
Abstract
The German Center for Diabetes Research (DZD) established a core data set (CDS) of clinical parameters relevant for diabetes research in 2021. The CDS is central to the design of current and future DZD studies. Here, we describe the process and outcomes of FAIRifying the initial version of the CDS. We first did a baseline evaluation of the FAIRness using the FAIR Data Maturity Model. The FAIRification process and the results of this assessment led us to convert the CDS into the recommended format for spreadsheets, annotating the parameters with standardized medical codes, licensing the data set, enriching the data set with metadata, and indexing the metadata. The FAIRified version of the CDS is more suitable for data sharing in diabetes research across DZD sites and beyond. It contributes to the reusability of health research studies.
Similar content being viewed by others
Introduction
The German Center for Diabetes Research (Deutsches Zentrum für Diabetesforschung - DZD) conducts large clinical multicenter studies in the field of diabetes and metabolic research1. It is part of the German Centers for Health Research (Deutsche Zentrender Gesundheitsforschung - DZG) which focus on novel therapies for diabetes, infections, lung diseases, cancer, mental disorders, cardiovascular and neurodegenerative diseases2,3,4,5,6,7. In this vein, a core data set (CDS) provides the descriptions of variables and definitions that are relevant for clinical research in an information database for purposes of consistency, data validity and reliability8,9. Analysis of clinical data integrated from multiple sources has been used to generate critical information that supports clinical research10,11. Data exchange among different levels of healthcare is also linked to better health service management and improved care for persons with diseases12. However, the use of heterogeneous systems to collect different types of data, typically maintained in various formats, impedes both data exchange and consolidative data analysis for research10,12.
A CDS is typically presented to the audience in human-readable format to help the end-user properly interpret the meaning of the associated data13. Machine-readable formats are designed to allow computers to easily process the data, which requires the data to be structured in a specific and standardized way14. Machine-readable formats also support data encoding and exchange between heterogeneous systems to facilitate reporting and standard queries15. The development of a CDS in various scientific spheres has shown to be a valuable component when sharing or integrating complex data from multiple data sources across different systems16. The design of a CDS enables harmonization and standardization in the collection, measurement and reporting of minimal information necessary for collaborative research17. For example, the CDS for the German Medical Informatics Initiative and the NFDI4Health Metadata Schema both employ a standardized framework to capture essential information, promote consistency, efficiency and comparability in data management and analysis18,19.
In 2021 the DZD established a CDS containing a list of clinical parameters relevant for joint studies in diabetes research20. The DZD CORE DATA SET (DZD CDS) is designed as the core component of clinical studies conducted by the DZD. A detailed description of each parameter contributes to standardization of data collection and ensures that the data is uniformly designated, defined, and recorded in the same format across studies. The first version of the DZD CDS was published for internal use on the DZD website and has since become a mandatory component for the design of all new DZD clinical studies20,21. To date, the DZD CDS has already been implemented in various DZD studies such as the Influence of intermittent fasting on insulin secretion (IFIS), ClinicalTrials.gov ID: NCT04607096 and the SGLT2 Inhibition in Addition to Lifestyle Intervention and Risk for Complications in Subtypes of Patients With Prediabetes (LIFETIME), ClinicalTrials.gov ID: NCT0605403522,23. It serves to contribute to the harmonization of data for diabetes research in general, thus the need to enhance its sustainability, reproducibility and shareability. Work is underway to establish a common CDS across the German Centers for Health Research (DZG). The parameters of this overarching core data set are published in the Medical Data Models (MDM) portal and will be part of the next version of the DZD CDS24.
The implementation of a formalised, provenance-enabled and semantically enriched representation of (meta)data leads to more findable, accessible, interoperable and reusable (FAIR) data25. The metadata adds value to data and saves time spent on data exploration, data selection during access and data processing which is key to realising the full capabilities of research25,26. The primary goal of this work was to enhance the value of the DZD CORE DATA SET (DZD CDS) through a two-fold approach: first, by conducting a baseline FAIR assessment, followed by implementing targeted FAIRification measures. As a result, a FAIRer version of the DZD CDS has been developed which is the main success benchmark of this work. The FAIRification process was imperative for both the data proprietors and diabetes research community, as it facilitates improved data management and sharing capabilities.
Methods
We started our FAIRification journey by conducting a baseline assessment of the following FAIR aspects:
-
1.
Findability: How searchable and findable are the DZD CDS items for users and across future versions of DZD CDS?
-
2.
Accessibility: Are the protocols for retrieving the DZD CDS explicit? Do they include well-defined mechanisms to obtain authorization for access to protected data?
-
3.
Interoperability: Are the items in DZD CDS annotated with terms from biomedical ontology terms to support interoperability? Do these annotations include data standards, terminologies and a structured format to enable the automatic extraction of relevant data items across future versions of the DZD CDS?
-
4.
Reusability: Is the DZD CDS presented in a manner concise enough to allow for reuse across all the different future DZD CDS versions and for different studies?
The results of the baseline assessment were used to determine the direction the FAIRification efforts ought to take, facilitate the planning for the various resources that the FAIRification journey would require and motivate the various stakeholders to engage in this journey. This section describes the resources and methods used to FAIRify the DZD CDS.
The Research Data Alliance FAIR Data Maturity Model
The Research Data Alliance (RDA) was established in 2013 as an international community that aims to address the growing global need for research infrastructure that allows for data sharing across technologies, disciplines, and countries27. The RDA working group for a “FAIR data maturity model” was founded in 2019 to develop a common set of core assessment criteria for FAIRness28. It established a set of FAIR indicators and related maturity levels. This further led to a set of guidelines and a checklist related to the implementation of the FAIR indicators which are useful for evaluating data FAIRness as shown in the following Table 129. The RDA indicators have been prioritised as follows30:
-
1.
Essential: The aspect of this indicator is paramount to achieving data FAIRness. Data FAIRness cannot be achieved without satisfying this indicator.
-
2.
Important: Though the aspect of this indicator is not paramount, satisfying it would significantly increase data FAIRness.
-
3.
Useful: The aspect of this indicator is nice-to-have but is not indispensable.
