
Abstract
We examined the association between maternal air purifier use during pregnancy and neurodevelopmental delay in toddlers by analysing data from 82,457 mother-toddler pairs. Air purifier use was measured using a simple yes/no question. Developmental delays at 1.5, 2.0, 2.5, and 3.0 years were assessed using the Ages and Stages Questionnaire, Third Edition. Generalized additive mixed model analysis with 21 covariates revealed that air purifier use was associated with lower prevalence of developmental delay in all five areas—communication, gross motor, fine motor, problem solving, and personal-social—at all four time points (adjusted risk ratios ranged from 0.827 to 0.927, and only one 95% confidence interval crossed the reference). These findings suggest a negative association between air purifier use during pregnancy and neurodevelopmental delay in toddlers.
Trial registration: UMIN000030786 (15/01/2018).
Similar content being viewed by others


Introduction
Accumulating evidence suggests that foetal exposure to air pollution plays a role in the aetiology of neurodevelopmental delay1,2,3. For example, previous studies linked foetal exposure to particulate matter (PM) or polycyclic aromatic hydrocarbons to brain morphology and reduced cognitive function in school-aged children4 and decreased IQs at 5 years of age5. Although the detailed mechanisms underlying the relationship remain unknown, one possible pathway is via neuroinflammation6.
One potential countermeasure against an air pollution-related increase in children’s neurodevelopmental delay would involve the use of air purifiers during pregnancy. Previous studies found that air purifiers can drastically reduce indoor PM1–PM50 concentrations7,8 and weaken allergic symptoms by reducing airborne PM2.5 levels9,10. Accordingly, children’s neurodevelopmental delay should also be reduced in the offspring of mothers who use an air purifier during pregnancy.
We previously examined this aspect using cohort data from the Japan Environment and Children’s Study (JECS)11. Although we did not measure indoor PM concentrations ourselves, we revealed that air purifier use during pregnancy was associated with decreased prevalence of infant neurodevelopmental delay at 6 and 12 months of age, as assessed using the Ages and Stages Questionnaire, Third Edition (ASQ-3). However, given that the human brain undergoes dramatic development both structurally and functionally in early childhood12, it is necessary to examine whether this association persists at later ages.
Therefore, to expand on our recent findings11, we examined the same topic but focused on data obtained from children between 1.5 and 3 years of age. Fortunately, the JECS data set including this time period has already been released. We hypothesized that a developmental delay would be less common in toddlers whose mother had used an air purifier during pregnancy.
Methods
Study design and participants
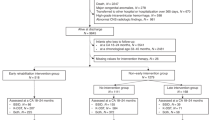
The detailed design and baseline characteristics of the JECS have been published elsewhere13,14,15. Briefly, the JECS is a nationwide, government-funded, birth cohort study of various environmental factors and children’s health and development [registered at UMIN.ac.jp as UMIN000030786 (15/01/2018)]. The participants in the JECS were registered via face-to-face recruitment in 15 regional centres throughout Japan between January 2011 and March 2014. The present study analysed the jecs-ta-20190930 data set, which was released in October 2019. This data set includes data on 103,060 pregnancies up to 3 years postpartum. From this set, we excluded records with inadequate data for analysis, such as those involving multiple participations (the second or third registration of the same mother), multiple births (twins or more), miscarriages/still births, and completely missing data, leaving 82,457 mother-toddler pairs for the final analysis (Fig. 1).

Participants’ flow chart.
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on research involving human participants and with the Helsinki Declaration of 1975, as revised in 2008. All procedures involving human participants were approved by the Ministry of the Environment’s Institutional Review Board on Epidemiological Studies (no. 100910001) and the Ethics Committee of the University of Toyama (no. R2018023). Written informed consent was obtained from all mother-toddler pairs.
Measures
Exposure
The use of air purifiers during the previous year was assessed as part of a series of questions regarding the dwelling house and environment in the second/third trimester (27.8 ± 6.4 SD weeks of gestation) using a simple yes/no question: ‘Have you used an air-cleaning device during the last year?’.
