
Abstract
The relative contribution of a theory-based intervention to modify high-risk behaviors in training programs is a major priority that remains an open question. Here, we tested whether the family-centered empowerment model used in the educational intervention was effective to modify high-risk behaviors of brucellosis via mother education. A quasi experimental study was conducted on 200 women presenting to healthcare practices in rural areas of Torbat-e Jam, Iran, from April 2020 to February 2021. Four rural areas were randomly assigned to the control and intervention groups. The intervention group received the training program, which included four 2-h sessions and consulting support via social network and messaging service. The control group did not receive any training. SPSS16 was implemented to test multiple statistical analyses. Our finding showed in the intervention group compared with the control group, knowledge, attitude, self-efficacy, self-esteem, and behavior outcomes were significantly changed (P < 0.001) across time during baseline through follow-up. Likewise, there are no differences (P > 0.05) in the change in construct of the family-centered empowerment model and risk behaviors in the control group from baseline to follow-up. Intervention based on a family-centered empowerment model is possible and very acceptable to modify high-risk behaviors of brucellosis by increasing an individual’s knowledge, changing attitude, and promoting self-efficacy and self-esteem.
Trial registration: Iranian Registry of Clinical Trials (IRCT), IRCT20160619028529N12. Registration date: 24/03/2020.
Similar content being viewed by others

Introduction
Brucellosis has been recognized as one of the most important zoonotic infections in the world with more than 500,000 human cases occurring annually in the world1,2. Brucellosis is still endemic in many parts of the world, including Africa3,4, Central Asia5,6,7,8, Mediterranean Basin8,9,10, Latin America11, and the Middle East where health systems rarely prioritize this infection9,12. Therefore, the World Health Organization (WHO) is considered this disease as a neglected zoonosis13. Brucellosis causes milk production decline, infertility, and abortion in cattle goats, swine, sheep, and dogs8,14. It is the most widespread zoonoses transmitted to humans through direct contact with infected animals or aborted fetuses, by consumption of contaminated meat and unpasteurized dairy products, or by inhaling airborne agents4,14. Therefore, farmers, ranchers, animal health personnel, laboratory personnel, abattoir workers, and other people involved in the livestock are the highest occupational risk groups. Human brucellosis has critical public health concerns and causes several symptoms like flue, including fever, fatigue, joint pain, weakness, sweating, malaise, and loss of appetite, weight loss, and arthritis4,15. It is often misdiagnosed as another infection disease, such as typhoid fever and malaria, resulting in underreporting and mistreatments4,14.With the rapid development of urbanization and animal industries, and the lack of appropriate hygienic scales in food handling and animal husbandry, brucellosis is mainly accounted as remaining a public health hazard2,12,14.
In the case of brucellosis, high-risk behaviors, including inappropriate behaviors such as consumption of unpasteurized dairy products, lack of personal protective equipment such as masks and gloves when working in the barn and warehouse, and contact with livestock secretions of infected animals, which are completely related to insufficient knowledge and awareness of people, their self-efficacy status and attitude9,12. Preventing high-risk behavior depends on increasing the level of awareness and improving the level of attitudes and beliefs, and a prerequisite for disease prevention is to have self-efficacy or the belief of people in their abilities to control risky behavior4,6,14,16. Since most livestock are kept mobile and there is no individual identification system, the eradication, and control of this infection may not be achieved by and test, slaughter, and vaccination only. In some regions, vaccination or eradication of infected livestock is not possible4,6. Therefore, prevention of human infection is primarily based on increasing occupational hygiene, food-safety measures, and safety knowledge11,12. Education training program about avoiding high-risk behaviors toward brucellosis (e.g., avoiding consuming contaminated meat and unpasteurized dairy products) and prevention strategies is important component to manage and control brucellosis1,15,17,18. Likewise, taking care of a patient with brucellosis is associated with several complications. Learning about brucellosis symptoms, transmission, and its adverse health effects as well as knowing about prevention strategies and treatment methods during treatment may cause many challenges for caregivers, among which is care burden9,12,18.
