
Abstract
Adjuvant S-1 monotherapy is the standard of care for stage II gastric cancer (GC) after curative resection in Japan, but its efficacy for microsatellite instability–high (MSI-H) tumors has remained unknown. Among a multi-institutional cohort of patients with stage II GC who underwent R0 resection followed by S-1 adjuvant chemotherapy between February 2008 and December 2018, we assessed MSI status with an MSI-IVD Kit (Falco). MSI status was assessable for 184 (88.5%) of the 208 enrolled patients, with MSI-H being identified in 24 (13.0%) individuals. Although neither relapse-free survival (RFS) (hazard ratio [HR] = 1.00, p = 0.997) nor overall survival (OS) (HR = 0.66, p = 0.488) differed between MSI-H versus microsatellite-stable (MSS) patients, MSI-H patients showed a nonsignificant but better RFS (HR = 0.34, p = 0.064) and OS (HR = 0.22, p = 0.057) than did MSS patients after adjustment for background characteristics by propensity score (PS) analysis. Gene expression analysis in the PS-matched cohort suggested that recurrence was associated with the immunosuppressive microenvironment in MSI-H tumors but with expression of cancer/testis antigen genes in MSS tumors. Our data reveal a better adjusted survival for MSI-H versus MSS stage II GC treated with S-1 adjuvant therapy, and they suggest that mechanisms of recurrence differ between MSI-H and MSS tumors.
Similar content being viewed by others

Introduction
Gastric cancer (GC) remains one of the most common and deadly cancers worldwide. In Japan, it is the third most common cause of cancer death, with an estimated 43,000 such deaths in 2019. In attempts to improve the survival of GC patients, several combinations of chemotherapeutic agents have been adopted for adjuvant treatment of stage III GC after curative D2 lymph node dissection. On the other hand, for stage II GC, 1-year adjuvant chemotherapy with the oral fluoropyrimidine S-1 has been the standard treatment in Japan based on the ACTS-GC study1, which showed 3-year relapse-free survival (RFS) and overall survival (OS) rates of 72.2% and 80.1%, respectively.
DNA mismatches that occur during cell division are largely restricted to microsatellite regions of the genome, which are composed of repetitive sequences of 2 or 3 bases. Defects in the mechanism of mismatch repair (MMR) can affect the number of such repeats in microsatellite regions, with such an abnormality being known as microsatellite instability (MSI). Tumors with a high MSI are designated as MSI-high (MSI-H)2, with the MSI-H phenotype usually being due to a deficiency in MMR caused by germline mutations in MMR-related genes including MLH1, MSH2, MSH6, and PMS2 or, more commonly, by epigenetic silencing of MLH1 as a result of its hypermethylation. The former mechanism underlying MSI-H status is more prevalent in younger individuals, with the latter being associated with aging2. The Cancer Genome Atlas network has classified GC according to four molecular subtypes: Epstein-Barr virus–infected tumors, MSI tumors, genomically stable tumors, and tumors with chromosomal instability3. Among these subtypes, MSI tumors have received attention for their potential immune reactivity, given the recent development of immune checkpoint inhibitors (ICIs).
Clinical and molecular profiling of MSI-H tumors has been largely limited to colorectal cancer (CRC)4,5. In early-stage CRC, MSI-H is a prognostic indicator for survival and for resistance to fluoropyrimidines, with guidelines now stating that patients with MSI-H stage II disease do not require adjuvant therapy6. In the case of GC, the importance of postoperative adjuvant chemotherapy for MSI-H tumors is currently under debate7,8. An integrated analysis that included the CLASSIC9 and MAGIC10 phase 3 trials showing the benefit of peri- or postoperative adjuvant chemotherapy for stage II/III GC suggested that MSI-H patients do not benefit from adjuvant chemotherapy as much as do microsatellite-stable (MSS) patients11. Other retrospective studies have also suggested that 5-fluorouracil–based adjuvant chemo(radio)therapy does not provide a disease-free survival benefit in patients with MSI-H GC12,13,14. However, these various studies were performed for stage II/III GC and with various chemotherapeutic regimens. No study has previously evaluated 5-fluorouracil monotherapy for MSI-H stage II GC, with such a study being especially important for patients in Japan, where S-1 monotherapy is the standard of care for adjuvant treatment of stage II GC. Furthermore, the true incidence as well as the characteristics of MSI-H stage II GC have remained unclear.
We have therefore now retrospectively investigated the prevalence and characteristics of MSI-H stage II GC and assessed the efficacy of S-1 adjuvant chemotherapy for such tumors compared with MSS stage II GC.
