
Abstract
This study compared the optical axial length (AL) obtained by composite and segmental methods using swept-source optical coherence tomography (SS-OCT) devices, and demonstrated its effects on the post-operative refractive errors (RE) one month after cataract surgery. Conventional AL measured with the composite method used the mean refractive index. The segmented-AL method used individual refractive indices for each ocular medium. The composite AL (24.52 ± 2.03 mm) was significantly longer (P < 0.001) than the segmented AL (24.49 ± 1.97 mm) among a total of 374 eyes of 374 patients. Bland–Altman analysis revealed a negative proportional bias for the differences between composite and segmented ALs. Although there was no significant difference in the RE obtained by the composite and segmental methods (0.42 ± 0.38 D vs 0.41 ± 0.36 D, respectively, P = 0.35), subgroup analysis of extremely long eyes implanted with a low power intraocular lens indicated that predicted RE was significantly smaller with the segmental method (0.45 ± 0.86 D) than that with the composite method (0.80 ± 0.86 D, P < 0.001). Segmented AL with SS-OCT is more accurate than composite AL in eyes with extremely long AL and can improve post-operative hyperopic shifts in such eyes.
Similar content being viewed by others

Introduction
The accurate calculation of intraocular lens (IOL) power is crucial for achieving desirable refractive outcomes after cataract surgery. Post-operative refractive errors are mainly dependent on the following four factors: corneal power, axial length (AL), post-operative IOL position, and IOL quality (i.e. the error from variability in IOL power). Earlier studies have shown that 17–36% of post-operative refractive errors arise from imprecise AL measurements1,2. Historically, ultrasound biometry has been the most commonly used technique for measuring AL, anterior chamber depth (ACD), and crystalline lens thickness3. The immersion technique is generally considered to be more accurate than the contact technique in ultrasound biometry. However, the development of partial coherence interferometry (PCI) has led to more advanced optical biometry systems, which are ten times more precise than ultrasound for measuring AL4. PCI-based systems are now widely used and recognised as the gold standard for measuring ocular biometric parameters4,5,6,7.
It should be noted that optical and acoustic ALs are not equivalent, because the retinal pigment epithelium (RPE) is the endpoint of the optical measurements, and the internal limiting membrane (ILM) is the endpoint of the ultrasonic measurements. Moreover, the segmental method for AL determination includes the individual sound velocity of each component and the composite method uses the average sound velocity for all the components. Both methods are available for measuring the AL using ultrasound. On the other hand, the composite method measures AL optically via the mean group refractive index for all the components. Recently, segmented ALs measured by an optical low-coherence reflectometry (OLCR) biometer with a peak wavelength of 820 nm were reported to be longer in short eyes and shorter in long eyes, compared to those obtained by composite ALs8,9. Although OLCR and PCI can measure the AL with greater precision than ultrasound and do not require any contact with the eye, the mis-segmentation of cornea or crystalline lens is difficult to detect, because OLCR and PCI provide axial and intraocular distances on an A-scan information without two-dimensional cross-sections of the images.
A second generation anterior segment swept-source optical coherence tomography (AS-OCT) was recently developed10,11,12. This novel, but commercially-available, AS-OCT system has an improved scan rate, depth capacity, and density assessment, allowing for sharper images of the anterior and posterior surfaces of the cornea, crystalline lens, and IOL. As a result, corneal thickness, ACD, aqueous depth (AQD: the distance between the corneal endothelium and the lens surface), and lens thickness can be automatically measured using AS-OCT with good repeatability and reproducibility10,11,12. Moreover, a newly introduced optical biometer that is also based on swept-source optical coherence tomography (SS-OCT) has been shown to generate repeatable and reproducible measurements13,14,15,16.
The current study compared optical ALs obtained with the conventional composite method and the segmental method using SS-OCT based devices and examined the differences in post-operative refractive errors following cataract surgery.
Results
A total of 374 eyes of 374 patients (251 women [67.1%]) were included in this study. Patients had a mean age of 76.1 ± 8.3 years (range: 40–96 years). All eyes had successful phacoemulsification with IOL implantation. AcrySof Toric and AN6MA IOLs were implanted in 358 and 16 eyes, respectively.