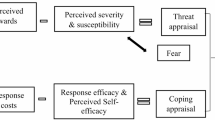
Family-centered care is a care philosophy that recognizes the importance of the family unit as the primary focus point in all health care. In fact, in this way, the patient's family can learn how to help their loved one who is suffering from an acute or chronic illness. The family-centered empowerment model is a theoretical framework that can reduce the level of care burden through increasing self-ability and improving mental and physical function16,19. This model is designed based on the effectiveness of the family members and individuals’ role on the three motivational, self-problem characteristics (knowledge, attitude, and perceived threat) and psychological (self-efficacy and self-esteem)19,20,21. The main target of the family-centered empowerment model is to strengthen the family members to improve the health level of the patient19. This model includes four steps, consisting first step: promoting the knowledge and attitude level through educational sessions. The second and third steps in improving self-efficacy and self-esteem through educational participation; and the fourth step, is evaluating all sessions during the empowerment training19,21,22. The family-centered empowerment model is used in several training programs to promote the care quality, reduce unfavorable side effects of a disease, and enhance patient and caregivers’ confidence21.
Although the data from the Ministry of Health and Medical Education the status of brucellosis in Iran is improving2,12, most parts of Iran are still endemic for brucellosis17,18,23. According to the epidemiologic data on trends of human brucellosis between 1991 and 2008, the yearly occurrence was around 43.24 patients per 100,000 populations2,24. In a recent study on 30 provinces of Iran, the mean incidence of brucellosis was 29.83 patients per 100,000 populations (45% females and 55% males and), and only 4.8% of the population were living in urban areas and 95.2% resided in rural areas12,23. Therefore, human brucellosis still remains a serious public concern in Iran and the situation of Iran among most other countries is troubling12. Although in Iran, livestock vaccination is provided free, the rate of livestock vaccination is low because of breeders’ insufficient awareness about brucellosis’s high-risk behaviors, consequences of untreated infection, transmission pathways, and prevention methods lead24. However, other factors, such as low individual knowledge about prevention methods, concerns about vaccine viability, inappropriate vaccination time and vaccine storage conditions, and inappropriate quarantine conditions mainly affect breeders’ preventive behaviors toward brucellosis18,24. To address this gap in the evidence base, this study aims to investigate the effectiveness of an educational intervention based on the family-centered empowerment model on modifying the high-risk behaviors of brucellosis through mother education.
Methods
Study design and participants
A quasi-experimental study examined the effect of an educational intervention based on a family-centered empowerment model on the management of high-risk behaviors in patients with brucellosis. We conducted this study from April 2020 to February 2021 in rural areas of Torbat-e Jam, Iran. Target population was mothers of patients with brucellosis who were supported by comprehensive rural health service centers in Torbat-e Jam. It was evidenced that there is a significant association between family health and mothering practices because the responsibility of family health falls mainly to the mother. Several studies reported that the mother has a key role in managing all aspects of family health and preventing disease and dealing with ill health25,26. It was assumed that mothers’ knowledge, attitude, and performance about managing brucellosis high-risk behaviors will be improved in the intervention group.
Therefore, we included mother of each family if they: (a) had a patient with brucellosis in their family, (b) living at least 6 months in the main centers of brucellosis, (c) and were aged 15 years ≤. Caregivers were excluded if they were: (a) unwilling to attend a training session and (b) had suffered types of disease and disability such as upper limb disability, visual impairment, and mental disturbance. The sample size were estimated based on the information about mean and standard deviation change of behavior scores between two groups, from a similar study by Babazadeh et al. who evaluated the efficacy of the family-centered empowerment model on the management of high-risk behaviors targeting patients with brucellosis7. Thus, we calculated the sample size equals to 60 participations in each group, using G-power 3.1.5 with consideration α = 0.05, \(\beta\) = 0.2, effect size = 0.54 and 10% loss to follow up rate.
Randomization and recruitment
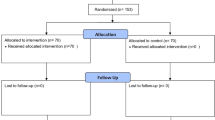
Random allocation of healthcare centers was done based on the Consort-checklist and flow diagram (Fig. 1). All main centers of brucellosis in Torbat-e-Jam were listed according to the rural areas. Fours villages were randomly selected from a list and they were randomly assigned to the control (2 villages) and intervention (2 villages) groups. In each rural, we provided a list of mothers who had a patient with brucellosis in their family. Briefly, 200 mother were randomly selected, of whom 60 mothers have not meet inclusion criteria, and four participants refused to participate in follow-up due to the pregnancy, traveling, and employment problems. Finally, 136 mother were involved in the final analysis and they were assigned to the control (n = 69) and intervention groups (n = 67). All participants filled out a consent form and completed the baseline and follow-up process (Immediately after the intervention and 3 months after intervention) (Fig. 1).