Results
Patients
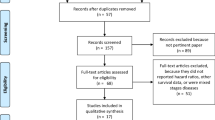
A total of 209 eligible patients was enrolled in the study. To identify MSI-H cases, we screened for MSI status in the 208 tumor samples from the stage II GC patients who received S-1 monotherapy as adjuvant chemotherapy. MSI status was evaluable in 184 samples (88.5%), with MSI-H being detected in 24 cases, yielding a prevalence of MSI-H in the study population of 13.0% (24/184) (Fig. 1). The characteristics of the MSI-H and MSS patients are shown in Table 1. MSI-H patients were older (median age of 70 vs. 67 years, p = 0.016) and tended to have a higher T stage but lower N stage compared with MSS patients, with all MSI-H cases being stage IIb (compared with 56.9% for MSS cases, p < 0.001). The neutrophil-to-lymphocyte ratio (median of 2.25 vs. 1.69, p = 0.086) and serum C-reactive protein concentration (median of 0.12 vs. 0.09 mg/dL, p = 0.543) were numerically higher, whereas the serum albumin level (mean of 3.78 vs. 3.96 g/dL, p = 0.021) was significantly lower, in the MSI-H patients than in the MSS patients. Reflecting their generally poor background, dose reduction for S-1 was more frequent in MSI-H patients than in MSS patients (25.0% vs. 16.9%, p = 0.391), resulting in the duration of S-1 therapy being similar in the two groups (median of 321.0 vs. 327.5 days, respectively). The most common reasons for S-1 discontinuation in MSI-H or MSS patients were adverse events (80% in each group) followed by disease recurrence (10% vs. 9%, respectively).

Flow diagram for study participants.
Prognosis of MSI-H versus MSS stage II GC
We assessed the survival of patients with stage II GC who received S-1 monotherapy after curative D2 resection. The 3-year OS and RFS rates for the entire study population were 91.6% (95% confidence interval [CI], 86.4–94.8%) and 83.6% (95% CI, 77.2–88.3%), respectively (Supplementary Figure 1). There was no significant difference in OS (hazard ratio [HR] of 0.66, with a 95% CI of 0.20–2.16; log-rank p = 0.488) or in RFS (HR of 1.00, with a 95% CI of 0.39–2.55; log-rank p = 0.997) between MSI-H and MSS cases (Fig. 2), with 3-year OS rates of 95.8% and 90.9% and 3-year RFS rates of 82.5% and 83.7% for MSI-H and MSS, respectively.

Overall survival (a) and relapse-free survival (b) for the study subjects according to MSI status.
We further investigated the clinical characteristics of MSI-H versus MSS stage II GC after curative resection (Table 1). There were 3 versus 31 total OS events for MSI-H versus MSS, respectively, with cancer-related death accounting for 1 (33%) versus 19 (61%) of these cases, respectively. The remaining two deaths for the MSI-H cases were due to other causes. Although 26 patients (16.2%) in the MSS group experienced disease recurrence, only 3 patients (12.5%) did so in the MSI-H group. Recurrence sites were varied and included intraperitoneal lymph nodes and liver, or both. Consequently, we analyzed cancer-specific survival (CSS) (Fig. 2c). Although there were no significant differences (hazard ratio [HR] of 0.31 with a 95% CI of 0.04–2.28; log-rank p = 0.249) between MSI-H and MSS cases, there was a trend towards better survival in MSI-H patients.
Given that there were differences in patient background between the MSI-H and MSS groups, we performed propensity score (PS) analysis to correct for potential imbalances. The PS was calculated with a logistic regression model and with sex, age, T stage, N stage, Lauren classification, and S-1 dose modification as explanatory variables. Weighted characteristics for the MSI-H and MSS groups are shown in Supplementary Table 1. After adjusting for the imbalances, we found a better survival for MSI-H versus MSS cases in terms of 3-year OS rate (95.5% vs. 90.9%; HR, 0.22 [95% CI, 0.05–1.05]; log-rank p = 0.057) and 3-year RFS rate (81.3% vs. 59.1%; HR, 0.34 [95% CI, 0.11–1.07]; log-rank p = 0.064), although these differences did not achieve statistical significance likely as a result of the small sample size (Fig. 3).

Overall survival (a) and relapse-free survival (b) according to MSI status with adjustment by propensity score analysis.
