methods for forecasting changes in medical burden due to extreme temperatures involve the following three steps.
First, a two-step DLNM was applied to elucidate the exposure–response relationship between daily average temperatures in domestic prefecture-level cities and the corresponding number of hospitalizations. Here, the abovementioned DLNM is fully applied to the existing data for city-specific training, and parameter estimates are generated as outputs.
Second, the temperature was projected using global climate models (GCMs). The temperature projections are derived from 12 GCMs. The China Regional Surface Meteorological Element Driving Dataset (CMDF) grid precipitation and temperature data are used as observational references. The temperature data from these models are subjected to bias correction through the equidistant cumulative distribution function method following bilinear interpolation to a 0.25° grid, yielding daily average temperature data for each city under various SSP scenarios. This study used 12 GCM models to calculate the projected daily mean temperature for each city from 2030 to 2100. The GCM models applied include KACE-1-0-G, NorESM2-MM, NorESM2-LM, INM-CM5-0, INM-CM4-0, TaiESM1, MRI-ESM2-0, MPI-ESM1-2-HR, IPSL-CM6A-LR, GFDL-CM4 and CanESM5,FGOALS-g3. This multimodel approach helps mitigate the instability associated with relying on a single GCM and enhances the robustness of the temperature projections.
Finally, health indicator estimation was performed by incorporating the improved temperature data into the initial exposure–response model to estimate the impact of temperature changes on the number of relevant hospitalizations under different SSP scenarios. On the basis of the DLNM temperature–hospitalization relationship, this study calculated the daily historical and future numbers of temperature-attributable hospitalizations Htemp on any day with daily mean temperatures above Tmm as follows:
where f* denotes the overall cumulative temperature–hospitalization association derived from the bidimensional term in the adjusted DLNM estimation, \({\text{proj}}_{* }^{T}\) represents the projected temperature series and H represents the total number of hospitalizations for a given area, either overall or disaggregated by population group and disease. The number of hospitalizations attributable to temperatures was calculated by summing subsets of days with temperatures above Tmm. This calculation separated components due to heat and cold by summing the subsets corresponding to days with temperatures higher or lower than Tmm.
Decadal temperature-related excess hospitalization was separately estimated for each city and for combinations of SSPs and GCMs. Subsequently, attributable fractions (namely, excess hospitalization risk) as GCM-ensemble means according to region, hospitalizations and the SSPs were further calculated using the corresponding total number of hospitalizations as the denominator.
Uncertainty analysis
The uncertainties in projecting future temperature-related hospitalizations primarily stem from the temperature–hospitalization relationship, the variation in temperature projections across different GCMs and population projections. The uncertainty in projected populations was addressed using three SSPs that encompass high-, medium- and low-emission pathways.
Vulnerable subgroups and population ageing
To identify future hot- and cold-temperature-susceptible subgroups, this study conducted the above analyses by disease, age and sex. On the basis of the temperature–hospitalization relationships within each subgroup, it projected the attributable proportions and number of hospitalizations under future hot- and cold-temperature conditions. Specifically, future estimates of hospitalizations for various population groups (0–18 years of age, 19–64 years of age, and 65 years of age and older; male and female) and for different diseases rely on linear projections derived from the 2022 city-level hospitalization data collected by the National Health Commission, along with nationwide hospitalization rates for each demographic and disease group and future population projections under the three SSP scenarios.
Ethical approval statement
This study was approved by the Medical Ethics Committee, Zhongnan Hospital of Wuhan University (approval no. 2024297 K, approval date: 10 December 2024). All procedures adhered to the ethical standards of this committee and applicable national regulations.
Reporting summary
Further information on research design is available in the Nature Portfolio Reporting Summary linked to this article.
Data availability
The national hospitalization data are confidential and obtained from the National Health Commission of China. To enhance transparency while adhering to data protection policies, we have publicly released city-level daily hospitalization counts and average hospitalization costs, with all city names anonymized and replaced by coded identifiers. All shared data are accessible at Zenodo45 (https://doi.org/10.5281/zenodo.16757996). Meteorological data were obtained from the ECMWF ERA5 dataset (https://cds.climate.copernicus.eu/cdsapp#!/dataset/sis-agrometeorological-indicators?tab=overview). The temperature data used for forecasting were sourced from the CMIP6 dataset (https://cds.climate.copernicus.eu/datasets/projections-cmip6?tab=overview). The population projection data were derived from publicly available data in a research paper (https://cloud.tsinghua.edu.cn/f/d593f46793fb4145b8b9/?dl=1). The GDP projection data were obtained from publicly available data at Zenodo46 (https://doi.org/10.5281/zenodo.5880037). Other economic and geographic information related to Chinese cities was sourced from the National Bureau of Statistics of China (https://www.stats.gov.cn/sj/ndsj/).