Several tools based on a range of different interpretations of FAIR have been developed to assess data FAIRness in different fields of research30,31. The FAIR Data Maturity Model (FDMM) was developed by the RDA as a harmonized set of assessment criteria to assess data FAIRness across the various fields of research30. Today it is a community-recognized comprehensive standard for manual FAIR assessment32,33. There are two ways of ‘scoring’ the FAIRness of a given resource using these indicators: The first approach scores the progress made per indicator on a five-level scale, while the second assigns a yes/no score to each indicator. The indicators are scored against five levels of compliance based on the degree to which the FAIR principles are implemented as shown in the following Table 234.
In this work the RDA-FDMM approach with five levels of compliance has been used to conduct the FAIR assessment of the DZD CDS. We chose this method because it allowed us to gives the possibility to ‘discard’ the data indicators and focus more on the metadata indicators. It also allowed us to self-assess the evolution of the DZD CDS FAIRifcation journey so as to get a better idea on where to concentrate efforts for a FAIRer outcome. The baseline evaluation has been performed on the former version of the DZD CDS1,20. We then used the results of this evaluation to inform our FAIRification journey. Finally, we conducted a second FAIR assessment using the RDA-FDMM to evaluate the FAIRness of the DZD CDS after our FAIRifaction efforts. For purposes of this task, we only scored the RDA-FDMM indicators that addressed the metadata elements which are 26 out of 41. It is important to note that the RDA has indicated that a FAIR evaluation based on the RDA-FDMM should not be conceived as a value judgment but rather as guidance towards improvement of the level of data FAIRness30.
Data Records
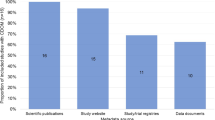
The concepts of the DZD CDS are represented in eight modules which include: master data (biodata), anthropometry, vital signs, laboratory, diabetes data, medical history, comorbidities and questionnaires. The modules consist of 126 items. The CDS also has additional optional modules for investigations that are only relevant for special studies. The data types include dates, integers, text (string), floats and booleans. A detailed description of each parameter contributes to the standardization of data collection and ensures that all data are uniformly labeled, defined, and recorded in the same format across all the DZD clinical studies. This is a prerequisite for the comparability of data from one study to another. A representation of the DZD CDS modules and variable proportions is shown in the following Fig. 1.

DZD CDS Data Records (Base Set).
Results
This section describes the state of the DZD CDS before FAIRification, the steps taken to FAIRify it, how we implemented these steps and the final FAIRified state of the DZD CDS.
Findability
Former DZD CDS Findability
For purposes of enhanced findability the DZD CDS was published on the DZD website and retrievable through a uniform resource locator (URL)1,20. However, this valuable DZD resource was neither registered in a searchable resource nor permanent. More work needed to be done to make the CDS findable in a registry. The metadata contained in the CDS was not standardized and it largely consisted of only the title and the contributors to the data set. There was neither readme nor provenance information provided alongside the data set. Based on this, both the RDA-F1-01M and RDA-F4-01M indicators scored 1 at the FAIR baseline assessment. The RDA-F2-01M scored 2. The RDA-F2-01M indicator scored 3 while the RDA-F1-02M scored 4. The RDA-F3-01M indicator was not applicable in this case.
Recommendations based on former state
The need to move the online location of the CDS specification should not require any change in the original URL. Therefore a persistent URL i.e a PURL, is required which then provides a stable, fixed URL that is set to point to content which may be periodically modified35,36. Further work is needed to include more metadata in the CDS description to improve its semantic interoperability. This includes enriching the metadata with information about the date on which the data set was completed, contextual information, target audience, keywords that describe the data, license, temporal coverage, spatial coverage, related data sets/resources, file formats used in the data set. The metadata and the data set they describe may be separate files but the persistent identifier (PID) should be explicitly stated in the metadata as indicated in the list of recommended metadata provided. Related readme and provenance information should be provided alongside the data set. The metadata should also include relevant domain specific controlled vocabularies, taxonomies and ontologies. Finally, more work is also needed to register or index the metadata in a searchable resource.
Improvements Implemented
The DZD CDS was shared at the MDM portal under ID 45923 and Digital Object Identifier (DOI) [https://doi.org/10.21961/mdm:45923] as shown in Fig. 237,38. An example for the exploration of the base set of the CDS in the MDM-Portal is found in Fig. 3. The MDM portal is a registered European information infrastructure which provides a multilingual platform for harmonization and exchange of medical data models for medical research for purposes of improving health outcomes37. This allows for a PID, versioning and tagging with keywords. It also provides a human-readable description and data type of each data element. Additional metadata and a standard operating procedure (SOP) containing adequate detail to guide research staff through the procedures of the CDS were registered in Zenodo where it was versioned and a DOI was assigned21,39. The DOIs on MDM and Zenodo are linked to machine-readable metadata which allows identifiers to stay persistent even after semantic information changes. Codes from the Unified Medical Language System (UMLS) were used to annotate all parameters of the DZD CDS40. The addition of metadata in this manner contributes to an overall increased visibility of the DZD CDS. Related readme and provenance information containing the data origin, citations for reused data, description of the data collection, data processing history and version history of the data have been provided alongside the data set. These implementations improved the findability of the DZD CDS. All findability-related metadata indicators scored 4 at the final FAIRness assessment, except RDA-F3-01M which is not applicable in this case.

DZD CDS in the MDM portal’s information section with description of the dataset and overview of the model.

DZD CDS Base Set exploration in the MDM portal. An example for download possibility and details about the modules of the base set.
Accessibility
Former DZD CDS Accessibility
The former version of the DZD CDS was retrievable by ‘clicking on an internet link’ (URL) that is a high-level interface to a low-level protocol that the computer executes to load data in the user’s web browser. The retrieval of the DZD CDS from this URL did not require further mediation by specialised or proprietary tools. This universally implementable protocol also allows for an authentication or authorisation procedure if necessary41. The data set which does not contain any personal data was not licensed. Based on this, both the RDA-A1-02M and RDA-A1.1-01M indicators scored 4 while the RDA-A2-01M, RDA-A1-03M and RDA-A1-04M indicators scored 1 at the FAIR baseline assessment. The RDA-A1-01M indicator was not applicable in this case.
Recommendations based on former state
Once the DZD CDS is no longer available online it is likely that the URL will become invalid and both humans and machines will no longer be able to access the data set. This creates the need to ensure the persistence of the metadata even after the core data set is no longer available by storing it in a relevant repository. The data set should be licensed.