Differences in gene expression related to recurrence in MSI-H versus MSS stage II GC
To assess possible differences in recurrence mechanisms between MSI-H and MSS GC, we analyzed gene expression according to recurrence for the PS-matched population. Among tumor samples of the PS-matched cohort, 34 samples (19 MSI-H and 15 MSS tumors), including 7 recurrent cases (3 MSI-H and 4 MSS tumors), were evaluable for such analysis with the Oncomine Immune Response Research Assay. We first compared gene expression between recurrent and nonrecurrent cases, and we found that recurrence was associated with higher expression of cancer/testis antigen (CTA) genes including MAGEA12, GAGE1, and GAGE2C as well as with lower expression of GZMK (Supplementary Figure 2 and Supplementary Table 2). We then compared gene expression associated with recurrence according to MSI status. Of note, gene expression patterns differed markedly between MSI-H and MSS tumors. Among MSI-H tumors, nonrecurrent cases showed higher expression of immune response–related genes including FCGR1A, FCGR3B, GZMB, CD3G, and CCL18 as well as of immune checkpoint genes such as TIGIT and LAG3 (Fig. 4a,b and Supplementary Table 2), suggesting that an adverse change in the tumor immune microenvironment may be associated with recurrence. On the other hand, among MSS tumors, recurrence was associated with higher expression of CTA genes (Fig. 4c,d and Supplementary Table 2). These findings thus suggested that the mechanisms underlying recurrence may differ between MSI-H and MSS tumors treated with adjuvant S-1 monotherapy.

Gene expression in recurrent or nonrecurrent cases according to MSI status in the PS-matched population. Heat maps of immune-related gene expression (a, c) are shown together with corresponding volcano plots (b, d) for recurrent or nonrecurrent cases of MSI-H (a, b) and MSS (c, d) GC. Each colored square in the heat maps represents the average log2[RPM] for expression of the indicated genes in a given patient, with the highest expression indicated in red, median in black, and lowest in green. Genes with a fold change in expression level of more than ± 10 and a p value of < 0.05 were extracted (Supplementary Table 2) and are shown in the heat maps, among which those with a fold change of more than ± 100 are highlighted in red in the heat maps and indicated in the volcano plots.
Discussion
As far as we are aware, our retrospective study is the first to examine the impact of MSI status on the survival of stage II GC patients who receive S-1 adjuvant monotherapy after curative resection. A recent large cohort study revealed the prevalence of MSI-H in GC to be 6.74% (130/1929) in a Japanese population, in which most cases were recurrent or metastatic15. In the present study, MSI-H was identified in 13% of completely resected stage II GC tumors of Japanese patients, suggesting that the prevalence of MSI-H is higher in early-stage tumors and decreases with stage progression, as has been shown for CRC4,5. Consistent with previous findings16, we also found that MSI-H GC cases were common in the distal portion of the stomach and were associated with the intestinal subtype of the Lauren classification as well as with a higher T stage rather than N stage, suggestive of the absence of clear racial or ethnic differences in clinicopathologic characteristics of MSI-H GC. In the current study, MSI-H patients were significantly older than MSS patients, suggesting that hypermethylation of MMR-related genes may be a cause of MSI-H in GC and hence that the condition is sporadic. With regard to age, we also found that nutrition and inflammation status appeared to be worse in MSI-H cases than in MSS cases, with such factors usually being associated with a poor survival17. Furthermore, S-1 dose reduction was required more frequently at the beginning of the adjuvant treatment for MSI-H cases, resulting in a lower S-1 dose intensity compared with MSS cases. Of interest, however, we found that the survival of MSI-H patients was not inferior to that of MSS patients in the current study. Moreover, survival was markedly better for MSI-H patients than for MSS patients after adjustment for patient background by PS analysis. We also found that cancer-specific death was numerically lower in the MSI-H group than in the MSS group.
Whereas S-1 monotherapy has been the standard of care for stage II GC after curative resection based on the ACTS-GC study in Japan1, little has been known of the impact of MSI status on the survival of such treated patients. Our data now suggest that MSI testing may be of benefit for elderly patients with stage II GC, given that MSI-H patients, even those with relatively poor backgrounds, have an excellent prognosis with S-1 postoperative adjuvant chemotherapy. However, it is unclear whether this is due to the inherent good prognosis of MSI-H or to S-1. In this regard, MSI analysis may provide insight into the value of S-1 monotherapy for MSI-H GC in an ongoing study (JCOG1507, BIRDIE study, jRCTs031180255) in which adjuvant S-1 monotherapy is compared with gastric resection alone in vulnerable elderly patients with stage II/III GC.