Code availability
This study conducts a historical analysis of the relationship between temperature and hospitalizations using the DLNM approach. It further implements extreme weather projections based on three different temperature threshold calculation methods to assess future climate impacts. These analyses project health risks under extreme heat and cold conditions for each city over 2030–2100. Finally, it estimates the excess medical burden by integrating the projected hospitalization risks with the future population and GDP projections, providing a comprehensive assessment of the potential healthcare challenges associated with climate change. All of the codes can be accessed at Zenodo45 (https://doi.org/10.5281/zenodo.16757996).
References
Carleton, T. A. & Hsiang, S. M. Social and economic impacts of climate. Science 353, aad9837 (2016).
Campbell-Lendrum, D., Neville, T., Schweizer, C. & Neira, M. Climate change and health: three grand challenges. Nat. Med. 29, 1631–1638 (2023).
Wong, C. Climate change is also a health crisis — these 3 graphics explain why. Nature 624, 14–15 (2023).
Rising, J., Tedesco, M., Piontek, F. & Stainforth, D. A. The missing risks of climate change. Nature 610, 643–651 (2022).
Gasparrini, A. et al. Mortality risk attributable to high and low ambient temperature: a multicountry observational study. Lancet 386, 369–375 (2015).
Romanello, M. et al. The 2023 report of the Lancet Countdown on health and climate change: the imperative for a health-centred response in a world facing irreversible harms. Lancet 402, 2346–2394 (2023).
Alahmad, B. et al. Associations between extreme temperatures and cardiovascular cause-specific mortality: results from 27 countries. Circulation 147, 35–46 (2023).
Mahon, M. B. et al. A meta-analysis on global change drivers and the risk of infectious disease. Nature 629, 830–836 (2024).
Chersich, M. F. et al. Associations between high temperatures in pregnancy and risk of preterm birth, low birth weight, and stillbirths: systematic review and meta-analysis. Br. Med. J. 371, m3811 (2020).
Lakhoo, D. P. et al. A systematic review and meta-analysis of heat exposure impacts on maternal, fetal and neonatal health. Nat. Med. 31, 684–694 (2025).
Hajat, S. et al. Ambient heat and acute kidney injury: case-crossover analysis of 1 354 675 automated e-alert episodes linked to high-resolution climate data. Lancet Planet. Health 8, E156–E162 (2024).
Peters, A. & Schneider, A. Cardiovascular risks of climate change. Nat. Rev. Cardiol. 18, 1–2 (2021).
Bell, M. L., Gasparrini, A. & Benjamin, G. C. Climate change, extreme heat, and health. N. Engl. J. Med. 390, 1793–1801 (2024).
Callaghan, M. et al. Machine-learning-based evidence and attribution mapping of 100,000 climate impact studies. Nat. Clim. Change 11, 966–972 (2021).
Dimitrova, A. et al. Temperature-related neonatal deaths attributable to climate change in 29 low- and middle-income countries. Nat. Commun. 15, 5504 (2024).
Zhang, H. et al. Unequal urban heat burdens impede climate justice and equity goals. Innovation 4, 100488 (2023).
Zangerl, K. E. et al. Child health prioritisation in national adaptation policies on climate change: a policy document analysis across 160 countries. Lancet Child Adolesc. Health 8, 532–544 (2024).
Deivanayagam, T. A. et al. Envisioning environmental equity: climate change, health, and racial justice. Lancet 402, 64–78 (2023).
Grimm, N. B. et al. Global change and the ecology of cities. Science 319, 756–760 (2008).
Bai, X. et al. Six research priorities for cities and climate change. Nature 555, 23–25 (2018).
Wu, Y. et al. Fluctuating temperature modifies heat-mortality association around the globe. Innovation 3, 100225 (2022).
Yin, P. et al. Projection of mortality burden attributable to nonoptimum temperature with high spatial resolution in China. Environ. Sci. Technol. 58, 6226–6235 (2024).
Braithwaite, J. et al. Analysing health system capacity and preparedness for climate change. Nat. Clim. Change 14, 536–546 (2024).
Al-Marwani, S. Climate change impact on the healthcare provided to patients. Bull. Natl Res. Cent. 47, 51 (2023).
Kephart, J. L. et al. City-level impact of extreme temperatures and mortality in Latin America. Nat. Med. 28, 1700–1705 (2022).