Outcomes
Children’s neurodevelopment at 1.5, 2.0, 2.5, and 3.0 years of age was assessed using the ASQ-3TM, an age-specific, structured, parent-completed, child monitoring system16. The ASQ-3 is a set of well-validated questionnaires that has been recommended by the United Nations Children’s Fund to verify whether children have normal neurological development17. The Japanese version of the ASQ-3 has also been validated18 and has already been used in several studies11,19. The ASQ-3 assesses the following five areas of development: (a) communication: language skills, such as babbling, vocalizing, listening, and understanding; (b) gross motor: arm, body, and leg movements during movement and play; (c) fine motor: hand and finger movements; (d) problem solving: problem-solving skills, learning, and playing with toys; and (e) personal-social: self-help skills, solitary social play, and play with toys and others. Screen-positive cases for each area are defined as those with scores on or below the cut-off values18. Taking early delivery into account, if a parent’s completion dates at 1.5, 2.0, 2.5, and 3.0 years were not within ± 1 month of the estimated delivery date, the data were treated as missing values in accordance with the scoring guidelines.
Covariates
We used the same potential confounders that were used in our previous study11 together with one new confounder. A priori-selected covariates included maternal age (< 25, 25– < 30, 30– < 35, or ≥ 35 years), body mass index (< 18.5, 18.5– < 25, or ≥ 25 kg/m2), parity (primiparous or multiparous), smoking status (never, former, or current), passive smoking status (almost never or 1, 2–3, 4–6, or 7 days/week), alcohol intake (never, former, or current), number of hours spent outdoors (< 1, 1– < 2, 2– < 3, or ≥ 3 h), physical activity (yes or no), folic acid intake20 (≤ 151, 152–202, 203–257, 258–337, or ≥ 338 µg) assessed using a food frequency questionnaire21, marital status (married, single, or divorced or widowed), highest educational level (≤ 12, > 12– < 16, or ≥ 16 years), employment status (yes or no), and annual household income (< 4, 4– < 6, or ≥ 6 million JPY), type of residence (wooden detached house, steel-frame detached house, wooden multiple dwelling house/apartment, steel-frame multiple dwelling house/apartment, or other), high-rise living22 (living ≥ 6th floor or not), number of rooms in the house/apartment (≤ 2, 3, 4, 5, or ≥ 6), living room flooring material (tatami [Japanese straw floor covering], carpet on tatami, wooden flooring/tiles, carpet on wooden flooring/tiles, or other), age of house/apartment building (< 1, 1– < 3, 3– < 5, 5– < 10, 10– < 20, or ≥ 20 years or unknown), house renovation/interior completion after becoming pregnant (yes or no), number of years living in the current place of residence (< 1, 1– < 3, 3– < 5, 5– < 10, 10– < 20, or ≥ 20 years), due date of delivery (months from 1 January 2011), and 19 study areas. These covariates were selected because they are standard variables for socioeconomic status and dwelling environment in Japan as well as because of their possible impact on exposure and/or outcome. For example, mothers with higher socioeconomic status, in terms of higher income and education and living in a new large house, were considered more likely to be able to afford an air purifier and to be concerned with children’s development. Multiparous mothers tend to use air purifiers to keep their house clean and older siblings can affect newborn’s development. In addition, living environment, living place, and the due date of birth can be associated with air pollutant exposure during the potential critical window of foetal development and thus affect both the effectiveness of air purifier use and child development. Potential mediators were not used as covariates. These variables were categorized according to usual medical practice or common practice in Japan and/or by referring to our previous studies23,24,25.
Statistical analysis
To calculate risk ratios (RRs) and their 95% confidence intervals (CIs), we used separate generalized additive mixed models, with 19 study areas in 15 regional centres set as a random effect, with best-fitted spline as a smoothing function for due date of delivery26, with log as a link function, and with binomial and Poisson as distributions for dichotomized and counted outcomes, respectively. Outcome variables were screen-positive cases in the five developmental areas of the ASQ-3: (a) communication, (b) general motor, (c) fine motor, (d) problem solving, and (e) social-personal, as well as (f) the total number of screen-positive cases over the five areas (thus, ranging from 0 to 5). The exposure variable was the yes/no answer to the question regarding air purifier use. Nonuse of air purifiers was used as the reference.