Our gene expression analysis revealed a potential difference in the mechanisms of recurrence between MSI-H and MSS tumors treated with adjuvant S-1 monotherapy, with recurrence in the former tumors likely being associated with immune suppression in the tumor microenvironment. We found increased CD3G and FCGR1A/3B expression, indicating that immune cells such as T lymphocytes, B lymphocytes, and macrophages were abundant in non-relapsed cases of MSI-H. Furthermore, the expression of GZMB and IL2R, which are the result of the immune response, was also high in MSI-H non-relapsed cases. These results suggest that T cells in tumors from non-relapsed cases of MSI-H were in the early stage of activation and had antitumor activity. Although LAG3 and TIGIT are commonly used as markers of exhausted T cells, these markers are first expressed when T cells are activated by antigen stimulation and are persistently present on the cell surface to gradually exhaust T cells18. Considering other gene expressions indicative of an active immune response, elevations in these markers were likely evidence of immune activity. Although MSI-H tumors in general are thought to have a good prognosis at early stages, data suggest that they have a poor prognosis in the absence of T cell infiltration19. It remains to be determined whether the S-1 adjuvant treatment impacted positively or negatively on such immune suppression tumors apparent in recurrent MSI-H cases in the present study. Developments in perioperative treatment with ICIs for early MSI-H tumors are under way20. Although the efficacy of such ICI-based therapy is generally high for these tumors, it is possible that the clinical benefit is limited to those cases with a poor immune environment, given that MSI-H tumors inherently have a good prognosis20. On the other hand, the expression of CTA genes was associated with recurrence in MSS tumors, consistent with previous results showing that the expression of MAGE and GAGE genes is associated with poor prognosis in GC21,22,23. Given their tumor-specific expression, immunotherapy targeting the proteins encoded by these genes has also been developed (jRCT2080222504). Nonetheless, our data suggest that MSI-H and MSS gastric tumors constitute distinct populations and therefore require the development of different treatment strategies.
Our study has several limitations. First, in this study, we performed PSM with MSI status as the objective variable and sex, age, T stage, N stage, Lauren classification and S-1 dose modification as the explanatory variables, which are clinically considered to have a particular impact on prognosis. Mainly due to sample size, there were limitations in adjusting for background variation with one-to-one matching, especially in making the SMD sufficiently small for factors other than the six explanatory factors listed above. However, the differences were generally smaller than before matching (although not necessarily as small as the SMD value), indicating that it is worthwhile to compare survival rates after adjusting for patient background. Second, the design of the study was retrospective and single arm, lacking data for patients treated with surgery alone. This lack is due to the fact that only samples obtained after S-1 adjuvant therapy became the standard (in 2008) were analyzed so as to ensure DNA quality, with the success of MSI analysis indeed being 88.5% in the present study. Furthermore, patients who still did not receive S-1 adjuvant therapy after the ACTS-GC study appeared to have a markedly different background, such as a poor performance status, and we therefore excluded these individuals. Second, we did not include patients with stage III GC. Our aim was to assess the relation between survival and MSI status among patients who received S-1 monotherapy. Given that various adjuvant regimens—such as docetaxel plus S-124, capecitabine plus oxaliplatin9, and S-1 plus oxaliplatin25—have been administered and that neoadjuvant regimens have recently been evaluated26,27 for stage III GC, data for the effect of MSI status on the efficacy of S-1 adjuvant chemotherapy for stage III GC will likely be of little clinical relevance. Moreover, perioperative therapy with ICIs plus cytotoxic agents has been evaluated for stage II/III GC28,29. A study of preoperative treatment with ipilimumab plus nivolumab for MSI-H GC including that of stage II has recently demonstrated substantial efficacy30 but lacked a chemotherapy cohort as a control. These factors underscore the importance of our data as a reference for future potential adoption of such approaches in clinical practice in Japan.
In summary, we found the prevalence of MSI-H to be 13% in Japanese patients with stage II GC who received S-1 adjuvant chemotherapy. MSI-H status was associated with stage IIb disease and a poor general condition, including a significantly older age and lower serum albumin concentration. Despite such indicators of a poorer prognosis compared with MSS stage II GC, patients with MSI-H GC showed a similar or—after adjustment for such background factors by PS analysis—better survival outcome. Given the potential difference in mechanisms of recurrence between MSI-H and MSS tumors, further study of such mechanisms is warranted, especially with the ongoing evaluation of ICIs for perioperative therapy in GC.
Methods
Patients
Patients included in this study were those who with stage II GC who received S-1 monotherapy as adjuvant chemotherapy after curative D2 resection at five affiliated institutions in Osaka between February 2008 and December 2018. Data regarding clinicopathologic features and treatment history were extracted. We also collected information on general status and laboratory data obtained immediately before adjuvant S-1 administration. Eligible patients were diagnosed with pathological stage II GC according to the 15th edition of the Japanese classification of GC and received S-1 monotherapy as adjuvant chemotherapy on a 1-year schedule after the standard curative D2 lymph node dissection in accordance with corresponding guidelines. Patients who had stage III GC or who received neoadjuvant chemotherapy were excluded. Histological classification and primary site were also determined according to the guidelines. This study was approved by the Institutional Review Board (IRB) of Kindai University Faculty of Medicine (approval number 30–130) in accordance with the Declaration of Helsinki. Patients provided written informed consent, where applicable, or such consent was waived by the IRB of Kindai University Faculty of Medicine, given that the study was retrospective in nature and made use only of deidentified data and excess archival tissue.
