
Abstract
The present study aimed to clarify the characteristics of young evacuees who had missed the Comprehensive Health Check of the Fukushima Health Management Survey (FHMS) after the Great East Japan Earthquake in 2011. The FHMS has been conducted as a prospective cohort study to evaluate the health status of evacuees annually after the great earthquake in 2011. This study focused on the annual participation rate in the Comprehensive Health Check of evacuees aged between 20 and 37 years in 2011 who evacuated due to the Fukushima Daiichi Nuclear Power Plant accident. The characteristics of subjects who did not participate after the second survey year were identified with a multivariate logistic regression model. The participation rate was estimated at 26.6% (9720 among 36,502 residents) and 15.6% (5691 residents) in 2011 and 2012, respectively. The logistic regression model revealed the following characteristics at baseline as independent predictors of non-participation after the second year of the survey: age ≤ 24 years (adjusted odds ratio 2.11, 95% CI 1.84–2.42), 25–29 years of age (1.28, 1.13–1.45), men (1.52, 1.38–1.69), evacuation outside the municipality but within Fukushima prefecture (1.54, 1.40–1.70), evacuation outside the Fukushima prefecture (1.40, 1.21–1.63), anemia (1.23, 1.06–1.43), smoking habit (1.34, 1.21–1.48), and drinking habit (1.20, 1.09–1.32). A medical history of heart disease showed opposite odds ratios, which indicate the association with continuous participation (0.43, 0.26–0.72, respectively). We observed deteriorated participation in the prospective study of the Comprehensive Health Check of the FHMS among evacuees of a younger age group, men, those evacuated outside their municipalities, and those with history of anemia, smoking and drinking habits. Hence, the cohort study may have missed certain population groups with worse health behaviors. Thus, it is necessary to consider various measures to increase the participation rate in the disaster cohort study to understand the long-term health effects of disasters on younger residents in evacuation zones.
Similar content being viewed by others
Introduction
The Great East Japan Earthquake in 2011 was a triple disaster cascading the earthquakes, the huge tsunami, and the nuclear accident at the Fukushima Daiichi Nuclear Power Plant (FDNPP). Natural disasters themselves cause medical conditions such as injuries, exposure to harmful substances, diseases, and mental health issues1. Delays and barriers in access to medical care indirectly affect human health2. The radiation disaster, such as the nuclear accident of Chornobyl and the atomic bombing of Hiroshima and Nagasaki, which are artificial disasters, could also cause direct and indirect health issues3,4. The current Russia–Ukraine war poses unpredictable radiation hazards in areas surrounding nuclear power plants5. Analyzing past disaster cohorts is essential when considering health measures for future disasters.
It is critical for medical professionals to identify and protect populations vulnerable to disasters. Post-disaster cohort studies have been published for Hurricane Maria6, Hurricane Katrina7, Red river flood8, Sichuan Earthquake9, Fort McMurray Wildfire10, and Sumatra Earthquake11. These studies have consistently shown that the elderly, poor, and structurally disadvantaged populations are more vulnerable to the indirect effects of natural disasters. We experienced a consistent and statistically significant increase in extreme weather conditions and, in turn, natural disasters during the past 30 years, from 1990 to 202012. However, only a few of them are longitudinal studies, and most are small in size. In disaster cohorts, evacuees move to unfamiliar locations from their original residence, making it difficult to track their health status in the long term13. Therefore, the long-term effects of disasters remain unclear.
In response to the Great East Japan Earthquake, the Fukushima prefectural government launched the Fukushima Health Management Survey (FHMS) in June 2011 to investigate the health status of residents and utilize the data obtained for health promotion, with a target population of approximately 2.05 million14. This large-scale prospective cohort study attempted to identify the influence of extended evacuation by reviewing the health information of evacuees, assessing the prevalence of various diseases, and promoting their health. The Comprehensive Health Check, in addition to the Basic Survey of FHMS, has been conducted especially for the residents of all age groups living in evacuation zones designated by the national government because of the FDNPP accident between March 11, 2011, and April 1, 2012. The Comprehensive Health Check evaluates complete blood cell counts with leukocyte fractions, urine occult blood, serum creatinine concentration, estimated glomerular filtration rate, and uric acid in conjunction with regular medical checkups in Japan14.