Table 1 summarises the ocular dimensions including the corneal thickness, ACD, AQD, lens thickness, and vitreous length measured with SS-OCT and AS-OCT. These values were significantly different when measured with the two instruments (P < 0.001). The intraclass correlation coefficient was 0.992 for the corneal thickness, 0.999 for AQD, and 0.998 for the lens thickness, indicating good agreement for these parameters.
The mean composite ALRPE was 24.81 ± 1.94 mm (range: 21.52 to 32.93 mm) and the mean segmented ALRPE was 24.79 ± 1.97 mm (range: 21.42 to 32.99 mm). These values were significantly different (P < 0.001), but there was a significant correlation between the two values (R = 1.00). The mean composite ALILM was 24.52 ± 2.03 mm (range: 21.09 to 33.01 mm) and the mean segmented ALILM was 24.49 ± 1.97 mm (range: 21.12 to 32.69 mm). These values were also significantly correlated (R = 1.00, P < 0.001). The mean difference between the composite and segmented ALILM was 0.038 ± 0.067 mm.
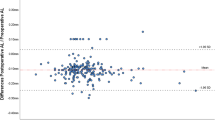
The Bland–Altman analysis revealed a negative proportional bias between the segmented and composite AL, indicating that the difference between segmented and composite ALILM measurements increased as AL increased (Fig. 1). The segmented ALILM was up to 0.32 mm shorter in an eye with a composite ALILM of 33.01 mm which is the longest eye in this study.

Bland–Altman plots showing the agreement between segmented and composite ALILM measurements. The solid line indicates the best-fit line (R2 = 0.89, P < 0.001). AL = axial length, ILM = inner limiting membrane.
The mean absolute refractive error (MAE) was 0.42 ± 0.38 D using the composite ALILM, and 0.41 ± 0.36 D using the segmented ALILM. There was no significant difference in the MAE (P = 0.35).
A subgroup analysis was performed for the 15 extra-long eyes implanted with low power IOLs (≤+4.00 D). The same model of IOL (AN6MA) were implanted in these 15 eyes. The mean composite ALILM was 31.02 ± 0.85 mm (range: 29.80 to 33.01 mm) and the mean segmented ALILM was 30.78 ± 0.82 mm (range: 29.61 to 32.69 mm, Table 2), which was significantly different (P < 0.001). The mean difference between composite and segmented ALILM measurements in extra-long eyes was 0.24 ± 0.03 mm.
The MAE using the segmented ALILM was 0.45 ± 0.86 D, which was significantly smaller than the MAE using the composite ALILM (0.80 ± 0.86 D, P < 0.001). Additionally, the percentage of correct refraction predictions within ±0.25 D, ±0.50 D, and ±1.00 D were 53.3%, 66.7%, and 86.7%, respectively, with segmented ALILM measurements and 33.3%, 53.3%, and 73.3%, respectively, with composite ALILM measurements (Table 2). There were significant differences in the percentage of refractive prediction errors between segmented and composite measurements within ±0.50 D (P = 0.003) and ±1.00 D (P = 0.01), but not ±0.25 D (P = 0.18).
Discussion
The AL can be calculated in a variety of ways, as shown in Fig. 2. These differences arose from changes in technology and measurement compatibility with IOL power calculation formulas. Since the segmental method with the ultrasound immersion technique is more accurate than the composite method with the ultrasound contact technique, we speculated that the optical measurements with the segmental method would be more precise than the conventional ones with the composite method. Therefore, the present study compared the composite and segmental methods of obtaining optical ALILM measurements. We found that the difference between the segmental and composite methods in optical ALILM measurements had a negative proportional bias with AL. This is because the regression Eq. (1) was used to adjust the composite ALRPE to the composite ALILM. As the ALRPE coefficient is 1.0446 (calculated by dividing 1.0 by 0.9573), ALILM was overestimated in the longer eye using Eq. (1). On the other hand, regarding vitreous length, which is often longer in the longer eye (see Supplementary Fig. S1), the calculated segmented AL is longer than the composite AL due to the difference between the reflective index of the vitreous (1.336), and the mean refractive index of the whole eye (1.349). However, this difference is smaller than the effect of the regression Eq. (1). Therefore, the ALILM was significantly shorter when acquired with the segmental method than with the composite method in highly myopic eyes. The IOL power calculation using the Haigis formula with segmented ALILM resulted in a smaller post-operative hyperopic shift than that using the composite ALILM in the subgroup analysis.