Microsatellite analysis
Tumor tissue corresponding to primary GC was collected. The samples were submitted to SRL (CLIA-certified, CAP-accredited central laboratory) for MSI testing with an MSI-IVD Kit (Falco). The procedure included extraction of DNA from normal and tumor components of paraffin-embedded gastrectomy tissue, and MSI status was evaluated by analysis of five microsatellite markers: BAT25, BAT26, NR21, NR24, and MONO27. MSI status was determined as MSI-H if two or more markers were positive. All results were anonymized by SRL, and the aggregated results for MSI status were analyzed in this study.
Gene expression analysis
Sample RNA was extracted from formalin-fixed and paraffin-embedded sections with the use of a MagMAX FFPE DNA/RNA Ultra Kit (Applied Biosystems) and KingFisher Flex Purification System (Thermo Fisher Scientific), and it was quantified with the use of a Qubit instrument and Qubit RNA High Sensitivity (HS) Kit (Invitrogen). Sequencing libraries were constructed with an Ion Torrent Oncomine Immune Response Research Assay Kit (Applied Biosystems). In brief, RNA (10 ng) was subjected to reverse transcription and the resulting cDNA was amplified with primers for the Oncomine assay. Amplicons were digested, ligated to barcode adaptors, and purified with the use of the AMPure XP reagent (Applied Biosystems). Libraries were quantified by real-time polymerase chain reaction analysis and diluted to a concentration of 50 pM before templating on the Ion Torrent Ion Chef instrument and sequencing with the Ion Torrent Ion GeneStudio S5 system and Ion Torrent Ion 540 Kit-Chef. Data were analyzed with the Torrent Server Immune Response RNA Plugin to provide housekeeping and target gene expression levels in absolute read counts, and target gene expression was normalized by housekeeping gene expression as reads per million (RPM) and log2[RPM]. Sample correlation and target gene expression (RPM) clustering heat maps and principal component analysis plots of the top 50 genes with the highest variance were also provided.
Statistical analysis
All statistical analysis was performed with EZR (Saitama Medical Center, Jichi Medical University, Saitama, Japan), which is a graphical user interface for R (The R Foundation for Statistical Computing, Vienna, Austria)31. Differences in categorical variables were assessed with the chi-square test or Fisher’s exact test, and those in continuous variables were evaluated with the independent t test. A p value of < 0.05 was considered statistically significant. The primary statistical outcome was RFS measured in months from the date of surgery to recurrence, death, or final follow-up. RFS curves were estimated with the Kaplan–Meier method and were compared with the log-rank test. OS was also measured from surgical treatment to death from any cause or last follow-up. Patients without documented clinical or radiographic disease recurrence or who were still alive were censored on the date of last follow-up. Follow-up was closed in December 2020. To minimize potential biases from background differences between the MSI-H and MSS groups, the nearest-neighbor matching method using propensity scores was employed. Logistic regression was used for the propensity score calculation from the following variables: sex, age, T stage, N stage, Lauren classification, and S-1 dose modification. A 1:1 matching by propensity scores was performed using a caliper of 0.20. The balance was verified by assessing a p value and standardized mean differences (SMDs).
Ethics approval and consent to participate
The study was performed according to the Declaration of Helsinki and was approved by the Institutional Review Board of Kindai University Faculty of Medicine (approval number 30–130). Patients provided written informed consent, where applicable, or such consent was waived by the Institutional Review Board–approved protocols, given that the study was retrospective in nature and made use only of deidentified data and excess archival tissue.
Data availability
The data sets generated during and/or analyzed during the study are not publicly available due to restrictions of the research ethics protocol but are available from the corresponding author upon reasonable request.
References
Sakuramoto, S. et al. Adjuvant chemotherapy for gastric cancer with S-1, an oral fluoropyrimidine. N. Engl. J. Med. 357, 1810–1820. https://doi.org/10.1056/NEJMoa072252 (2007).
Boland, C. R. & Goel, A. Microsatellite instability in colorectal cancer. Gastroenterology 138, 2073–2087. https://doi.org/10.1053/j.gastro.2009.12.064 (2010).
Comprehensive molecular characterization of gastric adenocarcinoma. Nature 513, 202–209. https://doi.org/10.1038/nature13480 (2014).
Kawakami, H., Zaanan, A. & Sinicrope, F. A. Microsatellite instability testing and its role in the management of colorectal cancer. Curr. Treat. Options Oncol. 16, 30. https://doi.org/10.1007/s11864-015-0348-2 (2015).