Flow of participants through each stage of the program.
Intervention
We used the Template for Intervention Description and Replication checklist to conduct the intervention program27 (Table 1). The Family-centered empowerment model was used as a framework to design the educational program because it is a suitable social model to assess the determinants that influence an individual’s behavioral patterns and quality of life21.
This model identifies multiple factors that empower the family members in promoting their health. Three dimensions for implementing this model have been identified includes, cognitive, personal traits, and motivation. Eligible mothers in the intervention group received a 2-month training that included four 2-h training sessions (every 15 days) with a focus on the key dimensions of the family-centered empowerment model, which are summarized in Table 2. Trainings were given in groups with 10 people and in the form of group discussions. In this study, we also considered consulting support by phone contact and social media to encourage caregivers to pay more attention to prevention strategies to manage and reduce high-risk behaviors of brucellosis. Consulting support were provided by the trainers for possible questions of the intervention group. A qualified training health educator and a physician provided training sessions and teach-back video, review action, educational pamphlets, and planning reminder card was used to conduct an intervention. In the control group, participants had not received any intervention, and they received a training package when the follow-up periods were finished.
Measuring tools
This study examined the effect of an educational intervention based on a family-centered empowerment model on the management of high-risk behaviors in patients with brucellosis. The outcome of this study was to reduce high-risk behaviors toward brucellosis based on changing cognitive characteristics (self-efficacy and self-esteem), and personal traits (knowledge, attitude, and perceived threat). The intervention based on family-centered empowerment model was considered as an independent variable, and the covariates studied were demographic factors including age, marital status, occupation, education, income, and household size, and history of brucellosis in family members.
The research questionnaires used in the study were as follows: demographic data questionnaire (14 items), high-risk behaviors questionnaire (17 items), and the empowerment evaluation questionnaire (37 items) that included questions on awareness, attitude, perceived threat, Rosenberg’s self-esteem and self-efficacy in high-risk behaviors related to brucellosis.
In this study, we used the family-centered empowerment model as a framework to design a questionnaire. To design the items that related to the family-centered empowerment model and high-risk behaviors, we studied the relevant literature (12) and interviewed 30 caregivers to collect their opinions concerning high-risk behaviors related to brucellosis. Then, an expert panel of ten specialists in health education, epidemiology, and physicians edited assessed the relevance and necessity of all questions to estimate the content validity index (CVI) and content validity ratio (CVR). In this study, the average CVR for the high-risk behaviors questionnaire and the family-centered empowerment questionnaire was 0.88 and 0.98, and CVI for these questionnaires was 0.94 and 0.92, respectively. We examined clarity, readability, and simplicity of questions based on the pilot which included 50 caregivers. The reliability coefficients (Cronbach’s α) of the high-risk behaviors questionnaire and the empowerment evaluation questionnaire were 0.88 and 0.85, respectively, suggesting an acceptable internal consistency of the tool’s criterion (20). Likewise, the appropriate correlation coefficient between all constructs of family-centered empowerment was observed.
Family-centered empowerment questionnaire
The empowerment evaluation questionnaire included questions on changing personal traits (knowledge, attitude, and perceived threat) and cognitive characteristics (self-efficacy and self-esteem). Knowledge about brucellosis was examined by 15 items based on information related to potential risk factors, the transmission of brucellosis in humans, symptoms, and as potential prevention strategies for disease (e.g., Raw and undercooked meat can be effective in transmitting malt fever?), which were ranged on a 3-point scale from 1 (false option), 2 (I don’t know), and 3(correct option). Cronbach’s α of this construct was 0.75. We used 12 items to estimate attitude, and perceived threat (e.g., I believe that livestock vaccination is important to prevent brucellosis in humans, or if I get sick, brucellosis has no side effects for me). All questions were ranged on a three-point scale ranging from 1 (disagree) to 3 (agree) and achieving a higher score meant a more positive attitude. Cronbach’sαon this scale was 0.93. The self-efficacy contained 7 questions (e.g., If I get sick, I can take my medication properly? Or I vaccinate my cattle, even if they cost a lot (with a three-point scale ranging from 1 (disagree) to 3 (agree) (23). Cronbach’sα on this scale was 0.97. Rosenberg’s self-esteem was measured by ten-question (e.g., I feel like a valuable person, at least equal to others?), which were evaluated based on a two-point scale from 1 (disagree) to 2 (agree). Cronbach’s α on this scale was 0.84.