He, Y.-S. et al. Time trends in the burden of environmental heat and cold exposure among children and adolescents. JAMA Pediatr. 179, 59–64 (2025).
Bonell, A. et al. Environmental heat stress on maternal physiology and fetal blood flow in pregnant subsistence farmers in The Gambia, West Africa: an observational cohort study. Lancet Planet. Health 6, E968–E976 (2022).
Yao, X. et al. Elderly vulnerability to temperature-related mortality risks in China. Sci. Adv. 11, eado5499 (2025).
O’Neill, B. C. et al. The Scenario Model Intercomparison Project (ScenarioMIP) for CMIP6. Geosci. Model Dev. 9, 3461–3482 (2016).
Zhang, S. et al. City-level population projection for China under different pathways from 2010 to 2100. Sci. Data 10, 809 (2023).
Wang, T. & Sun, F. Global gridded GDP data set consistent with the shared socioeconomic pathways. Sci. Data 9, 221 (2022).
Guo, Y. et al. Global variation in the effects of ambient temperature on mortality: a systematic evaluation. Epidemiology 25, 781–789 (2014).
Zhang, X. et al. Indices for monitoring changes in extremes based on daily temperature and precipitation data. WIREs Clim. Change 2, 851–870 (2011).
Colelli, F. P., Emmerling, J., Marangoni, G., Mistry, M. N. & De Cian, E. Increased energy use for adaptation significantly impacts mitigation pathways. Nat. Commun. 13, 4964 (2022).
De Cian, E. & Sue Wing, I. Global energy consumption in a warming climate. Environ. Resour. Econ. 72, 365–410 (2019).
Zhang, S. et al. Heat and cause-specific cardiopulmonary mortality in Germany: a case-crossover study using small-area assessment. Lancet Reg. Health Eur. 46, 101049 (2024).
García-León, D. et al. Temperature-related mortality burden and projected change in 1368 European regions: a modelling study. Lancet Public Health 9, E644–E653 (2024).
Liu, C. et al. Ambient particulate air pollution and daily mortality in 652 cities. N. Engl. J. Med. 381, 705–715 (2019).
Chen, G. et al. All-cause, cardiovascular, and respiratory mortality and wildfire-related ozone: a multicountry two-stage time series analysis. Lancet Planet. Health 8, E452–E462 (2024).
OECD. OECD Framework for Statistics on the Distribution of Household Income, Consumption and Wealth (OECD, 2013).
McIntyre, D., Thiede, M., Dahlgren, G. & Whitehead, M. What are the economic consequences for households of illness and of paying for health care in low- and middle-income country contexts? Social Sci. Med. 62, 858–865 (2006).
Xu, K. et al. Protecting households from catastrophic health spending. Health Aff. 26, 972–983 (2007).
Watts, N. et al. Health and climate change: policy responses to protect public health. Lancet 386, 1861–1914 (2015).
Kinney, P. L. Climate change, air quality, and human health. Am. J. Prev. Med. 35, 459–467 (2008).
Wei, P., Li, W. & Rongkai, C. Temperature-related hospitalization burden under climate change. Zenodo https://doi.org/10.5281/zenodo.15752585 (2025).
Wang, T. & Sun, F. Gross domestic product (GDP) downscaling: a global gridded dataset consistent with the Shared Socioeconomic Pathways. Zenodo https://doi.org/10.5281/zenodo.5880037 (2022).
Acknowledgements
We thank the National Clinical Pathway Implementation Monitoring Platform of China for their support in data collection and organization during this study. We are grateful to the National Health Commission Medical Management and Service Guidance Center and the Hospital Management Institute, Wuhan University, for their valuable guidance on the study. This research was funded by the National Natural Science Foundation of China (grant nos. 72474218, 82341120, 82372354, 72202229 and 72325008).
Author information
Authors and Affiliations
Contributions
X.W., W.P. and S.L. designed and supervised the study. L.W. and R.C. conducted the study, collected the data, analysed the results and drafted the paper. D.P., R.W., C.H., J.R. and H.W. provided calculations and writing related to the economics model, disease and public health. C.T. collected and processed the meteorological and temperature data and drafted the paper. Y.Z. collected and processed the population data and other data collected. D.P., X.M., X.Z. and H.D. provided guidance on the analysis and assessment of health and medical burden. R.C., L.W. and W.K. guided the uncertainty analysis and validation.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Peer review
Peer review information
Nature thanks the anonymous reviewers for their contribution to the peer review of this work.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Extended data figures and tables
Extended Data Fig. 1 Disease differences in the relative risk of extreme heat versus extreme cold in cities in different regions.