Improvements Implemented
Registering the additional metadata and SOP in the MDM portal and Zenodo allows the metadata to remain persistently accessible even after the CDS is no longer available21,41. As the data set does not contain personal data, an open licence was chosen with the help of a tool developed by the Creative Commons that helps the data owner choose an appropriate data license42. These implementations increased the accessibility of the DZD CDS. All the accessibility-related metadata indicators scored 4 at the final FAIRness assessment, except RDA-A1-01M which was not applicable in this case.
Interoperability
Former DZD CDS Interoperability
The parameters contained in the DZD CDS have been harmonized across all DZD study centres to define a consistent data set within the DZD clinical studies. In a year-long process all modules and items were adjusted in numerous meetings with speakers, study centers, the Clinical Study Board and the experts for laboratory analyses and health economy. The DZD CDS had references to other related publications43,44. However, it was not linked to any other (meta)data that is online resolvable as required according to the FAIR principles. There were also no PIDs as required to link the data set to online available (meta)data. It did not contain any ontologies, controlled vocabularies or thesauri to describe the structure of (meta)data. The qualified references in the DZD CDS were insufficient and the DZD CDS was made available on the website as an MS Excel file. The minimal metadata was neither online resolvable nor linked to any other online resolvable (meta)data. Based on this, both the RDA-I3-01M and RDA-I3-02M indicators scored 3 at the FAIR baseline assessment. All the other interoperability-related metadata indicators scored 1.
Recommendations based on former state
It is critical that the machines have knowledge of other system’s data exchange formats42,45. This can be facilitated by the implementation of a comprehensive data model that contains ontologies, controlled vocabularies and thesauri to describe the structure and meaning of (meta)data for purposes of semantic enrichment and later retrieval28,41. Adding contextual knowledge via qualified references to the data set will facilitate interoperability41,46. Qualified references provide descriptions about relationships and associations between (meta)data in a meaningful way46. If other data sets are needed to complete the data, or if complementary information is stored in a different data set, these references need to be included in the original data set41. Technical formats that give a higher certainty of the machine data readability to spreadsheets are recommended for purposes of reusability and interoperability31,47. Proprietary data formats should be avoided to ensure long-term access to the data, independent of a specific software tool31.
Improvements Implemented
Publishing the DZD CDS at the metadata registry MDM portal allows downloading and exporting the file in most common technical formats such as ODM, PDF, CDA, CSV, FHIR, SQL, SPSS, ADL, R and XLSX. The Clinical Data Interchange Standards Consortium Operational Data Model is the preferred format for download in the MDM portal48,49. Some other formats are still under revision. If the CSV format is chosen, the download is split in four categories: One containing the Study OID, the title and description. Two forms (starting with “F1” resp “F2”) containing the Base Set and the Optional Set. The fourth contains the code lists and refers to the forms via the shared identifier in column “OID”. For purposes of standardizing the vocabulary, all the concepts in the CDS were successfully annotated with codes from the UMLS that were provided by the MDM portal50. In addition, all parameters in the modules “Vital Signs” and “Laboratory” were annotated with LOINC codes51. All parameters from the modules “Master Data”, “Anthropometry”, “Diabetes”, “Medical History”, and “Medical History - Comorbidities” have received an additional annotation with codes according to SNOMED-CT51,52. The CDS on the MDM portal has been linked to the complete metadata and SOP which is registered in a searchable resource and is online resolvable21.
These efforts resulted in all the interoperability-related metadata indicators scoring 4 at the final FAIRness assessment. To further enhance the interoperability, references to other related data sets such as the CDS of the Medical Informatics Initiative in Germany may be added22,53.
Reusability
Former DZD CDS Reusability
As already mentioned, the former version of the DZD CDS lacked in metadata and provenance. Furthermore, it had not been released with a license that stipulates reuse and there was neither information about the linkage of the DZD CDS items nor how they have changed over time. If there were to be future versions of the DZD CDS, users would have to read through the different versions and search for matching data items manually and this is difficult to automate. Domain specific standards which also facilitate reuse were yet to be implemented in this data set. It did however have citations for reused data and publications that informed this data set. For example “Laposata’s Laboratory Medicine: Diagnosis of Disease in the Clinical Laboratory, 2e” or “Diabetes mellitus: Neuer Referenzstandard für HbA1c, Dtsch Arztebl 2009; 106(17): A-805 / B-686 / C-670, Reinauer, Hans; Scherbaum, Werner A.” but the citations were incomplete. Based on this, only the RDA-R1-01M indicator scored 2 while all the other reusability-related metadata indicators scored 1 at the FAIR baseline assessment.
Recommendations based on former state
It is easier to reuse data if there is rich metadata attached to the data in a manner that allows to decipher the origin, lineage, usefulness, relevance and how to cite the data in the said context. Therefore, generosity when providing metadata and provenance is highly encouraged. To avoid improper data reuse, explicitness in the elaborations that indicate the conditions under which both humans and machines can reuse the data is also encouraged. It is more likely that other researchers reuse data if the metadata contains domain-specific standards, i.e. (meta)data has the same type, is standardized, follows a community accepted template, contains the same type of data organized in a standardized way, well-established and sustainable file formats and uses a common vocabulary. For example, the Rili-BAEK part A 6.3.2 and ISO 15189 5.8 specify general requirements and a minimum set of information that must be included in a clinical chemistry laboratory report in Germany54.
Improvements Implemented
Rich metadata including standardized vocabularies was attached to the dataset and made publicly available. The Creative Commons BY-NC-SA 4.0 licence was chosen for this data set, metadata and SOP42. This follows the regulations of open definition by the Open Knowledge Foundation55,56. Therefore, the material is free to share and adapt for non-commercial use as long as appropriate credit is given and the contributions are distributed under the same licence as the original. Users can also reuse parts of the DZD CDS according to their research needs. The MDM portal has features that show similar datasets for comparability purposes. Users of the MDM portal can comment on the data model which allows user feedback.