The FHMS is one of the largest prospective disaster cohort studies to date. The FHMS is a census survey that includes all evacuees and was initiated by the Fukushima prefectural government with a funding of approximately 84 billion yen. The national government of Japan financially supports the FHMS. The prefectural government commissioned Fukushima Medical University to conduct the FHMS. It has revealed disaster-related health risks in residents forced to evacuate for extended periods of time. Because of the evacuation and subsequent lifestyle changes, an increased risk of worsening metabolic diseases such as obesity, dyslipidemia, and diabetes has been observed15,16,17. The prevalence of diabetes mellitus significantly increased after the disaster, and its incidence was significantly greater among evacuees than non-evacuees16. Blood pressure also increased among the victims, especially evacuees, after the Great East Japan Earthquake. The evacuation itself might be associated with an increased risk of hypertension among men18. The survey showed the effects of the disaster on dietary habits: the overall intake of meat and fish among young people decreased after the disaster19. However, the coverage rate of the Comprehensive Health Check of the FHMS has been low, ranging between 20.2 and 30.9% of the total population, despite continuous efforts to promote the study20,21. The characteristics of victims who missed the FHMS have not been sufficiently investigated yet.
We recently analyzed 8 years of data on young evacuees aged between 20 and 44 years who underwent the Comprehensive Health Check of the FHMS and investigated the impact of the Great East Japan Earthquake on anemia22. In the investigation, we found an increase in the number of young evacuees who did not participate in the Comprehensive Health Check during the study period. In this study, we specifically determined the characteristics of young evacuees who had not participated in the Comprehensive Health Check of the FHMS after the second year in this study as an exploratory analysis of the previous report22. The findings of this study suggest ways to improve the coverage of the Comprehensive Health Check and, in turn, contribute to promoting the health status of young evacuees.
Materials and methods
Study design and procedure
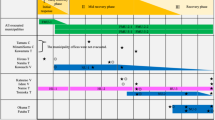
The FHMS is a prospective cohort study which initiated by the Fukushima Prefecture in July 2011 after the Great East Japan Earthquake. The FHMS was prospectively designed for all residents of Fukushima Prefecture to assess the prevalence of diseases and promote their health status. The Comprehensive Health Check, as a part of the FHMS, was intended for those who lived in a nationally designated evacuation area because of the FDNPP accident between March 11, 2011, and April 1, 2011 (Fig. 1 in the Supplement). This study was designed as an exploratory analysis with the FHMS database.
Participants
The subjects of the Comprehensive Health Check were notified annually by mail based on the resident registry of municipalities. After the notification, they receive the Comprehensive Health Check at Fukushima Medical University or individually at designated medical institutions. Even if they move out from the Fukushima prefecture, they can receive the Comprehensive Health Check outside the prefecture by notifying their change of address. Without notification of address change, however, it will be no chance for the eligible individuals to know the opportunity of the Comprehensive Health Check.
Our previous study on anemia in reproductive-age women focused on females aged between 20 and 44 who had participated in the Comprehensive Health Check in FHMS in the 2011 to 2018 survey, where a substantial decrease in the participation rate was observed as the study progressed22. This study targeted the participants of the Comprehensive Health Check aged between 20 and 37 years in 2011, the first survey year, to determine their participation for an 8-year follow-up period as an exploratory analysis of the previous study. Of note, the survey year in 2011 started in July 2011 and ended in March 2012. In the following years, data by March every year were summarized.
Ethical considerations
The institutional review board of Fukushima Medical University approved the FHMS, including exploratory analyses (approval numbers: 1319 for the Comprehensive Health Check, 2020239 for the mental and lifestyle survey, and 29064 for a bridge between the Comprehensive Health Check and mental-lifestyle survey). Written informed consent was obtained from all participants prior to the survey. This study was performed in accordance with the Ethical Guidelines for Medical and Health Research Involving Human Subjects in Japan.
Measures
The primary endpoint of this study is the annual participation status of the Comprehensive Health Check. Secondarily, we assessed the characteristics associated with non-participation after the second survey year of 2012 by utilizing the participant variables in 2011 as a baseline. The survey assessed their evacuation status, body mass index (BMI), blood pressure, medical history, smoking history, alcohol habit, and lipid and glycemic metabolism data.