An overview of axial length (AL) measurement strategies for ultrasound and optical AL measurements. (A–D) Acoustic contact and immersion measurements made using mean group (composite; A,B) and individual tissue (segmental; C,D) sound velocity. Optical AL measurements using the composite (E,F) and segmental (G,H) methods. Optical systems (E,G) measure the linear distance between the corneal surface and the retinal pigment epithelium (RPE, ALRPE) and optical systems (F,H) measure the linear distance between the corneal surface and the inner limiting membrane (ILM, ALILM). Since intraocular lens power calculation formulas were developed using the ALILM, each segmented ALRPE measurement was converted to an ALILM by subtracting the retinal thickness (assumed to be 300 µm in all eyes). Optical composite ALRPE measurements were converted to ALILM measurements using a regression equation: ALILM = (ALRPE − 1.3304)/0.9573.
Many IOL power calculation formulas were developed before PCI-based optical biometers were invented. Therefore, one needs to rely upon the ultrasound ALILM4. The ultrasound ALILM with the immersion technique is shorter than the optical ALRPE with the composite method; this difference could induce post-operative refraction errors7. Therefore, an established conversion algorithm between optical ALRPE measurements with the composite method and immersion ultrasound ALILM measurements with the segmental method has been used for a long time7. This algorithm, however, is subject to limitations such as an inadequate retinal thickness measurement in eyes with longer ALs. For example, an eye with a 30.0 mm ALILM should have a retinal thickness of 49 μm (achieved composite ALRPE minus composite ALILM), but an eye with a 20.0 mm ALILM should have a retinal thickness of 476 µm (10-fold difference). This may be one of the reasons why ALs in long and short eyes tend to be less accurate for predicting refractive outcomes following cataract surgery. In previous studies, the segmented ALs measured by an optical biometer with an 820 nm wavelength were longer in short eyes and shorter in long eyes compared to the composite ALs8,9. In the current study, the relationship between segmented and composite ALILM obtained by SS-OCT with a wavelength of 1060 nm was similar to that reported previously8,9.
Although the most significant source of error that contributes to post-operative refractive error comes from the AL17, errors in predicted post-operative IOL positions have also become a major contributor to post-operative refractive errors after the introduction of laser biometry1,2,18. The post-operative IOL position no longer influences post-operative refractive errors when low power IOLs (<+4.0 D) are used; even a 1.0 mm forward movement in a low power IOL position (e.g., from 4.0 mm to 3.0 mm) influences the refractive outcome by less than −0.2 D, as demonstrated in Table 3. However, the high power IOL has a big influence on the refractive outcome. Therefore, we performed a subgroup analysis on patients that received an IOL with a power less than +4.0 D.
Previous studies have documented inaccuracies of the popular IOL formulas in long eyes19,20,21,22,23,24,25. Although the Haigis formula generally has better refractive outcomes in long eyes, post-operative hyperopic errors proportional to the AL have been reported23.
The current study did not find a significant difference between predicted post-operative refractive errors when the segmental method and composite method measurements of optical AL were examined in all eyes. However, the post-operative hyperopic shift with the Haigis formula was significantly improved in highly myopic eyes when the optical ALILM acquired with the segmental method was used. Although the simple replacement of the composite ALILM with the segmented ALILM in the traditional IOL power calculations would not help because many formulas are optimised for the composite ALILM, recent studies reported that the segmented AL measured via an optical biometer with a peak wavelength of 820 nm improved refractive prediction accuracy for vergence formulas8,9.