R 4.0.5 mcgv packages including the bam (generalized additive mode for big data) function and SAS 9.4 (SAS Institute Inc., Cary, North Carolina) were used for all statistical analyses.
Missing data
The effective response rates at 1.5, 2.0, 2.5, and 3.0 years postpartum were 85.9% (n = 79,866), 84.5% (n = 78,535), 82.9% (n = 77,029), and 81.2% (n = 75,494), respectively. The missing data rate was highest for annual household income (n = 5618; 6.8%), followed (in order) by hours spent outdoors (n = 3304; 4.0%), physical activity (n = 2732; 3.3%), and years living in the current place of residence (n = 2570; 3.1%). All other covariates had a missing value rate ≤ 1%.
We conducted imputation using chained equations27 to obtain 10 imputed data sets using the MI procedure in SAS. All outcomes and mother’s age, height, and weight as continuous variables and all covariates except for due date of delivery (because of no missing data) as categorical variables were simultaneously imputed. Auxiliary variables that were associated with variables used in the main analysis were introduced to approach the missing at random assumption. For example, we included partner’s highest education level and the number of family members with an income into the imputation model because they effectively predicted income. The ASQ-3 scores at 0.5 and 1.0 years were used to predict the later scores (i.e., 1.5–3.0 years). The estimates from each data set after multiple imputation were combined using Rubin’s rule28.
Sensitivity analysis
Complete case analysis was conducted in addition to the main analysis. We have also checked the assumption of unbiased complete case analysis that missingness depends on the outcome when controlling for all other covariates29 (e.g., is income missingness associated with the neurodevelopment score when controlling for other covariates?). We checked the significance of a total of 420 β-coefficients (i.e., 21 covariates as used in the main analysis × 5 kinds of outcomes as continuous variables × 4 time points) using linear models.
Additional analysis
We calculated generalized variance inflation factors to assess multicollinearity.
Results
The characteristics of the mothers and dwelling environments together with data regarding air purifier use during pregnancy are presented in Table 1. Higher air purifier use was associated with multiple variables; in descending order by strength of relationship, the top five covariates were newer house (Cramer’s V = 0.104), higher income (V = 0.090), living room flooring materials (V = 0.080), multiparous status (V = 0.074), and numbers of rooms in the house (V = 0.067).
Cases and prevalence of developmental delay are presented in Table 2. All prevalences were lower in the air purifier use group than in the air purifier nonuse group.
Crude and adjusted RRs are presented in Fig. 2. All RRs were below the reference (= 1). They ranged from 0.767 to 0.927 and all but one 95% CI did not cross 1.

Tree plot of adjusted risk ratios (RRs) and 95% confidence intervals (CIs) for cases of developmental delay at four time points in various areas of the Ages and Stages Questionnaire, Third Edition, and the total number of cases with air purifier use (reference = nonuse of air purifiers). Based on imputed data for the 82,457 mother-toddler pairs in this study. Adjusted for maternal age, body mass index, parity, smoking status, passive smoking status, alcohol intake, number of hours spent outdoors, physical activity, folic acid intake, marital status, highest educational level, employment status, annual household income, type of residence, high-rise living, number of rooms in house/apartment, living room flooring material, age of house/apartment building, house renovation/interior completion after becoming pregnant, number of years living in current place of residence, and due date of delivery, with the 19 regional areas set as a random effect.
The results of complete case analysis were largely unchanged (Supplementary Fig. 1). In addition, analysis checking the unbiased assumption of complete case analysis detected only 11 significant β-coefficients out of a total of 420 ASQ-3 scores. Given that 21 significant β-coefficients were expected (i.e., α = 0.05), the result suggests that the current complete case analysis yielded unbiased results.
Multicollinearity was not detected among any covariate; that is, all generalized variance inflation factors were below 2.73.
Discussion
As an extension of our previous study11, we used recently fixed JECS data and examined the prospective relationship between the use of air purifiers during pregnancy and neurodevelopmental delay in toddlers up to 3 years of age. Our analysis revealed fewer cases of neurodevelopmental delay in toddlers who were born to mothers who had used an air purifier during pregnancy compared with children of mothers who had not used a purifier. These findings suggest that air purifier use during pregnancy is associated with lower prevalence of neurodevelopmental delay in offspring, despite the developmental outcomes being set to 1.5 to 3 years of age.