The evacuation status was classified into the following three groups by comparing the address information on the municipalities between resident registry at pre-quake of March 2011 and at the post-quake initial survey of 2011: evacuation within the same municipality, outside municipality but within Fukushima Prefecture, and outside of the Fukushima Prefecture. The medical history, smoking history, and alcohol habits were captured from the self-reported questionnaire. Participants’ medical history indicated concomitant medical conditions. Smoking history was denoted when participants reported current or past smoking habits. Alcohol habit was indicated by participants’ responses on a four-point Likert scale, ranging from drinking every day to drinking occasionally.
Statistical analysis
The participation rate of the Comprehensive Health Check at the baseline was assessed with the number of participants in the initial survey year divided by the estimated target population in March 2011. The participant characteristics were summarized with descriptive statistics. We classified the study cohort into two groups depending on their participation status: those who did not participate after the second survey and those who attended at least once (the non-participation cohort and the control, respectively). Two-group comparisons were performed using independent t-tests and Pearson’s chi-square tests on continuous and categorical data. We employed multivariate logistic regression analysis to predict the likelihood of missed participation in the Comprehensive Health Check after the second survey year of 2012 for characteristics in the first year of 2011. The explanatory variables include the baseline characteristics of age, gender, BMI, evacuation status, disease histories of hypertension, cerebrovascular disease, heart disease, anemia, diabetes mellitus, dyslipidemia, and kidney disease. We excluded the systolic and diastolic blood pressures, laboratory outcomes of hemoglobin A1c, low-density lipoprotein (LDL) cholesterol, and triglyceride from the multivariate analysis because of colinearities expected with the disease history of hypertension, diabetes mellitus, and dyslipidemia. All statistical analyses were performed using a two-sided approach, and statistical significance was considered when the p value was less than 0.05. Statistical evaluation was performed using the IBM SPSS Statistics version 28 (Armonk, NY, USA).
Results
Coverage of the Comprehensive Health Check in the younger population in the 2011 survey
The target population aged between 20 and 37 years and eligible for the Comprehensive Health Check in the FHMS in March 2011 was estimated as 36,502 persons (eTable 1 in the Supplement). A total of 9720 evacuees (4029 men and 5691 women) participated in the Comprehensive Health Check in 2011. Thus, the participation rate in the initial year of the Comprehensive Health Check was 26.6%. On the other hand, 5691 persons (15.6%) attended the Comprehensive Health Check once or more after the second survey year of 2012 (Fig. 1).

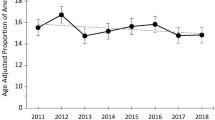
Annual participation of young evacuees in the Comprehensive Health Check of the Fukushima Health Management Survey. The annual change in participation in the Comprehensive Health Check of the Fukushima Health Management Survey (FHMS) is shown. The number of participants was classified according to year (A). The number of individual visits during the study period between 2011 and 2018 was counted (B). The annual percentage of participants is shown after classifying by the number of visits during the study period (C).
The median number [interquartile range] of visits for Comprehensive Health Check was 21,2,3,4 during the survey years 2011–2018. Four thousand twenty-nine evacuees, accounting for 41% of the 2011 survey participants, did not attend the Comprehensive Health Check after 2012. In contrast, 80% or more of the participants after the 2014 survey visited four times or more during the study period. The proportion of men declined by approximately 10% after 2014 compared to 2011 (Fig. 2 in the Supplement). The proportion of those aged between 20 and 25 years decreased to approximately 15% after 2013 compared to 2011.
Univariate assessment on the characteristics associated with non-participation after the second survey
We compared the characteristics of participants who did not attend the Comprehensive Health Check after the 2012 survey (non-participation cohort) with those who participated at least once in 2012 or in the following years (Table 1). The non-participation cohort was significantly younger, with more men, higher BMI, and higher blood pressure when compared to the control (average [standard deviation] or percentage: 29.3 [5.2] and 30.6 [4.8] years old; p < 0.001, 47% and 33% men; p < 0.001, 23.0 [4.5] and 22.6 [4.4] kg/m2 BMI; p < 0.001, and 115 [14] and 114 [14] mmHg systolic blood pressure; p < 0.001, in non-participation cohort and the control, respectively). Significant differences were also observed in the evacuation status (p < 0.001).
No significant differences in medical history were detected between the two groups, except a history of heart disease, which was significantly lower in the non-participation cohort (0.7% and 1.2% in the non-participation and control groups, respectively; p = 0.01).