Our study had several limitations. First, it is a retrospective single centre study and the population in our subgroup study was relatively small. We used two different IOLs; further investigation of segmented AL measurements in a prospective multicentre study with a larger group of patients and with one model is desirable. Second, the fixation status during the measurement is an important factor for AL accuracy. The SS-OCT biometer enables us to obtain an optical B-scan image during AL measurement. Therefore, it is now possible to check the fixation status during AL measurements and to examine complete longitudinal cross-sectional images of the eye26,27,28,29. Further studies that utilise these SS-OCT capabilities are needed. Third, our study only measured the effect of AL characteristics on post-operative refractive outcomes. However, other factors are known to influence the refractive outcomes in cataract surgery. The corneal power, in particular, should be investigated more carefully because prior studies have shown that standard keratometry overestimates the corneal power24. Finally, the mean group refractive index can vary with cataract grade30, and adjustments may be needed for cataract types and stages in future studies.
In conclusion, the segmented ALILM is more accurate than the conventional one measured with the composite method when using SS-OCT, and the segmented AL measurement reduces the post-operative hyperopic shift in eyes with extra-long AL.
Methods
Study participants
This was a retrospective, consecutive case series of all patients who had undergone uncomplicated cataract surgery at a single centre, the National Hospital Organization, Tokyo Medical Center between October 2015 and January 2018. The protocol was reviewed and approved by the Institutional Review Board of the National Hospital Organization, Tokyo Medical Center, and was designed in accordance with the tenets of the Declaration of Helsinki. Informed consent was obtained from all patients. The selection criteria of this study followed the recommendations of a recent editorial by Hoffer et al.31 regarding best practices for studies of IOL formulas: the use of optical biometry and the inclusion of only 1 eye from each study subject. If patients underwent bilateral cataract surgery, then a randomly selected eye was chosen for inclusion in the study. The exclusion criteria were a best-corrected distance visual acuity after cataract surgery worse than 20/40, a history of ocular surgery, a history of ocular trauma, the presence of a significant ocular comorbidity, unreliable or undetectable preoperative biometry measurements, or a history of intra- or post-operative complications.
All patients underwent cataract surgery through a 2.2-mm corneal incision. One of the following IOLs was implanted: AcrySof Toric (SN6A T3-T6, Alcon, Fort Worth, TX) or AN6MA (KOWA, Nagoya, Japan). All surgical procedures were performed under topical anaesthesia by the same experienced surgeon (TN) and all IOLs were successfully inserted into the capsular bag after phacoemulsification.
Data collection and patient examinations
All data were retrospectively collected from patient medical records. All patients had undergone preoperative and 1-month post-operative ophthalmic examinations, including a slit-lamp examination, keratometry, and fundoscopy. SS-OCT based biometer (OA-2000; TOMEY CORPORATION, Nagoya, Japan) and AS-OCT (CASIA2; TOMEY CORPORATION) were performed preoperatively. Distant corrected visual acuity, refraction, and intraocular pressure were also measured only by experienced technicians.
Swept-source optical coherence tomography based biometer
The SS-OCT based biometer was used to measure AL and corneal power, along with corneal thickness, ACD, and lens thickness using the swept-source laser (1060 nm wavelength). The biometer obtained 10 consecutive scans and automatically calculated the average value.
Anterior segment optical coherence tomography
The angle analysis mode in CASIA2 was used to obtain anterior segment images comprising 16 consecutive meridional scans. This instrument uses a super-luminescent diode light source (1310 nm wavelength) and has a scan speed of 50,000 A-scans/second. All OCT images were obtained while the pupil was dilated (topical 0.5% tropicamide and 0.5% phenylephrine hydrochloride). All eyes were imaged in a dark room (illuminance of 0.3 lx) using internal fixation and were obtained twice by a trained technician who was masked to the clinical data.
Only images taken with a horizontal (180°) alignment were used in the analysis. Images were centred on the corneal vertex, which was defined as the cross point of the vertex normal and anterior corneal surface. The AS-OCT parameters measured along the vertex normal included corneal thickness, ACD, AQD, and lens thickness. Corneal thickness was defined as the distance between the anterior and posterior corneal surfaces, ACD is the distance between the anterior corneal and anterior lens surfaces, AQD is the distance between the posterior corneal and anterior lens surfaces, and lens thickness is the distance between the anterior and posterior lens surfaces (Fig. 3). The corneal thickness, AQD, and lens thickness were measured by two independent examiners (SG, II) who were masked to the clinical data.