As shown in the descriptions of the data elements in the laboratory and diabetes modules, the metadata is in accordance with community accepted standards and recommendations57,58. The provenance included for the CDS indicates:
-
Origin of data, citations for reused data:
Where available the citations for reused data were extended, it is found under “Description” at the MDM entry. i.e. for the “Baecke Index leisure index” : ; German version by Wagner P, Singer R: “Ein Fragebogen zur Erfassung der habituellen körperlichen Aktivität verschiedener Bevölkerungsgruppen. Sportwissenschaft” (2003) 33:383-39743.
-
The workflow description for collecting data:
The detailed standard operating procedure has been published in Zenodo in PDF21. Some of this information is also part of the description in the MDM portal, i.e. for “Type of diabetes”: “According to the practice recommendations of the German Diabetes Association: Definition, classification and diagnosis of diabetes mellitus (Update 11/2020). If “type 3”, please specify subtype in the following question.” or for “Waist Circumference”: “Measured in the middle of the highest point of the iliac crest and the last rib, accurate to the nearest 0.5 cm; see DZD-SOP-DM-002 _Core _data_Set _V1.0”.
-
The processing history of data and the version history of data:
The first version (1.1.0) was published in 2021 as an excel sheet on the DZD website. The revised version was first uploaded to the MDM portal in November 2022 and has since been continuously adapted and further versioned (latest release in February 2024).
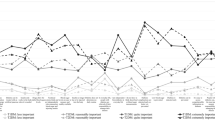
These implementations increased the reusability of the DZD CDS. All the reusability-related metadata indicators scored 4 at the final FAIRness assessment. The following Figs. 4 and 5 show the results of the baseline and final FAIR assessment using the RDA FDMM.

Baseline DZD CDS FAIR assessment results.

Final DZD CDS FAIR assessment results.
Discussion
As one step towards comprehensive data stewardship, the DZD data management group prioritised the FAIRification process of the CDS so as to foster its utilisation within the DZD and the wider diabetes research community. This work describes the FAIRification process applied to the DZD CDS. We argue that the enhancement of a CDS enables clinicians to generate and share “better” (FAIR) research data based on the information encoded in the CDS. Specifically, computer-readable data can be shared and exchanged across studies and study sites. The FAIR DZD CDS has been made available to the community in the MDM portal as already shown in Figs. 2 and 3.
In FAIRifying the DZD CDS, it was necessary to experiment with a number of FAIR assessment tools before deciding on which one was the most suitable with regards to the goals, priorities and resources available for the first FAIRification iteration. The decision to use the RDA-FDMM was arrived at after 3 tools were tried, tested and eliminated for various reasons. The SATIFYD was eliminated because although it was extremely easy to use, the experts were not satisfied with the tool’s interpretation of the FAIR data principles31. It has since been archived by the developers. The Australian Research Data Commons FAIR Data Self Assessment Tool was eliminated because it did not indicate which FAIR sub-principles are covered by each of the available questions and it does not allow for a separate assessment of data and metadata as was required in this context59,60,61. Although the FAIR Data Self-Assessment-Service for the Human Exposome Assessment Platform was aligned to the goals, priorities and resources available for the first FAIRification iteration, it was eliminated because it provided a similar means of assessment as the RDA-FDMM tool34. This process of testing and eliminating FAIR assessment tools was among the time-consuming factors in this work. The RDA-FDMM proved useful in enabling FAIR research data management by explicitly defining the requirements that should be fulfilled to support data FAIRness. The RDA-FDMM also provided for the compliance with these requirements to be evaluated and gaps in compliance to be identified. This further informed our multidisciplinary team that drafted the road map that led to a FAIRer DZD CDS. As the FAIR data principles gain traction, various FAIR assessment tools and frameworks with different focuses and FAIR assessment criteria continue to be developed62. These frameworks and tools often show inconsistent and even incomparable results63,64. Establishing the criteria that guides the choice of a FAIR assessment tool may prove to be a worthy cause.
The heterogeneity of non-interoperable research data infrastructure in a fragmented landscape makes it challenging to meaningfully exchange data12. According to the FAIR data principles, a key part of data interoperability is based on the availability of the data in machine readable formats, the linkage of this data to related (meta)data and the provision of contextual metadata about the data25. Semantic annotations as well as mappings to standards and terminologies play a critical role in achieving data interoperability and reusability44,65. Prior to our FAIRification efforts, the DZD CDS lacked structured and machine-readable encoding, hindering its potential for broad usability. The data curators thoroughly structured and harmonized the data and mapped the local codes to standardized terminologies in order to provide understandable, valuable and fit-for-purpose data for researchers. The mapping task was not trivial and required domain knowledge as well as thorough understanding of the used standard terminology terms to make sure that the semantic meaning is correctly translated from the local codes to the applied standards. The UMLS was implemented as a formal, accessible, shared code to describe the standardized variables in a machine-readable format. In addition, LOINC codes were provided for all parameters in the laboratory module and SNOMED codes for all others. This is beneficial in a number of ways:
-
It contributes to findability by facilitating data intelligibility66.
-
It allows for data linkage so that the data is openly accessible and shareable semantically which further facilitates reuse67.
-
It facilitates the data user to identify content in a structured way which facilitates semantic search functionality so that relevant data can be found with a single search query68.
-
It contributes to the establishment of a well-defined framework to harmoniously describe and structure the DZD CDS which contributes to the increased FAIRness of both the DZD CDS and the related data69.
-
It lays the groundwork required for data exchange among heterogeneous machines and enables the assessment of the comparability across studies related to the DZD CDS70.
-
It lays the groundwork required for compatible studies related to the DZD CDS to be combinable in a (semi)automatic way69,71.