Significantly higher proportions were seen for smoking history and drinking habit in the non-participation cohort (p for smoking history < 0.001; 38.2% and 29.4%, and p for drinking habit < 0.001; 51.0% and 44.3%, in the non-participation cohort and the others, respectively). No significant differences were found in the metabolic markers of hemoglobin A1c, low-density lipoprotein (LDL) cholesterol, and triglyceride levels between the two groups.
Baseline characteristics associated with non-participation cohort
We examined the baseline characteristics associated with non-participation after the second survey in a multivariate logistic regression model. The multivariate analysis revealed the following variables as the independent predictors of the non-participation: age ≤ 24 years (adjusted odds ratio 2.11, 95% CI 1.84–2.42), 25–29 years of age (1.28, 1.13–1.45), men (1.52, 1.38–1.69), evacuation outside the municipality but within Fukushima prefecture (1.54, 1.40–1.70), evacuation outside the Fukushima prefecture (1.40, 1.21–1.63), medical history of heart disease (0.43, 0.26–0.72), anemia (1.23, 1.06–1.43), smoking habit (1.34, 1.21–1.48), and drinking habit (1.20, 1.09–1.32) (Fig. 2).

Multivariate analysis to predict non-participation in the Comprehensive Health Check in the Fukushima Health Management Survey. A forest plot of the likelihood of non-participation in the Comprehensive Health Check after 2012 is shown. The higher odds indicate a higher likelihood of non-participation after the second survey. aOR adjusted odds ratio, BMI body mass index, CI confidence interval.
Discussion
The FHMS is one of the largest disaster cohort studies in the world and has been conducted for more than a decade. This study revealed a substantial decline in the participation rate of the Comprehensive Health Check during the study period in the evacuees after the FDNPP accident who aged 20–37 years. Despite a large investment and cooperation of public bodies of national and prefectural government and a medical university, the participation rate of the FHMS has been low. The lowering participation rate in the disaster cohort survey may lead to study bias. Thus, efforts should be made to encourage the evacuees in the survey, and careful interpretation is necessary when discussing the study results.
A large reduction in the participation rate was observed between the itinial and second survey years in this study as 4029 (41%) of the 2011 participants did not participate in the second survey year of 2012 or later. Why did they discontinue the Comprehensive Health Check? The health anxiety of the evacuees might be associated with the change in the participation. Residents could not obtain accurate information on radiation doses immediately after the FDNPP accident, and they would have felt anxious about their health because of radiation. On account of the issuance of evacuation orders, many residents were forced to evacuate to temporary housing or other places of residence. The external and internal exposure surveys conducted immediately after the FDNPP accident revealed that the estimated median annual external dose was less than one mSv during the first 4 months between March and July 201123. The internal exposure dose of 99.986% of approximately 184,000 residents was less than one mSv24. A study showed that radiation-related health concerns among evacuees were still high in 2020 compared to those who were not evacuated25. Another study found that radiation-related anxiety among Fukushima residents was resolved over time between 2012 and 201526. It has been noted that people with higher awareness of radiation risks are more likely to participate in internal radiation exposure screening programs. Thus, residents whose health anxiety improved earlier may have discontinued participating in the Comprehensive Health Check.
This study found that younger age (≤ 29 years), men, evacuation outside the municipality, anemia, drinking, and smoking habits were related to discontinuation of participation in the Comprehensive Health Check. Whereas a history of heart disease were associated with continuous participation. Various studies have reported factors that affect the uptake of physical examinations. For instance, a survey identifying factors related to an unwillingness to participate in health examinations among adults aged 19 years and older showed that 9% were unwilling to participate27. Being men, smoking, having higher self-rated health, never been invited before, and not being willing to pay money were related to the unwillingness. An online survey of willingness to participate in secondary prevention programs among individuals aged 18–75 years reported that younger people, men, manual workers, unemployed people, and those who did not regularly practice physical activity were less likely to participate in health check programs5. This study is consistent with such previous studies. The anemia, which was identified as a contributor of non-participation, might be underrecognized in this cohort despite it has been a global health burden, including Japan28. Therefore, it is necessary to proactively educate people who are likely to not participate in secondary prevention programs and encourage them to attend health examinations.