An anterior segment optical coherence tomography (OCT) image showing optical biometer measurements. Measurements were made before cataract surgery along the vertex normal. The inset shows an external photograph with the location and direction of the OCT scan (green arrow). CT = corneal thickness, AQD = aqueous depth, LT = crystalline lens thickness, Lens-f = lens fornix, AR = angle recess, SS = scleral spur, N = nasal, S = superior, T = temporal, I = inferior.
Definition of axial length
Figure 2 illustrates how AL was obtained using acoustic and optical measurements. To measure AL, systems used either the composite method, which utilises the mean group index, or the segmental method, which accounts for individual tissue indices of the cornea, aqueous, lens, and vitreous. Ultrasound biometry can measure AL in the following four ways: acoustic contact measurements using mean group sound velocity (Fig. 2A), acoustic immersion measurements using mean group sound velocity (Fig. 2B), acoustic segmented contact measurements using individual sound velocities (Fig. 2C), and acoustic segmented immersion measurements using individual sound velocities (Fig. 2D). Segmented immersion is theoretically the most accurate acoustic measurement because the ultrasound probe does not directly contact the cornea (Fig. 2D).
On the other hand, the SS-OCT based optical biometer measures the optical path length of the whole eye. Currently, it is essential for the optical AL measurement to determine ALILM from the ALRPE, as popular IOL power formulas do not use ALRPE but use ALILM measurements instead. To estimate composite distance measurements between the cornea and RPE (ALRPE, Fig. 2E), the SS-OCT based biometer system uses a mean group refractive index of 1.3496. Then, the following equation (Eq. 1), which is publicly available through the manufacturer, was used to translate ALRPE into composite distance measurements between the cornea and ILM (ALILM, Fig. 2F) in the current study:
The segmented ALRPE is measured as the sum of the thickness of the cornea, aqueous, lens, and vitreous (Fig. 2G). The refractive indices of the cornea, aqueous, lens, and vitreous were set to 1.376, 1.336, 1.410, and 1.336, respectively26,32. Refractive indices of the individual tissue were used during the calculation. The corneal thickness, AQD, and lens thickness were directly measured using AS-OCT. The optical vitreous length was calculated by subtracting the optical path length of the corneal thickness, AQD, and the lens thickness obtained by AS-OCT from the optical path length of the whole eye obtained using an SS-OCT based biometer. Finally, the optical vitreous length was divided by the refractive index of vitreous (1.336) to obtain the vitreous length. The segmented ALILM (Fig. 2H) was then calculated by subtracting the retinal thickness (previously established as 300 μm33,34,35) from the segmented ALRPE.
Formula calculations
The Haigis formula7 was calculated using Excel spreadsheets (Microsoft Corporation, Redmond, WA, USA), and was checked against licensed commercial software on the SS-OCT based biometer. The optimised lens constants from the User Group for Laser Interference Biometry (ULIB) were used for calculations (AcrySof Toric: a0 = 1.78, a1 = 0.40, and a2 = 0.10 and AN6MA: a0 = 1.57, a1 = 0.40, and a2 = 0.10)36.
Data analysis
Composite and segmented ALILM measurements were compared by using the paired t-test. Bland–Altman plots were used to assess the agreement between the composite and segmented ALILM. The mean post-operative refractive errors (post-operative spherical equivalent minus the predicted post-operative spherical equivalent), mean absolute prediction error (MAE), median absolute prediction error, and standard deviation of the prediction error were calculated with the composite ALILM and the segmented ALILM. The Wilcoxon test was used to compare the MAE values. Subgroup analysis was performed on eyes in which low power IOL less than +4.0 D were implanted. The percentages of eyes with arithmetic prediction errors within ±0.25 D, ±0.50 D, and ±1.0 D were compared between the composite ALILM and the segmented ALILM using the McNemar test. Statistical significance was defined as P < 0.05. All statistical analyses were performed using JMP Pro statistical software (version 10.0.2, SAS Institute Inc., Cary, NC, USA).