High-risk behaviors
Prevention strategies to manage and reduce high-risk behaviors of brucellosis was examined by 17 questions on factors such as methods of processing milk, dietary habits, husbandry practices, environmental sanitation, and dairy products (e.g., I use masks and gloves when working in the barn and cleaning livestock or I use freshly packaged milk). Items in this questionnaire were rated from 1 (never) to 5 (always), and Cronbach’s α on this scale was 0.99.
Statistical analysis
Data analysis was conducted using the descriptive analysis (mean and standard deviation) and bivariate analyses (chi-square, independent and paired t-tests, and Fischer’s test) to examine variation between different variables in control and intervention groups. We used the repeated measure ANOVA to estimate differences in a different outcome from baseline to follow-up in both groups. The generalized estimating equations (GEE) were also used to examine the effectiveness of the intervention on improving the high-risk behaviors in study population. Likewise, this analytical model allows for the accounting of cluster effects between model constructs (constructs of knowledge, attitude, self-efficacy, self-esteem) and behavior outcomes within an intervention program. We assumed training programs to be nested within improving high-risk behaviors via the Family-centered empowerment model’s constructs. This analytical analysis engaged adjustment for covariates that significantly affected outcomes because the main objective in this survey was examining the effectiveness of the family-centered empowerment model and its constructs on improving high-risk behaviors toward brucellosis. The estimated model constructs for the determinants of high-risk behaviors are accompanied by their 95% confidence interval (CI) and P < 0.05 were considered as significant differences. Data analysis was conducted by SPSS16.
Ethics approval and consent to participate
This article research project approved by Ethics Committee of Mashhad University of Medical Sciences (IR.MUMS.REC.1398.199) and was conducted with consideration of Helsinki Declaration in all phases of the study. Confidential data treatment was guaranteed. Written informed consent was obtained from the participants. Availability of data and materials Data from this study will not be openly available until planned publication outputs have been completed.
Results
We conducted a quasi-experimental study with 136 mothers. The socio-demographic characteristics of the study participants are summarized in Table 3. There were no statistically significant differences in these characteristics from control and intervention groups (P > 0.05). Our finding showed that the mean (± SD) of age and family number for the enrolled participants were 38.02 (± 11.32) and 4.16 (± 1.62), respectively. A majority of the eligible participants were married (94%), housekeepers (94.5%), low-income families (96.2%), and literate (63.7%) (Table 3).
The results of comparing participants’ knowledge, attitude, self-efficacy, self-esteem, and behavior outcomes in control and intervention groups in all-time points (baseline, immediately after intervention, and 3-months follow-up) are explained in Table 4. The results showed that there was no significant difference (P > 0.05) between scores of the family-centered empowerment model’s constructs in control and intervention groups at baseline. Our finding showed that among the participants in the intervention group compared with the control group, knowledge, attitude, self-efficacy, self-esteem, and behavior outcomes were significantly changed (P < 0.001) across time during baseline through follow-up (Table 4). Likewise, there are no significant differences (P > 0.05) in the change in construct of the family-centered empowerment model and risk behaviors in the control group from baseline to follow-up. Thus, the time effects for all constructs were different in the intervention group as compared to the control group. The score of all measurements was significantly increased immediately after intervention (P < 0.001) In the intervention group; but, these scores were decreased overtime at 3 months after the training. In control groups, the time trend was not significant for all constructs (P > 0.05). Based on the results of covariance analysis, the educational intervention had a significant effect on all constructs of the model for all post-intervention measurements and follow-up measurements. Therefore, the training program in this study has led to an increase in the score of participants’ knowledge, attitude, self-efficacy, self-esteem, and behavior outcomes in all measurements after intervention (Table 4).