The evacuation outside the municipality regardless within and outside of Fukushima prefecure was also accociated with non-participation after second survey. The evacuation zone after the FDNPP accident was revised multiple times, forcing evacuees to move to different areas frequently29,30. The evacuees have been invited for the Comprehensive Health Check by mail as described in the “Methods” section. Their new address will be easilty identified by the public office if they are within their home municipality, and they will receive the notification of the examination. However, they will not be notified unless they apply for their new addresses outside of the municipality. Combined with the confusion immediately after the earthquake, some evacuees who evacuated outside their home municipality might not know the opportunity of the Comprehensive Health Check. The remote evacuation might contribute to the low rate of participation in the first year of the program as extimated as 26.6%.
Some improvements can be made to minimize their non-participation. We found evacuees with younger ages ≤ 29 years as a predictor of the non-participation. Online communication may help to maintain their participation. Younger and more educated individuals may choose to respond online rather than in person31,32. There is a trend toward the practical application of digital technology in clinical trials that have been progressing during the coronavirus disease (COVID) era33. Financial incentives might encourage continued participation since participation in the FHMS is on a voluntary basis34.
While we believe that this study provides valuable information on post-disaster cohort studies, it has some limitations. First, it is not possible to generalize the results of this study. The FHMS is a disaster cohort study conducted after the Great East Japan Earthquake and the subsequent FDNPP accident. It is not clear whether the results can be replicated for other types of disasters or for disasters occurring in other regions. Second, there was no information on the characteristics of evacuees who did not participate in the entire series of the Comprehensive Health Check. This information cannot be identified unless the present data is combined with the data from health examinations conducted by municipal governments or workplaces. Existing results of health records by the health insurance system should be linked to the FHMS. It takes double effort for evacuees to participate in the Comprehensive Health Check of the FHMS and that of their health insurance system. A study on the reasons for non-participation in health examinations among 35–40 years old individuals found that the most common reasons were lack of time or interference with work35. The impact of evacuation due to the disaster can be investigated in greater detail by linking data from existing pre- and post-disaster medical records and the FHMS. A comparison of the data before and after the earthquake should be considered in the future to identify the populations vulnerable to the effects of major disasters.
Conclusion
We found a lowering participation rate in the Comprehensive Health Check of the FHMS in the evacuees aged 20–37 years, especially among younger evacuees who were men, evacuated outside the municipality, and had histories of anemia, smoking, and drinking habits. We might have missed disaster-related health risks in such evacuees. Having a history of heart disease was associated with continued participation in the survey. It is necessary to consider measures to increase the participation rate in the Comprehensive Health Check of the FHMS.
Data availability
The datasets analyzed during the present study are not publicly available because the data from the Fukushima Health Management Survey belongs to the government of Fukushima Prefecture and can only be used within the organization.
References
Banwell, N., Rutherford, S., Mackey, B., Street, R. & Chu, C. Commonalities between disaster and climate change risks for health: A theoretical framework. Int. J. Environ. Res. Public Health https://doi.org/10.3390/ijerph15030538 (2018).
Balsari, S., Kiang, M. V. & Buckee, C. O. Data in crisis—Rethinking disaster preparedness in the United States. N. Engl. J. Med. 385(16), 1526–1530. https://doi.org/10.1056/NEJMms2104654 (2021).
DiCarlo, A. L., Ramakrishnan, N. & Hatchett, R. J. Radiation combined injury: Overview of NIAID research. Health Phys. 98(6), 863–867. https://doi.org/10.1097/HP.0b013e3181a6ee32 (2010).
Bromet, E. J. & Havenaar, J. M. Psychological and perceived health effects of the chernobyl disaster: A 20-year review. Health Phys. 93(5), 516–521. https://doi.org/10.1097/01.HP.0000279635.14108.02 (2007).
Sawano, T., Tsubokura, M., Ohto, H., Kamiya, K. & Takenoshita, S. An attack on a nuclear power plant during a war is indiscriminate terrorism. Lancet https://doi.org/10.1016/S0140-6736(22)00522-0 (2022).
Santos-Burgoa, C. et al. Differential and persistent risk of excess mortality from Hurricane Maria in Puerto Rico: A time-series analysis. Lancet Planet Health 2(11), e478–e488. https://doi.org/10.1016/s2542-5196(18)30209-2 (2018).
Quast, T., Andel, R. & Sadhu, A. R. Long-term effects of disasters on seniors with diabetes: Evidence from Hurricanes Katrina and Rita. Diabetes Care 42(11), 2090–2097. https://doi.org/10.2337/dc19-0567 (2019).
