
Abstract
With distinct advantages in clinical application, total knee arthroplasty (TKA) is an effective surgical option for treating end-stage osteoarthritis in the knee. After TKA, incisional problems are one of the major factors influencing the speed in which patients recover. Although it is widely acknowledged that preoperative hypoalbuminemia and the incidence of incisional complications are significantly associated, it is still unclear if postoperative hypoalbuminemia raises the risk of incisional complications following TKA. Furthermore, human serum albumin (HSA) is frequently utilized domestically and internationally to treat postoperative hypoalbuminemia; nevertheless, there is ongoing discussion on whether HSA supplementation can enhance postoperative clinical outcomes. To investigate the relationship between hypoalbuminemia and suboptimal incision healing following TKA, as well as to determine whether HSA supplementation can enhance incision healing after surgery, we collected clinical data for this study. The study sample consisted of 22 patients with poorly healed incisions and 120 cases with normal healing of incisions who underwent TKA treatment for knee osteoarthritis (KOA) in the operator's hospital's Department of Orthopaedics between July 1, 2020, and July 1, 2023. To determine the prevalence of postoperative poor incision healing, data on patients' basic characteristics, preoperative test results, surgical data, postoperative test results, and postoperative incision healing were gathered. The contributing factors to inadequate recovery after surgery were examined using SPSS software. After controlling for confounding variables, a multivariate regression analysis model was used to examine the relationship between postoperative hypoalbuminemia, HSA supplementation, and poor incision healing. 22 cases (15.49%) had poor wound healing following surgery. The findings of multivariate regression analysis after controlling for confounders indicated that there was no correlation between poor wound healing and postoperative albumin level (P > 0.05). Similarly, there was no association (P > 0.05) seen between HSA supplementation and poor incision healing. Following the TKA, postoperative hypoalbuminemia does not raise the risk of incisional problems, and postoperative HSA supplementation neither lowers nor enhances the risk of inadequate incisional healing.
Similar content being viewed by others


Introduction
An increasing number of people with osteoarthritis of the knee have been discovered because of our society's aging population, the prevalence of risk factors like obesity, and rising health awareness1,2. Osteoarthritis of the knee causes joint discomfort, deformity, and dysfunction; the onset of end-stage disease will significantly reduce the prognosis of affected people3. The primary treatment for end-stage knee osteoarthritis (KOA) at this time is total knee arthroplasty (TKA), which can successfully relieve symptoms, correct deformity, restore joint function, and enhance quality of life4. However, this operation is more traumatic, with more intraoperative bleeding and a higher risk of poor incision healing, and it is one of the common complications after TKA5. This complication causes significant psychological and financial hardships for patients and their families in addition to lowering the quality of the patients' postoperative survival. It has been shown that there is a relationship between preoperative hypoalbuminemia and problems during incisional surgery6,7. In clinical work, hypoalbuminemia is more common following TKA; however, there is currently no information about the relationship between poor incision healing following TKA and postoperative hypoalbuminemia. Although guidelines do not support this therapy technique8, human serum albumin (HSA) has been utilized extensively in clinical settings to correct postoperative hypoalbuminemia state to enhance incision healing. The purpose of this study was to further assess the relationship between hypoalbuminemia and poor incision healing following TKA, as well as the effects of postoperative HSA supplementation on incision healing.
Patients and methods
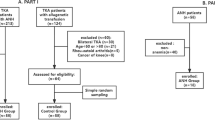
A retrospective collection of patient data was conducted from July 1, 2020, to July 1, 2023, at the Department of Orthopaedics in the First Affiliated Hospital of Harbin Medical University and the Department of Orthopaedics at the Shanghai Public Health Clinical Center. This research focused on patients who underwent TKA for KOA performed by the same surgeon. The inclusion criteria for this study were as follows: (1) meeting the diagnostic criteria for KOA9 and undergoing knee joint surgery for the first time; (2) all surgeries performed by the same surgeon using the medial parapatellar approach; (3) completion of plasma albumin level testing within 3 days post-surgery; (4) voluntary participation in the study and signing of the consent form. The exclusion criteria were as follows: (1) previous knee joint surgery or revision surgery; (2) patients with acute or chronic infections prior to surgery; (3) patients receiving exogenous albumin supplementation before surgery; (4) patients receiving plasma or whole blood transfusion before surgery; (5) long-term use of glucocorticoids or immunodeficiency; (6) concurrent or subsequent additional surgeries during hospitalization; (7) occurrence of other surgery-related complications during follow-up; (8) patients with mental disorders unable to cooperate with the study.