This result was synchronous with the GEE models that provided significant interaction effects between group and time. The results of this model showed a significant improvement (P < 0.001) in the change in behavior outcome among the participants in the intervention group compared with the control group across time during baseline through follow-up. Likewise, this model showed that among the all constructs of family-centered empowerment, only the attitude construct had a significant direct association (P = 0.019, 95% CI (0.112, 1.4.8)) with behavior outcome (Table 5).
Discussion
Human brucellosis is still considered a major zoonotic infection with a high frequency in many provinces of Iran12,26. Therefore, the implementation of a national brucellosis control program to promote awareness of brucellosis and preventive behaviors among occupational workers and livestock is an important aspect of brucellosis control in both animals and humans24. The purpose of this study was to evaluate the effectiveness of an educational intervention based on the family-centered empowerment model on modifying the high-risk behaviors of brucellosis through mother education. In fact, in this study, we tried to empower the family members to modify their risky behaviors toward brucellosis.
According to the results of this study, the family-centered empowerment model-driven educational intervention significantly modified mothers’ high-risk behaviors toward brucellosis by increasing their knowledge, changing attitudes, and promoting self-efficacy and self-esteem. Our finding confirms that mothers in the intervention group, under theory-based intervention, behaved better in preventing brucellosis and reducing brucellosis incidence in their families. Some studies recently investigated the effect of theory-based educational intervention in the adoption of appropriate behaviors and modification of high risky behaviors to prevent brucellosis in humans and livestock8,15,18,26. They mainly planned the educational interventions based on participants’ experience and knowledge or used other models to behavior change, such as PRECEDE-PROCEED18,23,26 and Health Belief Model (HBM)13,17. Most of these studies highlighted educational theories or models are effective frameworks that can guide providers to truly evaluate the risk of infection and identify preventive methods that can reduce and control the prevalence of the disease13,18,23,26.
However, it was evidenced that educational theories or models are not “culturally versatile” and do not account for socioeconomic characteristics and cultural factors of the target population18,23,26; therefore, several studies recommended conducting the same studies in different socioeconomic and cultural contexts to examine the power of these theories to change behaviors11,13,17,18. Our study is in line with their recommendations that emphasize the interdisciplinary effective survey, such as the combination of health education and brucellosis prevention strategies” to improve the prevalence of brucellosis and its burden in different endemic regions1,14,18. To the best of our knowledge, there is no training program based on a family-centered empowerment model that has examined the combination of health education and brucellosis prevention strategies. In this study, the family-centered empowerment model, as one of the main participatory health models21 which has been used to design training programs, successfully provides a clear appropriate framework to design a participatory intervention program. The significant difference in the level of risky behaviors toward brucellosis in the intervention group compared to the control group confirmed the efficacy of the family-centered empowerment model in modifying high-risk behaviors of brucellosis. Therefore, it is recommended to use such training on improving the health and risky behaviors of livestock breeders and their families through longitudinal studies.
Knowledge and awareness-related behavior is the main construct of the family-centered empowerment model that influences individuals’ practice. In this study, at baseline, the participants lack adequate knowledge and appropriate experience in safe behaviors toward brucellosis. All participants had heard of brucellosis, its zoonotic nature, and what the government was doing regarding brucellosis (vaccination and namely control), but they did not have inadequate and superficial knowledge regarding the recognizing symptoms of brucellosis in humans and animals, mode of transmission, and prevention methods. Poor knowledge scoring was also reported in several studies that evaluate the individuals’ knowledge of brucellosis in Africa3,4 and Asia3,6,8,26, which are the endemic regions of brucellosis. They reported that only approximately half of the population (including livestock and their family members, resident, and other occupation-related groups) knew about brucellosis4,12, which confirms the insufficient level of awareness and knowledge of brucellosis in this region. In Iran, several factors have been identified as main contributors to the low level of brucellosis knowledge is among the livestock value chain such as insufficient knowledge-creating activities provided by veterinary departments and public health agencies12,24,26, low literacy and self-efficacy rates15,17,18, and little training on the handling and rearing of animals7,13,17,26, and a lack of health education programs5,18,25. Our finding also showed that the score of mother’s knowledge was significantly increased immediately after intervention in the intervention group. This might be because of correct training that was provided to identify key concepts to avoid the high-risk behaviors associated with brucellosis. Several studies have indicated that raising the brucellosis-related knowledge is the main aspect that led to a higher stage of change and commitments to modify risky behaviors of brucellosis and inadequate knowledge leads to neglect in disease prevention and treatment4,14,23. Therefore, the implementation and development of brucellosis control programs and more efficient health educational intervention that should fit the perception and needs of the local population are necessary to improve the knowledge and control of brucellosis.