Data availability
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
References
Norrby, S. Sources of error in intraocular lens power calculation. J. Cataract. Refract. Surg. 34, 368–376 (2008).
Olsen, T. Calculation of intraocular lens power: a review The statistical. Acta Ophthalmol Scand 2007:472–485.
Hoffer, K. J. Ultrasound velocities for axial eye length measurement. J. Cataract. Refract. Surg. 20, 554–562 (1994).
Drexler, W. et al. Partial coherence interferometry: a novel approach to biometry in cataract surgery. Am. J. Ophthalmol. 126, 524–34 (1998).
Roy, A., Das, S., Sahu, S. K. & Rath, S. Ultrasound Biometry vs. IOL Master. Ophthalmol. 119, 29–31 (2012).
Rajan, M. S., Keilhorn, I. & Bell, J. A. Partial coherence laser interferometry vs conventional ultrasound biometry in intraocular lens power calculations. Eye 16, 552–556 (2002).
Haigis, W., Lege, B., Miller, N. & Schneider, B. Comparison of immersion ultrasound biometry and partial coherence interferometry for intraocular lens calculation according to Haigis. Graefes Arch. Clin. Exp. Ophthalmol. 238, 765–773 (2000).
Cooke, D. L. & Cooke, T. L. A comparison of two methods to calculate axial length. J. Cataract. Refract. Surg. 45, 284–292 (2019).
Wang, L., Cao, D., Weikert, M. P. & Koch, D. D. Calculation of axial length using a single group refractive index versus using different refractive indices for each ocular segment: theoretical study and refractive outcomes. Ophthalmol. 126, 663–670 (2018).
Chansangpetch, S. et al. Agreement of Anterior Segment Parameters Obtained From Swept-Source Fourier-Domain and Time-Domain Anterior Segment Optical Coherence Tomography. Invest. Ophthalmol. Vis. Sci. 59, 1554–1561 (2018).
Kimura, S. et al. Assessment of tilt and decentration of crystalline lens and intraocular lens relative to the corneal topographic axis using anterior segment optical coherence tomography. PLoS One 12, 1–12 (2017).
Shoji, T. et al. In vivo crystalline lens measurements with novel swept-source optical coherent tomography: an investigation on variability of measurement. BMJ Open. Ophthalmol. 1, e000058 (2017).
Reitblat, O., Levy, A., Kleinmann, G. & Assia, E. I. Accuracy of intraocular lens power calculation using three optical biometry measurement devices: the OA-2000, Lenstar-LS900 and IOLMaster-500. Eye 32, 1244–1252 (2018).
McAlinden, C. et al. Axial length measurement failure rates with biometers using swept-source optical coherence tomography compared to partial-coherence interferometry and optical low-coherence interferometry. Am. J. Ophthalmol. 173, 64–69 (2017).
Savini, G. et al. Accuracy of a new swept-source optical coherence tomography biometer for IOL power calculation and comparison to IOLMaster. J. Refract. Surg. 33, 690–695 (2017).
Gao, R. et al. Comparison of ocular biometric measurements between a new swept-source optical coherence tomography and a common optical low coherence reflectometry. Sci. Rep. 7, 2484 (2017).
Olsen, T. Sources of error in intraocular lens power calculation. J. Cataract. Refract. Surg. 18, 125–129 (1992).
Goto, S. et al. Prediction of postoperative intraocular lens position with angle-to-angle depth using anterior segment optical coherence tomography. Ophthalmol. 123, 2474–2480 (2016).
Melles, R. B., Holladay, J. T. & Chang, W. J. Accuracy of Intraocular Lens Calculation Formulas. Ophthalmol. 125, 288–294 (2018).
Bang, S. et al. Accuracy of intraocular lens calculations using the IOLMaster in eyes with long axial length and a comparison of various formulas. Ophthalmol. 118, 503–506 (2011).
Wang, J. K., Hu, C. Y. & Chang, S. W. Intraocular lens power calculation using the IOLMaster and various formulas in eyes with long axial length. J. Cataract. Refract. Surg. 34, 262–267 (2008).
Abulafia, A. et al. Intraocular lens power calculation for eyes with an axial length greater than 26.0 mm: Comparison of formulas and methods. J. Cataract. Refract. Surg. 41, 548–556 (2015).