Previous studies examined school-aged children4 and 5-year-old children5 at a single time point. In contrast, the current series of studies examined children up to 3 years of age at fixed intervals of 6 months. Taken together with our previous findings that focused on a neurodevelopmental delay up to 1 year of age11, we can conclude that the trajectory of the difference between the use or nonuse of air purifiers appeared as early as at 6 months of age, with the difference further increasing from 1 to 1.5 years of age and remaining the same until at least 3 years of age. Although the difference tended to decrease at 3 years of age in terms of the total number of cases, the tendency was not as clear. In addition, taken together with the previous detection of differences at later ages4,5, the possibility that the difference detected in our data at 3 years of age disappears immediately is likely to be very low.
Although the present study revealed that the maternal use of air purifiers was related to the development of their offspring until at least 3 years of age, this association is not causal but prospective. This means that there is no guarantee that the use of air purifiers during pregnancy would protect against neurodevelopmental delay in offspring. Furthermore, it remains unknown which property of air purifier use would mitigate neurodevelopmental delay, although we considered indoor PM to be one factor and used multiple possible confounders that affect exposure and/or outcome to adjust the model. This is because, firstly, we did not measure actual indoor PM levels. Secondly, we did not measure the ability of the air purifiers to reduce the exposure of mothers to such pollutants. Thus, future studies should examine the mechanism underlying the association. In addition to the underlying mechanism, a randomized controlled trial should be conducted to examine causality. Given that not all medications have a clear mechanism of action, a preventive method itself should be developed. Taken together, while the association found in the present study is itself clear, the meaning of this association and how useful it is for preventing neurodevelopmental delay need to be examined further.
The strengths of the study are as follows. First, our sample size was large. We analysed over 82,000 mother-toddler pairs. Second, our sample was recruited from 15 regional centres throughout Japan. In addition, our sample was recruited within the past 10 years. Thus, our sample is plausibly representative of recent Japanese mother-toddler pairs. Third, the dropout rate was relatively low, at about 18.8%, despite the 3-year follow-up. In addition, we imputed data. Thus, any selection bias was likely to be small. Finally, we introduced multiple potential confounders, including not only demographic, socioeconomic, and dwelling environmental variables, but also time and location variables, that can impact air purifier use and neurodevelopment through a potential critical window of pollutant exposure and foetal development. This means that the unpredictable effects of unmeasured confounders should be minimal.
A number of limitations also need to be considered. First, we measured neurodevelopmental delay using the ASQ-3. Although the ASQ-3 is a well-validated questionnaire, it is neither a diagnostic nor objective measure. Thus, although acceptable, the objectivity of the measures is not as high as it could be. Second, we measured the use of air purifiers via a very simple yes/no question. Thus, further analyses, such as one involving a dose–response study using the duration and/or frequency of air purifier use and the numbers owned while controlling for important confounders, such as filter type and household location8 as well as air pollutant levels and meteorological data30, that can more directly impact air purifier use and foetal neurodevelopment, were impossible. Finally, because we did not measure indoor PM concentrations, mediation analysis using the PM concentration was impossible.
In conclusion, we found a negative prospective association between air purifier use during pregnancy and neurodevelopmental delay in offspring up to 3 years of age.
Data availability
Data are unsuitable for public deposition due to ethical restrictions and the legal framework of Japan. It is prohibited by the Act on the Protection of Personal Information (Act No. 57 of 30 May 2003, amendment on 9 September 2015) to publicly deposit data containing personal information. Ethical Guidelines for Medical and Health Research Involving Human Subjects enforced by the Japan Ministry of Education, Culture, Sports, Science and Technology and the Ministry of Health, Labour and Welfare also restrict the open sharing of epidemiologic data. All inquiries about access to data should be sent to: jecs-en@nies.go.jp. The person responsible for handling enquiries sent to this e-mail address is Dr Shoji F. Nakayama, JECS Programme Office, National Institute for Environmental Studies.
References
Guxens, M. et al. Air pollution during pregnancy and childhood cognitive and psychomotor development: Six European birth cohorts. Epidemiology 25, 636–647. https://doi.org/10.1097/EDE.0000000000000133 (2014).