The ability of the MDM portal to export data in technical formats facilitates the interoperability of the DZD CDS. The implementation of these formats enables data to be loaded directly into heterogeneous software for data analysis, integration and transformation to other formats for purposes of interoperability. The addition of contextual knowledge (PIDs, reference to other data sets/publications) in the form of meaningful links to relevant resources has further enhanced machine-actionability and processing. It may be necessary to provide more details and guidelines such as the specification of conventions for the definition of URIs of common resources to facilitate data interoperability between different data sets that would be relevant for the DZD CDS to be interoperable with. Data validation remains a critical step to ensure that the data generated is usable by researchers and to validate that only valid codes are used to encode the data72,73. For purposes of transparent data governance, the data providers developed comprehensive provenance and a README file that detail how the data elements are represented. In all DZD multicentred clinical trials, the direct identifying data (IDAT) are handled spatially and organisationally separated from the medical data (MDAT) to comply with legal, organisational and technical requirements regarding data protection74. For this reason the IDAT is not part of the CDS. Record linkage is handled via a pseudonymization service offered by a trusted agency75. This influenced our decision to choose an open machine-readable licence76. A relevant community standard for diabetes metadata is yet to be implemented in the DZD CDS. Our addition of a plurality of accurate and relevant attributes to the DZD CDS has also increased the reusability of this dataset. Implementing the FAIR principles through independent registry portals like the MDM portal offers both advantages and limitations. These portals are key in making datasets findable and accessible by indexing them with standardized metadata and offering searchable databases, which aids in data standardization and sharing77. They enable clinical researchers to merge datasets from various studies, thereby expanding research scope. However, challenges such as gaps in data coverage, inconsistent data quality, sustainability issues, and limited integration with broader data ecosystems diminish their standalone effectiveness77,78. This underscores the necessity for integrating registry portals within a more comprehensive data management strategy to enhance their utility in research.
FAIRification has shown to be a worthy investment towards improving the data quality and a FAIR data set positively affects research outcomes62. While the FAIR principles are generally known, only a few scientists can explain their meaning or interpretation in detail79. Studies show that scientists tend to overestimate the FAIRness of their data62,64. Thus, it is imperative to raise awareness among scientists on what it actually means to strive for a “FAIRness” and to support them in the FAIRification process62,79.
FAIR data is a journey; not a destination. This work presents our initial FAIRification efforts of the DZD CDS. Yielding consensus on the various matters that tend to arise during the retrospective FAIRification as well as implementing the decisions agreed upon will require a significant investment of resources. We still have a few questions to ponder on as a result of embarking on this journey; What is the frequency of updates required to maintain a FAIR DZD CDS? Is it necessary for all the pertinent stakeholders (data owners, domain experts, FAIR data stewards) to continuously participate in the subsequent FAIRification iterations? Is it a realistic expectation to iteratively provide the resources required for FAIRification cycles? Is it more practical to incrementally set a minimum FAIR score per FAIRification iteration than to aim for the ever elusive 100%?
Impact of this Work
In this work, we have documented the comprehensive FAIRification journey of the DZD CDS. This work required a deep understanding of the processes by which the CDS had been defined, adapted, and expanded. Conducting this work led us to resonate with the sentiments expressed in previous studies that successful data FAIRification requires collaborative efforts between data stewards, data owners and domain experts10,80. The fruit of our collaborative efforts is improved FAIRness of the DZD CDS. We postulate that this result will contribute to enhanced data sharing in diabetes research.
Our FAIRification journey this far has led us to annotate all the concepts in the DZD CDS with UMLS codes which studies show to be a critical step in the implementation of an ontology matching service for querying FAIR data81. During the annotation process we established a well-defined framework to describe and structure the DZD CDS in order to facilitate findability and interoperability. We furthermore registered the DZD CDS and the related metadata in the MDM portal and on Zenodo to enable version control and access to current and future versions of the CDS. The MDM portal now houses the DZD CDS in a machine readable format that uses an established and accessible language37,38. We expect to see an increase in the reuse of this data set as a result and the fact that we put an open licence on this data set. A key return on investment in the resources employed for this FAIRification journey is the increased certainty of the future data readability. The real world benefit of the applied FAIRification and its limitations remain areas of future research. It would particularly be interesting to see the impact this work has on patient data that has been produced using a FAIRified CDS. We only considered the FDMM metadata indicators in the FAIR assessment of the DZD CDS. This adaptation was necessary to fit the assessment to the context of a CDS. Future work should explore if the methods described in this work are reproducible in a different context.
FAIRification has been described as a gradually incremental process82. Our journey so far has helped to increase our understanding of the FAIR concept and informed our decision to employ formal workflows developed for FAIRification for our next FAIRification iteration80,83. In aligning more formal workflows to the nature of the DZD CDS and related data sets, it may be necessary to skip the step of data de-identification and pseudonymization because this data set does not contain any information which would comprise the data subjects’ rights regarding privacy issues. Conducting this work led us to resonate with studies that describe the process of retrospectively mapping raw data to the format required for purposes of data transformation and machine-readability as a clerical burden that requires a substantial investment of time and effort84,85,86,87. It is for this reason that we encourage scientists and data owners to design their scientific projects in a manner that puts into consideration prospective data FAIRification right from the infancy stage. In our case, this largely consists of data standardization and harmonization at the source for purposes of semantic modelling. It has also been recommended that regular FAIR assessments and continuous improvements in FAIR scores should be performed throughout data management32.
We hope that this work serves to inform the development of other future FAIR evaluators. It is also anticipated that our FAIRification of the DZD CDS will contribute to its increased uptake among relevant stakeholders both within the DZD the wider diabetes research community and act as a blue print for FAIR core data sets on an international scale.
Data availability
An archived record of the former version of the DZD CDS before FAIRification is retrievable in Zenodo at: https://doi.org/10.5281/zenodo.1252669020. The FAIRified version of the DZD CDS has been deposited into the MDM portal and it is retrievable at: https://medical-data-models.org/45923?lang=en38.
The related metadata and SOPs have been deposited into Zenodo and is retrievable at: https://zenodo.org/record/736000021.
Code availability
No code was used in this work.
References
Deutsches Zentrum für Diabetesforschung. DZD website. https://www.dzd-ev.de/en/research/multicenter-studies/index.html. Accessed: 2024-04-16.
Olschki, L. S.Summary of past and future activities of the German Center for Lung Research (DZL), 179–189 (Fondazione Internazionale Premio Balzan, 2021).
Hoffmann, J. et al. The DZHK research platform: maximisation of scientific value by enabling access to health data and biological samples collected in cardiovascular clinical studies. Clinical Research in Cardiology 112, 923–941, https://doi.org/10.1007/s00392-023-02177-5 (2023).
Falkai, P. et al. Concept of the Munich/Augsburg consortium precision in mental health for the German center of mental health. Frontiers in Psychiatry 13: 815718, https://doi.org/10.3389/fpsyt.2022.815718 (2022).