In this study, the mothers in the intervention group showed a greater change in the average score of attitude, as compared with the control group at the follow-up and post-intervention. Likewise, our finding highlighted the role of attitude as the most important determinates on behavior outcome. This might be due to the effect of educational intervention that was clarified the expected benefits of vaccination and preventive strategies associated with brucellosis. In the intervention group, we provided correct information on preventive strategies that is practical to equip individuals in society to safeguard themselves. We also asked participants to share their points of view and personal experiences regarding disease transmission and symptoms. This made respondents show a very positive attitude and willingness to receive more information on brucellosis prevention and treatment. A positive attitude toward the importance of chronic disease in cattle and especially abortion lead to better identification of disease in livestock3,4. It was evidenced that raising the brucellosis-correct information is the main aspect that has influenced their willingness and ability to modify risky behaviors of brucellosis3,4,6,17. Therefore, it is critical for the relevant healthcare professionals and authorities to take note of positive attitude as the main influential factors to modify risky behaviors of brucellosis.
Similarly, the intervention had significant effects on increasing self-efficacy and self-esteem in the intervention group when compared with the control groups, which was consistent with the results of other surveys using the family-centered empowerment model20,21. They highlighted the effect of self‑efficacy on modifying risky behaviors of brucellosis in rural mothers7,18,21. Self‑efficacy is defined “as the perceived ability to perform a target behavior and refers to positive and negative feelings and people's judgments about their ability to master the situation”28. During the training sessions, all mothers learned how to set realistic goals to improve their ability to engage in desired preventive behaviors and practice (e.g. avoiding eating fresh meat and cheese, boiling milk, timely vaccination of livestock, and using protective safe equipment) despite various conflicting situations. We also identified barriers and teach them how to overcome perceived barriers via precise and simple which is leads to creating a sense of self‑efficacy and empowerment in participants. Our result supports other studies that found an increase in the individual's self-efficacy and self-esteem could be made higher stage of commitment to modify healthy behaviors7,17,18,21.
Strengths of the study
Our study is one of the first to examine the effectiveness of an educational intervention-based family-centered empowerment model on brucellosis control and prevention strategies in Iran as the main endemic region of brucellosis in Asia. Testing the application of the educational theories and practices in different communities is essential to improve the theory-based intervention and understand the crucial determinates in the successful training program. A theory-based intervention like the present research tests the power of mediator’s constructs and finds out how these constructs influence an individual’s abilities and attitude to commit to specific behaviors. The findings of this study highlight the importance of theory-based intervention in local settings to modify community’s high-risk behaviors by promoting their knowledge and self-efficacy through utilizing their positive attitudes.
Likewise, in this study, the positive effects of the intervention based on the family-centered empowerment model on successful behavior changes were sustained because the mean scores of mediator constructs in the intervention group were still higher than the mean of these scores in the control group at the follow-up. This could be related to useful theoretical mediator constructs (includes knowledge, attitude, self-efficacy, and self-esteem) that were used in this training program. The content of the questionnaire and educational sessions were tailored based on situational and need assessment. However, the declining trend of the scores in both groups after 3 months reminds the need for continuous. Results from this public health intervention will provide a basis for future educational training aimed at modifying the high-risk behaviors toward brucellosis. It is an acceptable and feasible educational intervention as needs minimal time and investment by the training of rancher family members or occupationally exposed populations.
Limitations
This study is subject to some sources of limitations in the process of design and implementation of the theory-based intervention. Most of the participants had a low level of education or were illiterate. To overcome this bias, we explained and read all items of the research questionnaires for participants so that they could complete the questionnaire. Self-reporting is another limitation in our study that may affect the outcome of investigations. Likewise, there is the possibility that some mediator questions in research questionnaires may not reflect all aspects of the family-centered empowerment model’s constructs in a natural setting. However, the probability of this bias is unlikely to occur because the result of test–retest reliability was more than 0.9 for research questionnaires in this study. In addition, some questions may not be sensitive enough to detect all changes during follow-up because the multiple preventive behaviors were targeted in the training program. Therefore, further studies on family-centered empowerment models are still needed to test its specific change constructs in different populations. Identification of successful mediators constructs to maintain stable behavior are part of a field that needs further investigation via theory-based interventions in the future.