Kawakami, H., Zaanan, A. & Sinicrope, F. A. Implications of mismatch repair-deficient status on management of early stage colorectal cancer. J. Gastrointest. Oncol. 6, 676–684. https://doi.org/10.3978/j.issn.2078-6891.2015.065 (2015).
National Comprehensive Cancer Network. Colon Cancer (Version 2.2021). (2021)https://www.nccn.org/professionals/physician_gls/pdf/colon.pdf.
Lordick, F. Chemotherapy for resectable microsatellite instability-high gastric cancer?. Lancet Oncol. 21, 30012. https://doi.org/10.1016/s1470-2045(20)30012-7 (2020).
Smyth, E. C. Chemotherapy for resectable microsatellite instability-high gastric cancer?. Lancet Oncol. 21, 30025. https://doi.org/10.1016/s1470-2045(20)30025-5 (2020).
Bang, Y. J. et al. Adjuvant capecitabine and oxaliplatin for gastric cancer after D2 gastrectomy (CLASSIC): A phase 3 open-label, randomised controlled trial. Lancet 379, 315–321. https://doi.org/10.1016/s0140-6736(11)61873-4 (2012).
Cunningham, D. et al. Perioperative chemotherapy versus surgery alone for resectable gastroesophageal cancer. N. Engl. J. Med. 355, 11–20. https://doi.org/10.1056/NEJMoa055531 (2006).
Pietrantonio, F. et al. Individual patient data meta-analysis of the value of microsatellite instability as a biomarker in gastric cancer. J. Clin. Oncol. 37, 3392–3400. https://doi.org/10.1200/jco.19.01124 (2019).
Kim, S. M. et al. Prognostic value of mismatch repair deficiency in patients with advanced gastric cancer, treated by surgery and adjuvant 5-fluorouracil and leucovorin chemoradiotherapy. Eur. J. Surg. Oncol. J. Eur. Soc. Surg. Oncol. Brit. Assoc. Surg. Oncol. 46, 189–194. https://doi.org/10.1016/j.ejso.2019.08.025 (2020).
Dai, D. et al. Association between the microsatellite instability status and the efficacy of postoperative adjuvant chemoradiotherapy in patients with gastric cancer. Front. Oncol. 9, 1452. https://doi.org/10.3389/fonc.2019.01452 (2019).
Kim, S. Y. et al. The benefit of microsatellite instability is attenuated by chemotherapy in stage II and stage III gastric cancer: Results from a large cohort with subgroup analyses. Int. J. Cancer J. Int. Cancer 137, 819–825. https://doi.org/10.1002/ijc.29449 (2015).
Akagi, K. et al. Real-world data on microsatellite instability status in various unresectable or metastatic solid tumors. Cancer Sci. 112, 1105–1113. https://doi.org/10.1111/cas.14798 (2021).
Ratti, M., Lampis, A., Hahne, J. C., Passalacqua, R. & Valeri, N. Microsatellite instability in gastric cancer: Molecular bases, clinical perspectives, and new treatment approaches. Cell Mol. Life Sci. 75, 4151–4162. https://doi.org/10.1007/s00018-018-2906-9 (2018).
Wang, D. S. et al. Comparison of the prognostic value of various preoperative inflammation-based factors in patients with stage III gastric cancer. Tumour Biol J. Int. Soc. Oncodevelopmental Biol. Med. 33, 749–756. https://doi.org/10.1007/s13277-011-0285-z (2012).
Ruffo, E., Wu, R. C., Bruno, T. C., Workman, C. J. & Vignali, D. A. A. Lymphocyte-activation gene 3 (LAG3): The next immune checkpoint receptor. Semin. Immunol. 42, 101305. https://doi.org/10.1016/j.smim.2019.101305 (2019).
Pagès, F. et al. International validation of the consensus Immunoscore for the classification of colon cancer: A prognostic and accuracy study. Lancet 391, 2128–2139. https://doi.org/10.1016/s0140-6736(18)30789-x (2018).
Shimozaki, K., Nakayama, I., Hirota, T. & Yamaguchi, K. Current strategy to treat immunogenic gastrointestinal cancers: Perspectives for a new era. Cells 12, 12071047. https://doi.org/10.3390/cells12071049 (2023).
Lee, E. K. et al. GAGE12 mediates human gastric carcinoma growth and metastasis. Int. J. Cancer J. Int. Cancer 136, 2284–2292. https://doi.org/10.1002/ijc.29286 (2015).
Kong, U., Koo, J., Choi, K., Park, J. & Chang, H. The expression of GAGE gene can predict aggressive biologic behavior of intestinal type of stomach cancer. Hepatogastroenterology 51, 1519–1523 (2004).
Zambon, A. et al. MAGE, BAGE, and GAGE gene expression in patients with esophageal squamous cell carcinoma and adenocarcinoma of the gastric cardia. Cancer 91, 1882–1888 (2001).