Joos, S. et al. German Cancer Consortium (DKTK)–a national consortium for translational cancer research. Molecular Oncology 13, 535–542, https://doi.org/10.1002/1878-0261.12430 (2019).
Luciano, M. et al. Editorial: Mortality of People with Severe Mental Illness: Causes and Ways of its Reduction. Frontiers in Psychiatry 13:1009772, https://doi.org/10.3389/fpsyt.2022.1009772 (2022).
Deutschen Zentren der Gesundheitsforschung. DZG website. https://deutschezentren.de (Accessed: 2024-09-16).
Lin, S., Morrison, L. J. & Brooks, S. C. Development of a data dictionary for the strategies for post arrest resuscitation care (SPARC) network for post cardiac arrest research. Resuscitation 82, 419–422, https://doi.org/10.1016/j.resuscitation.2010.12.006 (2011).
Durinx, C. et al. Identifying ELIXIR core data resources. F1000Research 5, https://doi.org/10.12688/f1000research.9656.2 (2016).
Queralt-Rosinach, N. et al. Applying the FAIR principles to data in a hospital: challenges and opportunities in a pandemic. Journal of Biomedical Semantics 13, 12, https://doi.org/10.1186/s13326-022-00263-7 (2022).
Hoffmann, K. et al. Data integration between clinical research and patient care: A framework for context-depending data sharing and in silico predictions. PLOS Digital Health 2, e0000140, https://doi.org/10.1371/journal.pdig.0000140 (2023).
Torab-Miandoab, A., Samad-Soltani, T., Jodati, A. & Rezaei-Hachesu, P. Interoperability of heterogeneous health information systems: a systematic literature review. BMC Medical Informatics and Decision Making 23, 18, https://doi.org/10.1186/s12911-023-02115-5 (2023).
Rashid, S. M. et al. The semantic data dictionary-an approach for describing and annotating data. Data Intelligence 2, 443–486, https://doi.org/10.1162/dint_a_00058 (2020).
Buchanan, E. M. et al. Getting started creating data dictionaries: How to create a shareable data set. Advances in Methods and Practices in Psychological Science 4, https://doi.org/10.1177/2515245920928007 (2021).
Wilson, P. S. What mapping and modeling means to the HIM professional. Perspectives in health information management 4, 2 (2007).
Sass, J. et al. The German Corona Consensus (GECCO) dataset : a standardized dataset for COVID-19 research in university medicine and beyond. BMC Medical Informatics and Decision Making 20, 1–7, https://doi.org/10.1186/s12911-020-01374-w (2020).
Devivo, M. et al. International spinal cord injury core data set. Spinal Cord 44, 535–540, https://doi.org/10.1038/s41393-022-00862-2 (2006).
Draeger, C. et al. Identifying relevant FHIR elements for data quality assessment in the german core data set. In Caring is Sharing–Exploiting the Value in Data for Health and Innovation, 272–276, https://doi.org/10.3233/SHTI230117 (IOS Press, 2023).
Darms, J. et al. Improving the FAIRness of health studies in Germany: The German central health study hub COVID-19. In Caring is Sharing - Exploiting the Value in Data for Health and Innovation, 78–82, https://doi.org/10.3233/SHTI210818 (IOS Press, 2021).
German Center for Diabetes Research. Withdrawn: DZD CORE DATA SET - first version published at DZD website for internal use (obsoleted by doi 10.21961/mdm:45923), https://doi.org/10.5281/zenodo.12526690 (2024).
German Center for Diabetes Research (DZD). DZD CORE DATA SET – metadata and SOP, https://doi.org/10.5281/zenodo.7360000 (2022).
University Hospital Tuebingen. IFIS website. https://clinicaltrials.gov/ct2/show/NCT04607096. Accessed: 2024-04-16.
Jumpertz von Schwartzenberg, R. et al. SGLT2 inhibition in addition to lifestyle intervention and risk for complications in subtypes of patients with prediabetes-a randomized, placebo controlled, multi-center trial (lifetime)-rationale, methodology and design. medRxiv 2023–11, https://doi.org/10.1101/2023.11.18.23298622 (2023).
DZG. DZG CORE DATA SET. https://medical-data-models.org/45851#model-model (2023). Accessed: 2024-07-04.
Wilkinson, M. D. et al. The FAIR guiding principles for scientific data management and stewardship. Scientific data 3, 1–9, https://doi.org/10.1038/sdata.2016.18 (2016).
Pasquetto, I., Borgman, L., & Wofford, F. Uses and reuses of scientific data: the data creators' advantage. Harvard Data Science Review, 1 (2), https://doi.org/10.1162/99608f92.fc14bf2d (2019).
Berman, F., Wilkinson, R. & Wood, J. Building global infrastructure for data sharing and exchange through the research data alliance. D-Lib Magazine 20, 1 – 4, https://doi.org/10.1045/january2014-berman (2014).
RDA FAIR Data Maturity Model Working Group. FAIR data maturity model: specification and guidelines. Res. Data Alliance 10, https://doi.org/10.15497/rda00050 (2020).
Bahim, C., Dekkers, M. & Wyns, B. Results of an analysis of existing FAIR assessment tools. Data Science Journal, https://doi.org/10.5334/dsj-2024-033 (2019).
Bahim, C. et al. The FAIR data maturity model: An approach to harmonise FAIR assessments. Data Science Journal, https://doi.org/10.5334/dsj-2020-041 (2020).
Krans, N. et al. FAIR assessment tools: evaluating use and performance. NanoImpact 100402, https://doi.org/10.1016/j.impact.2022.100402 (2022).
Bach, J. S. et al. FAIR assessment practices: Experiences from KonsortSWD and BERD@NFDI. In Proceedings of the Conference on Research Data Infrastructure, vol. 1, https://doi.org/10.52825/CoRDI.v1i.344 (2023).
Balaur, I. et al. FAIR assessment of MINERVA as an opportunity to foster open science and scientific crowdsourcing in systems biomedicine. bioRxiv, https://doi.org/10.1101/2024.08.28.610042 (2024).
Müller, H. et al. BIBBOX, a FAIR toolbox and app store for life science research. New Biotechnology, https://doi.org/10.1016/j.nbt.2023.06.001 (2023).
Hilse, H.-W. & Kothe, J. Implementing persistent identifiers (Consortium of European Research Libraries, 2006).