Conclusion
This study contains useful findings to understand the brucellosis control and prevention strategies. International evidence indicates brucellosis requires more attention, and intervention strategies based on behavior change theory are the main method to manage and control brucellosis. Our finding highlighted the family-centered empowerment model-driven educational intervention significantly modified mothers’ high-risk behaviors toward brucellosis. Likewise, the utility of family-centered empowerment model constructs for modifying the high-risk behaviors of brucellosis was supported since individuals in an intervention group moved to a higher stage of change if they had higher knowledge, attitude, self-efficacy, and self-esteem. It appears that the use of family-centered empowerment model and its potential constructs could be used as a promising educational theory to develop behavior change success. Therefore, existing educational sessions between cattle keepers and government veterinary services could be utilized optimally to provide relevant information on human and livestock health, brucellosis control, and prevention strategies. Raising the brucellosis-related knowledge, changing attitude, and promoting self-efficacy and self-esteem would probably be more efficient to modify risky behaviors of brucellosis if provided through the appropriate training program, which in this study was conducted based on a family-centered empowerment model. Likewise, more attention should be paid to improving brucellosis-related knowledge and attitude of the rancher or occupationally exposed populations and to ensure that caregivers are equipped to treat this zoonotic disease.
Data availability
Datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- WHO:
-
World Health Organization
- CI:
-
Confidence interval
- SPSS16:
-
Statistical Package for Social Sciences software
- GEE:
-
The generalized estimating equations
- HBM:
-
Health Belief Model
References
Mataji Amirrood, M. et al. The impact of training on women’s capabilities in modifying their obesity-related dietary behaviors: Applying family-centered empowerment model. J. Res. Health Sci. 14(1), 76–81 (2013).
Ahmadkhani, M. & Aajapjotd, A. Space-time analysis of human brucellosis considering environmental factors in Iran. Asian Pac. J. Trop. Dis. 7(5), 257–265 (2017).
Tempia, S. et al. Brucellosis knowledge, attitudes and practices of a South African communal cattle keeper group. Onderstepoort J. Vet. Res. 86(1), 1–10 (2019).
Mligo, B. J. et al. Knowledge, attitude and practices of frontline health workers in relation to detection of brucellosis in rural settings of Tanzania: A cross-sectional study. One Health Outlook 4(1), 1–12 (2022).
Baron-Epel, O. et al. A cross sectional survey assessing knowledge, attitudes and behaviors regarding brucellosis among Arab Israelis. BMC Public Health 18(1), 1–8 (2018).
Alqahtani, Y. A. et al. Knowledge, attitudes, and practices regarding Brucellosis among parents in Aseer Region, Southwestern Saudi Arabia. In Healthcare (Multidisciplinary Digital Publishing Institute, 2021).
Babazadeh, T. et al. Effect of educational intervention based on family-centered empowerment model in high risk behavior modification among patients with brucellosis. Jorjani Biomed. J. 4(2), 81–91 (2016).
Wang, Z. et al. Brucellosis knowledge and personal protective equipment usage among high-risk populations in Brucellosis-Endemic areas—China, 2019–2020. China CDC Wkly. 3(6), 106 (2021).
Zhang, N. et al. Brucellosis awareness and knowledge in communities worldwide: A systematic review and meta-analysis of 79 observational studies. PLoS Negl. Trop. Dis. 13(5), e0007366 (2019).
Aydin, M. Acute pancreatitis and low ascites-serum albumin gradient ascites caused by Brucellosis: Brucellosis related ascites. Med. Sci. Discov. 8(8), 470–474 (2021).
López-Merino, A. Brucellosis in Latin America. In Brucellosis: Clinical and Laboratory Aspects 151–161 (CRC Press, 2020).
Bahmani, N. & Bahmani, A. A review of brucellosis in the Middle East and control of animal brucellosis in an Iranian experience. Rev. Med. Microbiol. 33(1), e63–e69 (2022).