Suades-Gonzalez, E., Gascon, M., Guxens, M. & Sunyer, J. Air pollution and neuropsychological development: A review of the latest evidence. Endocrinology 156, 3473–3482. https://doi.org/10.1210/en.2015-1403 (2015).
Johnson, N. M. et al. Air pollution and children’s health-a review of adverse effects associated with prenatal exposure from fine to ultrafine particulate matter. Environ. Health Prev. Med. 26, 72. https://doi.org/10.1186/s12199-021-00995-5 (2021).
Guxens, M. et al. Air pollution exposure during fetal life, brain morphology, and cognitive function in school-age children. Biol. Psychiat. 84, 295–303. https://doi.org/10.1016/j.biopsych.2018.01.016 (2018).
Perera, F. P. et al. Prenatal airborne polycyclic aromatic hydrocarbon exposure and child IQ at age 5 years. Pediatrics 124, E195–E202. https://doi.org/10.1542/peds.2008-3506 (2009).
Brockmeyer, S. & D’Angiulli, A. How air pollution alters brain development: The role of neuroinflammation. Transl. Neurosci. 7, 24–30. https://doi.org/10.1515/tnsci-2016-0005 (2016).
Fermo, P., Comite, V., Falciola, L., Guglielmi, V. & Miani, A. Efficiency of an air cleaner device in reducing aerosol particulate matter (PM) in indoor environments. Int. J. Environ. Res. Public Health https://doi.org/10.3390/ijerph17010018 (2019).
Kanatani, K. T. et al. Indoor particle counts during Asian dust events under everyday conditions at an apartment in Japan. Environ. Health Prev. Med. 19, 81–88. https://doi.org/10.1007/s12199-013-0356-4 (2014).
Jia-Ying, L. et al. Efficacy of air purifier therapy in allergic rhinitis. Asian Pac. J. Allergy Immunol. 36, 217–221. https://doi.org/10.12932/AP-010717-0109 (2018).
Itazawa, T. et al. The impact of exposure to desert dust on infants’ symptoms and countermeasures to reduce the effects. Allergy 75, 1435–1445. https://doi.org/10.1111/all.14166 (2020).
Matsumura, K., Hamazaki, K., Tsuchida, A., Inadera, H. & JECS Group. Prospective association of air-purifier usage during pregnancy with infant neurodevelopment: A nationwide longitudinal study – Japan Environment and Children’s Study (JECS). J Clin Med 9, 1924. https://doi.org/10.3390/jcm9061924 (2020).
Gilmore, J. H., Knickmeyer, R. C. & Gao, W. Imaging structural and functional brain development in early childhood. Nat. Rev. Neurosci. 19, 123–137. https://doi.org/10.1038/nrn.2018.1 (2018).
Kawamoto, T. et al. Rationale and study design of the Japan environment and children’s study (JECS). BMC Public Health 14, 25. https://doi.org/10.1186/1471-2458-14-25 (2014).
Michikawa, T. et al. Baseline profile of participants in the Japan Environment and Children’s Study (JECS). J. Epidemiol. 28, 99–104. https://doi.org/10.2188/jea.JE20170018 (2018).
Iwai-Shimada, M. et al. Questionnaire results on exposure characteristics of pregnant women participating in the Japan Environment and Children Study (JECS). Environ. Health Prev. Med. 23, 45. https://doi.org/10.1186/s12199-018-0733-0 (2018).
Squires, J. & Bricker, D. Ages & Stages Questionnaires (ASQ-3): A parent-completed child-monitoring system 3rd edn. (Paul H Brookes Publishing Company, Baltimore, 2009).
Korfmacher, J. & Chawla, N. Toolkit of Recommended Curricula and Assessments for Early Childhood Home Visiting. Geneva: UNICEF, https://www.unicef.org/eca/sites/unicef.org.eca/files/2017-11/Toolkit_of_Recommended_Curricula_and_Assessments_for_Home_Visiting_0.pdf (2013).
Mezawa, H. et al. Psychometric profile of the ages and stages Questionnaires, Japanese translation. Pediatr. Int. 61, 1086–1095. https://doi.org/10.1111/ped.13990 (2019).