Simser, C. N. & Somers, M. A. Experimentation and Collaboration: Creating Serials for a New Millennium: Proceedings of the North American Serials Interest Group, Inc. 12th Annual Conference, May 29-June 1, 1997, University of Michigan, Ann Arbor, Michigan, vol. 1 (Psychology Press, 1998).
Dugas, M. et al. Portal of medical data models: information infrastructure for medical research and healthcare: Database. The Journal of Biological Databases and Curation, https://doi.org/10.1093/database/bav121 (2016).
Deutsches Zentrum für Diabetesforschung. DZD CORE DATA SET. https://doi.org/10.21961/mdm:45923 (2021).
Weber, T., Kranzlmüller, D., Fromm, M. & de Sousa, N. T. Using supervised learning to classify metadata of research data by field of study. Quantitative Science Studies 1, 525–550, https://doi.org/10.1162/qss_a_00049 (2020).
Humphreys, B. L., Del Fiol, G. & Xu, H. The UMLS knowledge sources at 30: indispensable to current research and applications in biomedical informatics. Journal of the American Medical Informatics Association 27, 1499–1501, https://doi.org/10.1093/jamia/ocaa208 (2020).
Rocca-Serra, P. et al. D2.1 The FAIR cookbook, https://doi.org/10.5281/zenodo.6783564 (2022).
Data4Ag project of CTA with PAFO and FAO. Farm data management, sharing and services for agriculture development online course, https://doi.org/10.5281/zenodo.3663553 (2020).
Baecke, J. A., Burema, J. & Frijters, J. E. A short questionnaire for the measurement of habitual physical activity in epidemiological studies. Am J Clin Nutr 36, 936–942, https://doi.org/10.1093/ajcn/36.5.936 (1982).
Laleci, G. B., Yuksel, M. & Dogac, A. Providing semantic interoperability between clinical care and clinical research domains. Journal of Biomedical and Health Informatics 17, 356–369, https://doi.org/10.1109/TITB.2012.2219552 (2013).
Nilsson, J., Sandin, F. & Delsing, J. Interoperability and machine-to-machine translation model with mappings to machine learning tasks. In 2019 IEEE 17th International Conference on Industrial Informatics (INDIN), vol. 1, 284–289, https://doi.org/10.1109/INDIN41052.2019.8972085 (2019).
Muzoora, M. R. et al. Towards FAIR patient reported outcome: Application of the interoperability principle for mobile pandemic apps. In Applying the FAIR Principles to Accelerate Health Research in Europe in the Post COVID-19 Era, 85–86, https://doi.org/10.3233/SHTI210820 (2021).
Rocca-Serra, P. et al. The FAIR cookbook-the essential resource for and by FAIR doers. Scientific data 10, 292, https://doi.org/10.1038/s41597-023-02166-3 (2023).
Huser, V., Sastry, C., Breymaier, M., Idriss, A. & Cimino, J. J. Standardizing data exchange for clinical research protocols and case report forms: An assessment of the suitability of the clinical data interchange standards consortium (cdisc) operational data model (odm). Journal of Biomedical Informatics 57, 88–99, https://doi.org/10.1016/j.jbi.2015.06.023 (2015).
Clinical Data Interchange Standards Consortium. CDISC Website. https://www.cdisc.org/standards/data-exchange/odm (2024). Accessed: 2024-07-04.
Bodenreider, O. The unified medical language system (UMLS): integrating biomedical terminology. Nucleic Acids Research 32, D267–D270, https://doi.org/10.1093/nar/gkh061 (2004).
Bodenreider, O., Cornet, R. & Vreeman, D. J. Recent developments in clinical terminologies—SNOMED CT, LOINC, and RxNorm. Yearbook of Medical Informatics 27, 129–139, https://doi.org/10.1055/s-0038-1667077 (2018).
Lee, D., de Keizer, N., Lau, F. & Cornet, R. Literature review of SNOMED CT use. Journal of the American Medical Informatics Association 21, e11–e19, https://doi.org/10.1136/amiajnl-2013-001636 (2014).
Ulrich, H. et al. Hands on the medical informatics initiative core data set—lessons learned from converting the MIMIC-IV. In German Medical Data Sciences 2021: Digital Medicine: Recognize–Understand–Heal, 119–126, https://doi.org/10.3233/SHTI210549 (2021).
Bietenbeck, A. et al. Requirements for electronic laboratory reports according to the German guideline Rili-BAEK and ISO 15189. Journal of Laboratory Medicine 45, 197–203, https://doi.org/10.1515/labmed-2020-0130 (2021).
Perens, B. et al. The open source definition. Open sources: Voices from the Open Source Revolution 1, 171–188 (1999).
Open Knowledge Foundation. Open definition 2.1. https://opendefinition.org/od/2.1/en/. Accessed: 2024-04-16.
Laposata, M. Laboratory Medicine Diagnosis of Disease in Clinical Laboratory 2/E (McGraw-Hill Education, 2014).
Fonseca, V. A., Kirkman, M. S., Darsow, T. & Ratner, R. E. The American diabetes association diabetes research perspective. Diabetes Care 35, 1380–1387, https://doi.org/10.2337/dc12-9001 (2012).
Ziaabadi, M. FAIR and open energy data for the wind energy sector. Master’s thesis, Høgskulen på Vestlandet (2021).
Schwanitz, V. J. et al. Towards FAIR data for low carbon energy-current state and call for action. Research Square, https://doi.org/10.1038/s41598-022-08774-0 (2021).
Australian Research Data Commons. FAIR data self assessment tool. https://ardc.edu.au/resource/fair-data-self-assessment-tool/ Accessed: 2024-04-16. (2022).
Inau, E. T., Sack, J., Waltemath, D. & Zeleke, A. A. Initiatives, concepts, and implementation practices of the findable, accessible, interoperable, and reusable data principles in health data stewardship: Scoping review. J Med Internet Res 25, e45013, https://doi.org/10.2196/45013 (2023).
Candela, L., Mangione, D. & Pavone, G. The FAIR assessment conundrum: Reflections on tools and metrics. Data Science Journal https://doi.org/10.5334/dsj-2024-033 (2024).