Shahnavazi, M., Gholamreza, M., Ansari-Moghadam, A., Raeisy, D. & Varnamkhasti Khashei, F. Preventive behaviors of Brucellosis in Khash City Ranchers based on Health Belief Model. Iran. J. Health Educ. Health Promot. 4(4), 281–288 (2016).
Zhai, M. et al. Research on the predictive effect of a combined model of ARIMA and neural networks on human brucellosis in Shanxi Province, China: A time series predictive analysis. BMC Infect. Dis. 21(1), 1–12 (2021).
Eskandari, Z. et al. The effect of educational program based on the health belief model on brucellosis preventive behaviors among traditional ranchers in rural areas of Hamadan Province. J. Educ. Community Health 3(4), 16–23 (2017).
Krisnana, I. et al. Reducing acute stress disorders in mothers of leukemic children by means of the Family Centered Empowerment module (FACE). Cent. Eur. J. Nurs. Midwifery 10(2), 1035 (2019).
Babaei, V. et al. The effectiveness of an educational intervention based on the health belief model in the empowerment of stockbreeders against high-risk behaviors associated with brucellosis. J. Educ. Community Health 1(3), 12–19 (2014).
Bahadori, F. et al. Application of the PRECEDE-PROCEED model in prevention of brucellosis focused on livestock vaccination process. BMC Vet. Res. 17(1), 1–13 (2021).
Dalvand, H., Rassafiani, M. & Bagheri, H. Family centered approach: A literature review. Mod. Rehabil. 8, 1 (2014).
Moradian, S. T. Family-centered care: An evolutionary concept analysis. Int. J. Med. Rev. 5(2), 82–86 (2018).
Rahimibashar, F., Salesi, M. & Alhani, F. A review of 15 years application the family centered empowerment model on the consequences of acute and chronic diseases. J. Mil. Med. 21(4), 325–341 (2019).
Barkhordari-Sharifabad, M., Saberinejad, K. & Nasiriani, K. The effect of health literacy promotion through virtual education on the self-care behaviors in patients with heart failure: A clinical trial. J. Health Literacy 6(1), 51–60 (2021).
Fadaei, E. et al. Effect of health educational intervention based on the educational phase of the PRECEDE-PROCEED model on the promotion of preventive behaviors of Brucellosis in the Villagers of Minoodasht, Iran. J. Educ. Community Health 8(3), 203–208 (2021).
Behzadifar, M. et al. A policy analysis of agenda-setting of Brucellosis in Iran using a multiple-stream framework: Health policy and historical implications. J. Prev. Med. Hyg. 62(2), E544 (2021).
Shahroodi, M. V. et al. Effect of a theory-based educational intervention for enhancing nutrition and physical activity among Iranian women: A randomised control trial. Public Health Nutr. 24(18), 6046–6057 (2021).
Alizadeh-Siuki, H. et al. Behavioral determinants of brucellosis incidence among stockbreeders and their family members in rural area based on PRECEDE model. J. Educ. Health Promotion 9, 25 (2020).
Yamato, T. P. et al. Rasch analysis suggested that items from the template for intervention description and replication (TIDieR) checklist can be summed to create a score. J. Clin. Epidemiol. 101, 28–34 (2018).
Maddux, J. E. Self-efficacy theory. In Self-Efficacy, Adaptation, and Adjustment 3–33 (Springer, 1995).
Acknowledgements
The author wishes to express her gratitude towards the vice president of research in Mashhad University of Medical Sciences.
Funding
This study was supported by grants from the Mashhad University of Medical Science, Iran.
Author information
Authors and Affiliations
Contributions
All authors contributed to conceptualization of the study. M.S.S.H. conducted data collection and health education intervention among women population; S.B.T.S. drafted the work and approved the version to be published and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved; V.G.H. made substantial contributions to the conception or design of the work, analysis or interpretation of data; H.T. supervised project and made substantial contributions to the design and interpretation of data.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Shojaei, M.S., Tavakoly Sany, S.B., Ghavami, V. et al. An educational intervention based on family-centered empowerment model to modify high-risk behaviors of brucellosis via mother education. Sci Rep 12, 18869 (2022). https://doi.org/10.1038/s41598-022-23385-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-022-23385-5