Methods
All inpatient information and post-discharge outpatient follow-up information were collected from the inpatient electronic medical record system, and all patients were followed up for at least 1 month after surgery. The information collected included: basic information (age, BMI, gender); history of underlying diseases (hypertension, diabetes mellitus); preoperative test results (preoperative albumin, preoperative hemoglobin); surgery-related information (anesthesia method, ASA classification, operation time, time of tourniquet use, intraoperative blood loss); and postoperative information ( antimicrobials time, drainage tube staying time, postoperative blood transfusion, postoperative albumin transfusion); test results (postoperative albumin, postoperative hemoglobin); incidence of poor incision healing ( exudation, fat liquefaction, dehiscence, hematoma, etc.) in the 30 d postoperatively.
Diagnostic criteria:(1) Postoperative hypoalbuminemia was defined as plasma albumin < 35 g/L within 3 days after surgery in this study.(2) Poor healing of superficial incisions with inflammatory reaction at the incision, but without suppuration, as proposed by Dennis et al.10 was used as an observational endpoint in this study, which mainly included dehiscence of the incision, fat liquefaction, exudation, hematoma, delayed healing, and necrosis of skin margins, and did not include Incision or prosthesis-related infections.
Statistical analysis
The data was processed using SPSS 26.0 statistical software. The measurement information with a normal distribution was expressed as mean ± SD, and the comparison was made by two independent samples t-test; the measurement information with a skewed distribution was expressed as M (Q1, Q3), and the comparison was made by rank-sum test; the counting information was expressed as frequency and percentage, and the comparison was made by Fisher's exact test or chi-square test. The study employed various independent and dependent variables, including basic patient information, underlying disease history, preoperative test results, surgery-related information, postoperative related information, test results, and the occurrence of poor incision healing within 30 days after surgery. Univariate analyses used incision healing as the dependent variable, and multivariate logistic regression models were utilized to include a single factor if relevant. Confounding factor adjustments were made, and the resulting OR and 95% CI were derived. Statistics were deemed significant if P < 0.05.
Ethics approval and consent to participate
Ethical approval for this study was granted by the Medical Ethics Review Committee of the Shanghai Public Health Clinical Center (Fudan University) (Approval ID: 2024-S012-01). All methods were carried out in accordance with relevant guidelines and regulations. Informed consent was obtained in writing from all the individual participants included in the study.
Consent for publication
Written informed consent was obtained from all patients for publication of this study.
Results
Basic information
Based on the inclusion and exclusion criteria set forth for the study, 142 patients in total were recruited as study participants. The mean age was 65.70 ± 6.34 years, with 31 (21.80%) males and 111 (78.20%) females. The research participants were split into two groups based on incision healing: 22 (15.49%) were in the poor healing group and 120 (84.51%) were in the normal healing group.52(36.60%) were associated with diabetes mellitus, and 33(23.20%) were combined with hypertension. Table 1 shows that 96 subjects (67.61%) had postoperative hypoalbuminemia.
Univariate analyses of factors affecting poor postoperative incision healing
Based on the results of univariate analyses, several factors were found to be significantly associated with poor healing, including age, diabetes mellitus, operation time, time of tourniquet use, intraoperative blood loss, postoperative albumin, and postoperative hemoglobin (all P < 0.05) (Table 1).
Logistic regression analyses of postoperative hypoalbuminemia, albumin supplementation and poor incision healing
After controlling for the confounders, the results of the multivariate logistic regression indicated that there was no correlation between the postoperative albumin level and the occurrence of poor incisional healing (OR = 1.120, 95% CI: 0.952 ~ 1.318, P = 0.172). The results of the univariate logistic regression indicated that there was no correlation between the albumin supplementation and the occurrence of poor incisional healing (OR = 1.387, 95% CI: 0.460 ~ 4.177, P = 0.561) (Table 2).
Discussion
KOA is a common and frequently occurring disease in Orthopaedics, which is prevalent in the elderly over 60 years of age. The end stage often leads to obvious deformity and dysfunction of the knee joint, which seriously affects the quality of life of the patients11,12. TKA is the most used surgical treatment for severe osteoarthritis in the clinic. It can significantly reduce the pain of patients with the end stage, recover or improve the function of the joints, drastically lower the disability rate, and enhance quality of life—advantages that are unmatched by other treatment options13.