Yoshida, K. et al. Addition of docetaxel to oral fluoropyrimidine improves efficacy in patients with stage III gastric cancer: Interim analysis of JACCRO GC-07, a randomized controlled trial. J. Clin. Oncol. 37, 1296–1304. https://doi.org/10.1200/jco.18.01138 (2019).
Shitara, K. et al. Phase II study of adjuvant chemotherapy of S-1 plus oxaliplatin for patients with stage III gastric cancer after D2 gastrectomy. Gastric Cancer Off. J. Int. Gastric Cancer Assoc. Jpn. Gastric Cancer Assoc. 20, 175–181. https://doi.org/10.1007/s10120-015-0581-1 (2017).
Tokunaga, M. et al. Phase III trial to evaluate the efficacy of neoadjuvant chemotherapy with S-1 plus oxaliplatin followed by D2 gastrectomy with adjuvant S-1 in locally advanced gastric cancer: Japan clinical oncology group study JCOG1509 (NAGISA trial). J. Clin. Oncol. 35, TPS4134–TPS4134. https://doi.org/10.1200/JCO.2017.35.15_suppl.TPS4134 (2017).
Kataoka, K. et al. A randomized Phase II trial of systemic chemotherapy with and without trastuzumab followed by surgery in HER2-positive advanced gastric or esophagogastric junction adenocarcinoma with extensive lymph node metastasis: Japan clinical oncology group study JCOG1301 (Trigger study). Jpn. J. Clin. Oncol. 45, 1082–1086. https://doi.org/10.1093/jjco/hyv134 (2015).
Bang, Y. J. et al. KEYNOTE-585: Phase III study of perioperative chemotherapy with or without pembrolizumab for gastric cancer. Futur. Oncol. 15, 943–952. https://doi.org/10.2217/fon-2018-0581 (2019).
Kelly, R. J. et al. CheckMate 577: A randomized, double-blind, phase 3 study of nivolumab (Nivo) or placebo in patients (Pts) with resected lower esophageal (E) or gastroesophageal junction (GEJ) cancer. J. Clin. Oncol. 35, TPS212–TPS212. https://doi.org/10.1200/JCO.2017.35.4_suppl.TPS212 (2017).
André, T. et al. Neoadjuvant nivolumab plus ipilimumab and adjuvant nivolumab in localized deficient mismatch repair/microsatellite instability-high gastric or esophagogastric junction adenocarcinoma: The GERCOR NEONIPIGA phase II study. J. Clin. Oncol. 41, 255–265. https://doi.org/10.1200/jco.22.00686 (2023).
Kanda, Y. Investigation of the freely available easy-to-use software “EZR” for medical statistics. Bone Marrow Transplant. 48, 452–458. https://doi.org/10.1038/bmt.2012.244 (2013).
Acknowledgements
We thank all the patients, investigators, and medical staff who participated in this study. The study was supported in part by a Grant-in-Aid for Young Scientists from the Japan Society for the Promotion of Science (KAKENHI grant no. JP18K15330).
Author information
Authors and Affiliations
Contributions
C.S. and H.K. conceived and designed the study, developed the methodology, acquired the clinical data, and wrote and edited the manuscript. R.T., H.S., K.I., Y.K., J.F., and R.K. provided samples. C.S., H.K., and Y.C. discussed and interpreted the data. T.S. and K.N. supervised the study.