RRs of hospital admissions at the 95th (a) and 5th (b) percentile temperatures for five different disease categories—circulatory, respiratory, endocrine/metabolic, psychiatric, and genitourinary diseases—across 21 provincial capital cities in China. The top panel displays the RRs of extremely high temperatures (95th percentile), whereas the bottom panel shows the RRs of extremely low temperatures (5th percentile). Each point represents the estimated RRs for a specific disease category, providing a detailed analysis of how extreme temperatures impact hospital admissions for different health conditions.
Extended Data Fig. 2 Sex differences in the relative risk of extreme heat versus extreme cold in cities in different regions.
The vertical axis of the figure is RRs. The figure presents RRs of hospital admissions at the 95th (a) and 5th (b) percentile temperatures for males and females across 21 provincial capital cities selected from the seven geographic regions in China. Each point represents the estimated RRs for males and females, allowing for comparisons between sexes and across different cities.
Extended Data Fig. 3 Sex differences in the relative risks of extreme heat versus extreme cold across cities.
Relative risks of hospital admission for males under extreme heat (a) versus extreme cold (b) and females under extreme heat (c) versus extreme cold (d) in Chinese cities.
Extended Data Fig. 4 Relative risks of extreme heat versus extreme cold in 21 provincial capitals.
Relative risks of hospitalization at the 95th percentile (extreme heat) and 5th percentile (extreme cold) temperatures for each city grouped by region.
Extended Data Fig. 5 Hospital admissions across temperature percentiles by age group.
The x-axis represents temperature percentiles, with lower percentiles (colder temperatures) on the left and higher percentiles (warmer temperatures) on the right. The y–axis shows the number of hospital admissions, with different age groups distinguished by color.
Extended Data Fig. 6 Impact of temperature on hospital admission for gestation–related diseases (GRDs).
Geographic distribution of extreme temperature–associated hospitalization risks for GRDs across Chinese cities, showing extreme heat (a) and cold (b) patterns. (a) GRDs thermal risk demarcation line for extreme heat, where cities north of this threshold (red dashed line) (~31°N) present elevated relative risks for GRDs hospitalizations. (b) GRDs thermal risk demarcation line of extreme cold, with cities south of this threshold (blue dashed line) (~39°N) demonstrating increased cold–associated risk.
Extended Data Fig. 7 Projected temperature trends over time in China.
Future temperature change trends across different regions under three emission scenarios.
Extended Data Fig. 8 Future temperature thresholds.
Future temperature thresholds across different regions are calculated via three evaluation methods for extreme temperatures, a for heat and b for cold.
Extended Data Fig. 9 Future excess hospitalization risks attributed to temperatures under T0.
(a) Heat-related temperatures and (b) cold-related temperatures.T0, above 27.5 °C and below 12.5 °C.
Extended Data Fig. 10 Future excess hospitalization risks attributed to temperatures under T2.
(a) Heat-related temperatures and (b) cold-related temperatures.T2, temperature thresholds change annually, assuming a trend of temperature adaptation.
Extended Data Fig. 11 Future regional excess hospitalization costs and GDP (Unit: RMB, T1, no adaptation).
a represents the excess heat–related costs, and b represents the GDP under different carbon emission scenarios.
Extended Data Fig. 12 Relationship between HBEI and hospital availability under extreme heat across three emission scenarios.
Number of Hospitals represents the total number of hospitals in each city, while Number of Class III Hospitals refers to tertiary hospitals, which provide more comprehensive and higher-quality medical care.
Extended Data Fig. 13 Excess hospitalizations attributable to extremely hot and cold temperatures across different regions.
Here, the unit label on the y-axis uses “K” to denote thousands, whereas “M” denotes millions.
Supplementary information
Supplementary Information
This file contains Supplementary Text (sections 1–8), Supplementary Tables 1–6 and Supplementary References.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Liao, S., Pan, W., Wen, L. et al. Temperature-related hospitalization burden under climate change. Nature 644, 960–968 (2025). https://doi.org/10.1038/s41586-025-09352-w
Received:
Accepted:
Published:
Version of record:
Issue date:
DOI: https://doi.org/10.1038/s41586-025-09352-w
This article is cited by
-
Why water security matters to cities under extreme heat in the Global North
npj Urban Sustainability (2026)
-
Mobile observation in urban environmental monitoring: theory, methods, and applications
International Journal of Environmental Science and Technology (2026)