Minatoya, M. et al. Cat and dog ownership in early life and infant development: A prospective birth cohort study of japan environment and children’s study. Int. J. Environ. Res. Public Health 17, 205. https://doi.org/10.3390/ijerph17010205 (2019).
Gao, Y. et al. New perspective on impact of folic acid supplementation during pregnancy on neurodevelopment/autism in the offspring children—a systematic review. PLoS ONE 11, e0165626. https://doi.org/10.1371/journal.pone.0165626 (2016).
Yokoyama, Y. et al. Validity of Short and Long Self-Administered Food Frequency Questionnaires in Ranking Dietary Intake in Middle-Aged and Elderly Japanese in the Japan Public Health Center-Based Prospective Study for the Next Generation (JPHC-NEXT) Protocol Area. J Epidemiol 26, 420–432. https://doi.org/10.2188/jea.JE20150064 (2016).
Fujiwara, T., Michikawa, T., Suzuki, K., Takebayashi, T. & Yamagata, Z. Impact of high-rise living on children’s development and health: A critical review of literature. Yamanashi Med. J. 29, 1–9 (2014).
Hamazaki, K. et al. Dietary intake of fish and n-3 polyunsaturated fatty acids and risks of perinatal depression: The Japan Environment and Children’s Study (JECS). J. Psychiatr. Res. 98, 9–16. https://doi.org/10.1016/j.jpsychires.2017.11.013 (2018).
Matsumura, K. et al. Education level and risk of postpartum depression: results from the Japan Environment and Children’s Study (JECS). BMC Psychiatry 19, 419. https://doi.org/10.1186/s12888-019-2401-3 (2019).
Matsumura, K., Hamazaki, K., Tsuchida, A., Inadera, H. & JECS Group. Omega-3 fatty acid intake during pregnancy and risk of infant maltreatment: A nationwide birth cohort—the Japan Environment and Children’s Study. Psychol. Med. 1–10. https://doi.org/10.1017/S0033291721002427 (2021, FirstView).
Dominici, F., Samet, J. M. & Zeger, S. L. Combining evidence on air pollution and daily mortality from the 20 largest US cities: A hierarchical modelling strategy. J. R. Stat. Soc. A Stat. 163, 263–284. https://doi.org/10.1111/1467-985x.00170 (2000).
van Buuren, S. Multiple imputation of discrete and continuous data by fully conditional specification. Stat. Methods Med. Res. 16, 219–242. https://doi.org/10.1177/0962280206074463 (2007).
Rubin, D. B. Multiple Imputation for Nonresponse in Surveys (Wiley, New York, 2004).
Hughes, R. A., Heron, J., Sterne, J. A. C. & Tilling, K. Accounting for missing data in statistical analyses: Multiple imputation is not always the answer. Int J Epidemiol 48, 1294–1304. https://doi.org/10.1093/ije/dyz032 (2019).
Schwartz, J. et al. The concentration–response relation between air pollution and daily deaths. Environ Health Perspect. 109, 1001–1006. https://doi.org/10.1289/ehp.011091001 (2001).
Acknowledgements
We are grateful to the JECS participants and to the individuals who performed the data collection. The findings and conclusions of this article are solely the responsibility of the authors and do not represent the official views of the Japanese government.
Funding
The JECS is funded by the Ministry of the Environment, Japan. This funding source played no role in the study’s design; in the collection, analysis, or interpretation of data; in the writing of the report; or in the decision to submit this paper for publication.
Author information
Authors and Affiliations
Consortia
Contributions
K.M. drafted the paper and analysed the data. K.M. and H.I. conceived and designed the study. K.H., A.T., H.I., and the JECS group critically reviewed the draft and checked the analysis. The JECS group collected the data and obtained the funding. K.H. and H.I. provided administrative, technical, and material support. All authors approved the submission of the manuscript in its current form.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Matsumura, K., Hamazaki, K., Tsuchida, A. et al. Prospective association of air purifier use during pregnancy with the neurodevelopment of toddlers in the Japan Environment and Children’s Study. Sci Rep 11, 19454 (2021). https://doi.org/10.1038/s41598-021-98482-y
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-021-98482-y