Tong, V. T., Zotti, M. E. & Hsia, J. Impact of the Red River catastrophic flood on women giving birth in North Dakota, 1994–2000. Matern. Child Health J. 15(3), 281–288. https://doi.org/10.1007/s10995-010-0576-9 (2011).
Xu, X. et al. Food guide Pagoda and the food safety of women: One-year follow-up study on the effects of the 2008 Sichuan Earthquake. Asia Pac. J. Clin. Nutr. 27(3), 662–670. https://doi.org/10.6133/apjcn.092017.08 (2018).
Brown, M. R. G. et al. Mental health symptoms unexpectedly increased in students aged 11–19 years during the 3.5 years after the 2016 fort Mcmurray wildfire: Findings from 9,376 survey responses. Front. Psychiatry 12, 676256. https://doi.org/10.3389/fpsyt.2021.676256 (2021).
Sudaryo, M. K. et al. Injury, disability and quality of life after the 2009 earthquake in Padang, Indonesia: a prospective cohort study of adult survivors. Glob. Health Action 5, 1–11. https://doi.org/10.3402/gha.v5i0.11816 (2012).
Romanello, M. et al. The 2021 report of the Lancet countdown on health and climate change: Code red for a healthy future. Lancet 398(10311), 1619–1662. https://doi.org/10.1016/S0140-6736(21)01787-6 (2021).
van den Berg, B., van der Velden, P., Stellato, R. & Grievink, L. Selective attrition and bias in a longitudinal health survey among survivors of a disaster. BMC Med. Res. Methodol. 7, 8. https://doi.org/10.1186/1471-2288-7-8 (2007).
Yasumura, S. et al. Study protocol for the Fukushima health management survey. J. Epidemiol. 22(5), 375–383. https://doi.org/10.2188/jea.je20120105 (2012).
Kawasaki, Y. et al. The basic data for residents aged 16 years or older who received a comprehensive health check examinations in 2011–2012 as a part of the Fukushima Health Management Survey after the great East Japan Earthquake. Fukushima J. Med. Sci. 60(2), 159–169. https://doi.org/10.5387/fms.2014-31 (2014).
Satoh, H. et al. Evacuation after the Fukushima Daiichi nuclear power plant accident is a cause of diabetes: Results from the Fukushima Health Management Survey. J. Diabetes Res. 2015, 627390. https://doi.org/10.1155/2015/627390 (2015).
Ohira, T. et al. Effect of evacuation on body weight after the Great East Japan Earthquake. Am. J. Prev. Med. 50(5), 553–560. https://doi.org/10.1016/j.amepre.2015.10.008 (2016).
Ohira, T. et al. Evacuation and risk of hypertension after the Great East Japan Earthquake: The Fukushima Health Management Survey. Hypertension 68(3), 558–564. https://doi.org/10.1161/hypertensionaha.116.07499 (2016).
Uemura, M. et al. Association between psychological distress and dietary intake among evacuees after the Great East Japan Earthquake in a cross-sectional study: the Fukushima Health Management Survey. BMJ Open 6(7), e011534. https://doi.org/10.1136/bmjopen-2016-011534 (2016).
Radiation Medical Science Center for the Fukushima health management survey FMU. What is a Comprehensive health check? [cited 2022 24.March]. Available from: https://fukushima-mimamori.jp/physical-examination/outline.html.
Radiation Medical Science Center for the Fukushima health management survey FMU. Fukushima Health Management Survey 'Comprehensive health check' Status of implementation from 2011 to 2019 [cited 2022 24.March]. Available from: https://www.pref.fukushima.lg.jp/uploaded/attachment/369432.pdf.
Yamamoto, K. et al. Changes in the proportion of anemia among young women after the Great East Japan Earthquake: The Fukushima health management survey. Sci. Rep. 12(1), 10805. https://doi.org/10.1038/s41598-022-14992-3 (2022).
Ishikawa, T. Individual doses to the public after the Fukushima nuclear accident. J. Radiat. Prot. Res. 45(2), 53–68. https://doi.org/10.14407/jrpr.2020.45.2.53 (2020).
Kamiya, K. et al. External and internal exposure to Fukushima residents. Radiat. Prot. Dosim. 171(1), 7–13. https://doi.org/10.1093/rpd/ncw185 (2016).
Orui, M. et al. Current psychological distress, post-traumatic stress, and radiation health anxiety remain high for those who have rebuilt permanent homes following the Fukushima nuclear disaster. Int. J. Environ. Res. Public Health https://doi.org/10.3390/ijerph17249532 (2020).