Wang, Q. et al. Accuracy of intraocular lens power calculation formulas in long eyes: A systematic review and meta-analysis. Clin Exp Ophthalmol (2018).
Olsen, T. Intraocular lens power calculation errors in long eyes. J. Cataract. Refract. Surg. 38, 733–734 (2012).
Yokoi, T. et al. Evaluation of refractive error after cataract surgery in highly myopic eyes. Int. Ophthalmol. 33, 343–348 (2013).
Shammas, H. J. et al. Biometry measurements using a new large-coherence-length swept-source optical coherence tomographer. J. Cataract. Refract. Surg. 42, 50–61 (2016).
Whang, W. J., Yoo, Y. S., Kang, M. J. & Joo, C. K. Predictive accuracy of partial coherence interferometry and swept-source optical coherence tomography for intraocular lens power calculation. Sci. Rep. 8, 1–10 (2018).
Omoto, M. K. et al. Ocular biometry and refractive outcomes using two swept-source optical coherence tomography- based biometers with segmental or equivalent refractive indices. Sci. Rep. 9, 6557 (2019).
Akman, A., Asena, L. & Güngör, S. G. Evaluation and comparison of the new swept source OCT-based IOLMaster 700 with the IOLMaster 500. Br. J. Ophthalmol. 100, 1201–1205 (2016).
Prinz, A. et al. Influence of severity of nuclear cataract on optical biometry. J. Cataract. Refract. Surg. 32, 1161–1165 (2006).
Hoffer, K. J. et al. Protocols for studies of intraocular lens formula accuracy. Am. J. Ophthalmol. 160, 403–405.e1 (2015).
Goncharov, A. V. & Dainty, C. Wide-field schematic eye models with gradient-index lens. J. Opt. Soc. Am. A Opt Image Sci. Vis. 24, 2157–2174 (2007).
Myers, C. E. et al. Retinal thickness measured by spectral-domain optical coherence tomography in eyes without retinal abnormalities: the Beaver Dam Eye Study. Am. J. Ophthalmol. 159, 445–456 (2015).
Duan, X. R. et al. Normal macular thickness measurements using optical coherence tomography in healthy eyes of adult Chinese persons: The Handan Eye Study. Ophthalmol. 117, 1585–1594 (2010).
Chan, A. et al. Normal macular thickness measurements in healthy eyes using Stratus optical coherence tomography. Arch. Ophthalmol. 124, 193–8 (2006).
User Group for Laser Interference Biometry (ULIB). Available at, http://ocusoft.de/ulib; (Oct 31, 2016. Accessed May 10, 2018).
Acknowledgements
The authors thank Keiko Ogawa, CO, Saori Sugiyama, CO, and Maki Matsumaru, CO, (Orthoptists of National Hospital Organization, Tokyo Medical Center) for their assistance with data collection.
Author information
Authors and Affiliations
Contributions
S.G., N.M., T.N. K.O., I.I., S.K. and K.N. designed the concept of this study. S.G., T.N. and I.I. collected the data. S.G., N.M. and T.N. conducted statistical analysis. S.G., N.M., T.N. and I.I. interpreted the data. S.G., N.M. and T.N. drafted the work. S.G., N.M., T.N. K.O., I.I., S.K. and K.N. revised it critically for important intellectual content. S.G., N.M., T.N. K.O., I.I., S.K. and K.N. approved of the version submitted for publication. All author agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Corresponding author
Ethics declarations
Competing interests
Drs. Goto, Maeda, Noda, and Nishida received fees from TOMEY CORPORATION for a sponsored seminar not related to this study. No conflicting relationship exists for any other author.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Goto, S., Maeda, N., Noda, T. et al. Comparison of composite and segmental methods for acquiring optical axial length with swept-source optical coherence tomography. Sci Rep 10, 4474 (2020). https://doi.org/10.1038/s41598-020-61391-7
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-020-61391-7
This article is cited by
-
Network architecture optimization for ophthalmic ultrasound image detection based on modular ablation of multi-version YOLO
BioMedical Engineering OnLine (2025)