Corresponding author
Ethics declarations
Competing interests
H.K. has received consulting fees from Bristol-Myers Squibb Co. Ltd., Eli Lilly Japan K.K., MSD K.K., Ono Pharmaceutical Co. Ltd., Daiichi-Sankyo Co. Ltd., and Taiho Pharmaceutical Co. Ltd.; honoraria from Bristol-Myers Squibb Co. Ltd., AstraZeneca K.K., Bayer Yakuhin Ltd., Eli Lilly Japan K.K., MSD K.K., Ono Pharmaceutical Co. Ltd., Chugai Pharmaceutical Co. Ltd., Daiichi Sankyo Co. Ltd., Takeda Pharmaceutical Co. Ltd., and Taiho Pharmaceutical Co. Ltd.; lecture fees from Bristol-Myers Squibb Co. Ltd., Eli Lilly Japan K.K., MSD K.K., Ono Pharmaceutical Co. Ltd., Daiichi Sankyo Co. Ltd., Chugai Pharmaceutical Co. Ltd., Takeda Pharmaceutical Co. Ltd., and Taiho Pharmaceutical Co. Ltd.; and research funding from Bristol-Myers Squibb Co. Ltd., Chugai Pharmaceutical Co. Ltd., Taiho Pharmaceutical Co. Ltd., and Eisai Co. Ltd. H.S. has received honoraria from Bayer Co. Ltd., Bristol-Myers Squibb Co. Ltd., Chugai Pharmaceutical Co. Ltd., Daiichi Sankyo Co. Ltd., Eli Lilly Japan Co. Ltd., Merck Bio Pharma Co. Ltd., MSD Co. Ltd., Ono Pharmaceutical Co. Ltd., Sanofi Co. Ltd., Taiho Pharmaceutical Co. Ltd., Takeda Pharmaceutical Co. Ltd., and Yakult Honsha Co. Ltd., as well as research funding from Ono Pharmaceutical Co. Ltd., Daiichi Sankyo Co. Ltd., Taiho Pharmaceutical Co. Ltd., Takeda Pharmaceutical Co. Ltd., and Sanofi Co. Ltd. Y. K. reports grants and personal fees from Daiichi Sankyo Co. Ltd., outside the submitted work.T.S. reports grants, personal fees and other from Ono Pharmaceutial, grants and personal fees from Chugai Pharmaceutical, grants, personal fees and other from Yakult Honsha, grants and personal fees from Bristol-Myers, grants and personal fees from Elli-Lilly, grants and personal fees from Daiichi-sankyo, other from Takara-Bio, grants from Giliad, grants from BeiGene, grants from MSD, grants and other from Merck-BioPharm, grants and other from Taiho-Pharmaceutical, personal fees from Sanofi-Aventis, other from Takeda Pharmaceutical, outside the submitted work. K.N. reports grants and personal fees from AstraZeneca K.K., grants and personal fees from Astellas Pharma Inc., grants and personal fees from MSD K.K., grants, personal fees and other from Ono Pharmaceutical Co.,Ltd., grants and personal fees from Nippon Boehringer Ingelheim Co.,Ltd., grants and personal fees from Novartis Pharma K.K., grants, personal fees and other from Pfizer Japan Inc., grants and personal fees from Bristol Myers Squibb Company, grants, personal fees and other from Eli Lilly Japan K.K., grants and personal fees from Chugai Pharmaceutical Co.,Ltd., grants and personal fees from Daiichi Sankyo Co., Ltd., grants and personal fees from Merck Biopharma Co., Ltd., during the conduct of the study; personal fees from MEDICUS SHUPPAN,Publishers Co., Ltd., personal fees from Care Net, Inc, personal fees and other from KYORIN Pharmaceutical Co.,Ltd., personal fees from Medical Review Co., Ltd., personal fees from Roche Diagnostics K.K., personal fees from Medical Mobile Communications co., Ltd, personal fees from 3H Clinical Trial Inc., personal fees from Nichi-Iko Pharmaceutical Co., Ltd., grants, personal fees and other from Takeda Pharmaceutical Co.,Ltd., grants and personal fees from Taiho Pharmaceutical Co.,Ltd., grants from SymBio Pharmaceuticals Limited., personal fees from YODOSHA CO., LTD., personal fees from Nikkei Business Publications, Inc, personal fees from Thermo Fisher Scientific K.K., personal fees from YOMIURI TELECASTING CORPORATION., personal fees from Nippon Kayaku Co.,Ltd., grants and personal fees from AbbVie Inc, grants from ICON Japan K.K., grants from PAREXEL International Corp., grants from Kissei Pharmaceutical Co.,Ltd., grants from EPS Corporation., grants from Syneos Health., grants from Pfizer R&D Japan G.K., grants from A2 Healthcare Corp., grants from IQVIA Services JAPAN K.K., grants from Eisai Co., Ltd., grants from CMIC Shift Zero K.K., grants and personal fees from Kyowa Kirin Co.,Ltd, grants and personal fees from Bayer Yakuhin, Ltd, grants from EPS International Co.,Ltd,., grants from Otsuka Pharmaceutical Co., Ltd., personal fees from Hisamitsu Pharmaceutical Co.,Inc., personal fees from NANZANDO Co.,Ltd, personal fees from Amgen Inc., grants from PRA HEALTHSCIENCES, grants from Covance Japan Inc., grants from Medical Reserch Support, grants from Sanofi K.K., grants from PPD-SNBL K.K, grants from Japan Clinical Research Operations, grants from Sysmex Corporation, grants from AbbVie Inc., grants from Mochida Pharmaceutical Co., Ltd., grants from GlaxoSmithKline K.K., outside the submitted work. All remaining authors declare no conflict of interest.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Sato, C., Kawakami, H., Tanaka, R. et al. Survival impact of microsatellite instability in stage II gastric cancer patients who received S-1 adjuvant monotherapy after curative resection. Sci Rep 13, 10826 (2023). https://doi.org/10.1038/s41598-023-37870-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-023-37870-y