Takebayashi, Y., Lyamzina, Y., Suzuki, Y. & Murakami, M. Risk perception and anxiety regarding radiation after the 2011 Fukushima nuclear power plant accident: A systematic qualitative review. Int. J. Environ. Res. Public Health https://doi.org/10.3390/ijerph14111306 (2017).
de Waard, A. M. et al. Unwillingness to participate in health checks for cardiometabolic diseases: A survey among primary health care patients in five European countries. Health Sci. Rep. 4(2), e256. https://doi.org/10.1002/hsr2.256 (2021).
Kusumi, E. et al. Prevalence of anemia among healthy women in 2 metropolitan areas of Japan. Int. J. Hematol. 84(3), 217–219. https://doi.org/10.1532/IJH97.06097 (2006).
Ministy of Economy TaI. Notice of evacuation orders, etc. to date [cited 2022 24.March]. Available from: https://www.meti.go.jp/earthquake/nuclear/hinan_history.html.
Ryousuke, T. K., Toshio, O. & Kazuhiko, N. A study on the place of refeuge and refuges’ transition process since disaster occurrence until occupancy of temporary housing—From case studies of damaged area in Iwate prefecture. J. Archit. Plann AIJ 79, 2799–2808 (2014).
Marra, C., Gordon, W. J. & Stern, A. D. Use of connected digital products in clinical research following the COVID-19 pandemic: A comprehensive analysis of clinical trials. BMJ Open 11(6), e047341. https://doi.org/10.1136/bmjopen-2020-047341 (2021).
Ebert, J. F., Huibers, L., Christensen, B. & Christensen, M. B. Paper- or web-based questionnaire invitations as a method for data collection: Cross-sectional comparative study of differences in response rate, completeness of data, and financial cost. J. Med. Internet Res. 20(1), e24. https://doi.org/10.2196/jmir.8353 (2018).
Fitzgerald, D. et al. Use of online or paper surveys by Australian women: Longitudinal study of users, devices, and cohort retention. J. Med. Internet Res. 21(3), e10672. https://doi.org/10.2196/10672 (2019).
Haff, N. et al. The role of behavioral economic incentive design and demographic characteristics in financial incentive-based approaches to changing health behaviors: A meta-analysis. Am. J. Health Promot. 29(5), 314–323. https://doi.org/10.4278/ajhp.140714-LIT-333 (2015).
Wall, M. & Teeland, L. Non-participants in a preventive health examination for cardiovascular disease: Characteristics, reasons for non-participation, and willingness to participate in the future. Scand. J. Prim. Health Care 22(4), 248–251. https://doi.org/10.1080/02813430410006611 (2004).
Acknowledgements
We express our gratitude to Ms. Tomoyo Nishimura, Ms. Noriko Miura, Ms. XuJin Zhu, Mr. Kazuki Sekiya, and Ms. Erika Yamashita at Medical Governance Research Institute. The findings and conclusions of this article are solely the responsibility of the authors and do not represent the official views of Fukushima Prefecture government.
Funding
The Fukushima Health Management Survey was supported by the National Health Fund for Children and Adults affected by the Nuclear Incident. Funding providers had no role in the study design, data collection and analysis, decision to publish, or manuscript preparation. No competing interests related to employment, consultancy, patents, products in development, or marketed products are declared.
Author information
Authors and Affiliations
Contributions
Drs. K.Y. and M.T. had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. Concept and design: K.Y., M.T., M.K., M.Tsubokura. Acquisition, analysis, or interpretation of data: All authors. Drafting of the manuscript: K.Y., M.Takita. Critical revision of the manuscript for important intellectual content: T.O., M.M., S.Y., A.S., M.H., K.O., H.Y., M.S., H.O., and K.K. Statistical analysis: K.Y., M.Takita, Y.T. Obtained funding: M.Tsubokura, M.S., H.O., K.K. Administrative, technical, or material support: K.Y., T.Z. Supervision: M.Tsubokura, M.S., H.O., K.K.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Yamamoto, K., Takita, M., Kami, M. et al. Loss of participation among evacuees aged 20–37 years in the disaster cohort study after the Great East Japan Earthquake. Sci Rep 12, 19600 (2022). https://doi.org/10.1038/s41598-022-23896-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-022-23896-1