Wilkinson, M. D. et al. FAIR assessment tools: towards an “apples to apples” comparisons, https://doi.org/10.5281/zenodo.7463421 (2022).
Liao, Y., Lezoche, M., Panetto, H. & Boudjlida, N. Why, where and how to use semantic annotation for systems interoperability. 1st UNITE Doctoral Symposium, 71–78 (2011).
Hedden, H. Taxonomies and controlled vocabularies best practices for metadata. Journal of Digital Asset Management 6, 279–284, https://doi.org/10.1057/dam.2010.29 (2010).
Wittig, U., Rey, M., Weidemann, A. & Müller, W. Data management and data enrichment for systems biology projects. Journal of Biotechnology 261, 229–237, https://doi.org/10.1016/j.jbiotec.2017.06.007 (2017).
Awaysheh, A. et al. A review of medical terminology standards and structured reporting. Journal of Veterinary Diagnostic Investigation 30, 17–25, https://doi.org/10.1177/1040638717738276 (2018).
Navathe, S. B. & Kerschberg, L. Role of data dictionaries in information resource management. Information & Management 10, 21–46, https://doi.org/10.1016/0378-7206(86)90058-3 (1986).
Zhu, Q. et al. Harmonization and semantic annotation of data dictionaries from the pharmacogenomics research network: a case study. Journal of Biomedical Informatics 46, 286–293, https://doi.org/10.1016/j.jbi.2012.11.004 (2013).
Humphreys, B. L. & Lindberg, D. The UMLS project: making the conceptual connection between users and the information they need. Bulletin of the Medical Library Association 81, 170–177 (1993).
Jawaid, H., Latif, K., Mukhtar, H., Ahmad, F. & Raza, S. A. Healthcare data validation and conformance testing approach using rule-based reasoning. In Health Information Science, 241–246, https://doi.org/10.1007/978-3-319-19156-0_25 (Springer International Publishing, Cham, 2015).
Harman, L. B. & Cornelius, F. Ethical health informatics: Challenges and opportunities (3 edn., Jones & Bartlett Publishers, 2017).
Bahls, T. et al. Designing and piloting a generic research architecture and workflows to unlock German primary care data for secondary use. Journal of Translational Medicine 18, 1–10, https://doi.org/10.1186/s12967-020-02547-x (2020).
Hampf, C. et al. Federated trusted third party as an approach for privacy preserving record linkage in a large network of university medicines in pandemic research, https://doi.org/10.21203/rs.3.rs-1053445/v1 (2021).
Kreutzer, T. Open content: A practical guide to using Creative Commons licences (German Commission for UNESCO, 2014).
Qu, Y. Evaluating and Enhancing FAIR Compliance in Data Resource Portal Development. Master’s thesis, Purdue University, https://doi.org/10.25394/PGS.25686354.v1 (2024).
Maxwell, L. et al. FAIR, ethical, and coordinated data sharing for COVID-19 response: a scoping review and cross-sectional survey of COVID-19 data sharing platforms and registries. The Lancet Digital Health 5, e712–e736, https://doi.org/10.1016/S2589-7500(23)00129-2 (2023).
McLaughlin, J. E., Tropsha, A., Nicolazzo, J. A., Crescenzi, A. & Brouwer, K. L. Moving towards FAIR data practices in pharmacy education. American Journal of Pharmaceutical Education 86, 8670, https://doi.org/10.5688/ajpe8670 (2022).
Jacobsen, A. et al. A generic workflow for the data FAIRification process. Data Intelligence 2, 56–65, https://doi.org/10.1162/dint_a_00028 (2020).
van Damme, P. et al. Performance assessment of ontology matching systems for FAIR data. Journal of Biomedical Semantics 13, 1–17, https://doi.org/10.1186/s13326-022-00273-5 (2022).
David, R. et al. FAIRness literacy: the Achilles’ heel of applying FAIR principles. CODATA Data Science Journal 19, 1–11, https://doi.org/10.5334/dsj-2020-032 (2020).
Sinaci, A. A. et al. From raw data to FAIR data: the FAIRification workflow for health research. Methods of Information in Medicine 59, e21–e32, https://doi.org/10.1055/s-0040-1713684 (2020).
Inau, E. T., Radke, D., Westphal, S., Zeleke, A. & Waltemath, D. Comparing voluntary LOINC mappings for the SHIP-4 medical laboratory data dictionary before and after domain expert review. In 67. Jahrestagung der Deutschen Gesellschaft für Medizinische Informatik, Biometrie und Epidemiologie e. V. (GMDS), 13. Jahreskongress der Technologie- und Methodenplattform für die vernetzte medizinische Forschung e. V. (TMF), https://doi.org/10.3205/22gmds058 (2022).
Spadaro, G. et al. The cooperation databank: machine-readable science accelerates research synthesis. Perspectives on Psychological Science 17, 1472–1489, https://doi.org/10.1177/17456916211053319 (2022).
Rocca-Serra, P. & Sansone, S.-A. Experiment design driven FAIRification of omics data matrices, an exemplar. Scientific Data 6, 271, https://doi.org/10.1038/s41597-019-0286-0 (2019).
Kochev, N. et al. Your spreadsheets can be FAIR: A tool and FAIRification workflow for the enanomapper database. Nanomaterials 10, 1908, https://doi.org/10.3390/nano10101908 (2020).
Acknowledgements
This work was partially funded by the NFDI4Health - Nationale Forschungsdateninfrastruktur für personenbezogene Gesundheitsdaten (DFG-funded project 442326535) and the Deutsches Zentrum für Diabetesforschung (German Center for Diabetes Research).
Funding
Open Access funding enabled and organized by Projekt DEAL.
Author information
Authors and Affiliations
Contributions
E.T.I. and M.P. devised the project and its main conceptual ideas. E.T.I., A.D., I.A., B.F., M.P., R.S., and Y.Z. conceived the model and participated in the theoretical and technical discussions. A.A.Z., and D.W. supervised this work. E.T.I. wrote the initial draft with assistance from A.D. All the authors read, reviewed, and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Inau, E.T., Dedié, A., Anastasova, I. et al. The Journey to a FAIR CORE DATA SET for Diabetes Research in Germany. Sci Data 11, 1159 (2024). https://doi.org/10.1038/s41597-024-03882-0
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41597-024-03882-0