Unplanned readmissions after TKA predominantly stem from challenges in incision healing14. A successful postoperative rehabilitation is imperative for patients undergoing TKA, as it directly correlates with optimal incision healing. Inadequate healing of the incision significantly impedes a patient's postoperative recovery, predisposing them to periprosthetic infections15, prolonging hospitalization, and potentially necessitating further debridement16. These complications compound the financial burden and suffering experienced by patients. Given the reduced soft tissue surrounding the incision, heightened local tension, and increased joint activity and mobility, precise attention to the incision site in TKA is paramount. The unique anatomical and kinematic characteristics of this region render surgical incisions particularly vulnerable to suboptimal healing. The probability of perioperative complications may increase when underlying internal medical conditions, such as diabetes and hypertension, are not optimally managed17. Our study did not find any statistically significant differences between the two groups of patients. This observation suggests that most patients in our study cohort had well-controlled internal disorders and were receiving regular and effective therapeutic interventions. Previous research has consistently demonstrated a compelling correlation between malnutrition and the incidence of post-surgical complications18. Notably, the elderly demographic exhibits heightened vulnerability to malnutrition owing to age-related physiological decline. Serum albumin emerges as a pivotal biomarker for assessing the nutritional status of patients undergoing surgical interventions. Within the realm of Orthopaedics surgery, investigations have unveiled a noteworthy correlation between preoperative hypoproteinemia and suboptimal wound healing outcomes6,19. However, in our current inquiry, discernible differences in preoperative albumin levels between comparative cohorts were not statistically significant. Consequently, to elucidate the potential association between preoperative hypoalbuminemia and compromised wound healing, we are poised to augment our sample size to facilitate a more comprehensive investigation.
In the community of postoperative surgical patients, postoperative hypoalbuminemia is also prevalent; prior studies have estimated a frequency of 70–80%20. The total knee replacement procedure is quite invasive, has a high intraoperative and postoperative blood loss rate, and results in a substantial loss of plasma albumin and other nutrients. In a similar vein, we discovered that the group with poorly healing incisions had higher operating times and intraoperative blood losses than the typically healing group but had lower postoperative hemoglobin and albumin levels. Due to the body's stressed hypermetabolic state in the early postoperative phase, proteolytic metabolism speeds up and anabolic metabolism slows down, creating a persistently negative nitrogen balance; Moreover, aged patients have a markedly impaired ability to compensate for surgical stress, making them more vulnerable to hypoalbuminemia throughout the recovery phase. Hypoalbuminemia has the potential to impede fibroblast proliferation, which in turn can lower collagen synthesis and hinder the healing of incisions21. Additionally, a decrease in plasma hypoalbuminemia may result in a decrease in plasma colloid osmolality, which could cause swelling in the surrounding tissues and raise the risk of incisional infection22. Finally, hypoalbuminemia may cause immunosuppression, which could lead to a decline in the body's immunity23. Poor healing of the incision following surgery is theoretically associated with postoperative hypoalbuminemia. Postoperative hypoalbuminemia, however, is simply a transient condition brought on by things like heightened capillary permeability and hemodilution from excessive fluid rehydration during the recovery phase; most patients' indices will recover more significantly in around a week. Research by Kompan et al. on 76 patients who had undergone surgery for abdominal malignancies revealed no correlation between postoperative serum albumin concentrations and postoperative complications24. Our research found that there is no correlation between postoperative hypoalbuminemia and the risk of problems from inadequate incision healing.
Due to its lengthy metabolic cycle (half-life of 15–19 days), albumin is primarily used to assess preoperative nutritional status and chronic malnutrition. However, because it cannot accurately reflect the body's nitrogen balance status following surgery, it is unclear if albumin level can be used as a trustworthy indicator for assessing postoperative nutritional status. Because albumin and transferrin have very short half-lives—1.9 days on average and 8.8 days on average—they are better indicators of patients' short-term nutritional condition following surgery. We are interested in investigating whether albumin and transferrin levels can be used as an indicator for predicting postoperative incision infections in the next stage of our investigation, as there have been less studies that have utilized them to predict postoperative Orthopaedics incision problems.
HSA is a blood product commonly used in clinical treatment and is more commonly used in medical institutions because of its wide range of indications. Surgery and trauma patients are commonly malnourished, and such patients are often accompanied by varying degrees of hypoalbuminemia, it is usually accepted that intravenous infusion of HSA can replenish nutrients and improve the body's immunity or resistance. Most surgeons thought that albumin infusion could reduce incision edema and thus promote incision healing, so albumin infusion was very common in the clinic. However, more and more studies have shown that albumin infusion does not improve incision complications24,25. The same result was obtained in our study. The reasons for this are considered as follows: (1) albumin contains an unbalanced variety of amino acids and lacks certain essential amino acids, so its nutritional value is not high26; (2) exogenous albumin leaks out of the body into the extravascular area after entering the human body, which not only fails to replenish the albumin in the blood but also results in tissue edema, which may affect the healing of the tissues27; and (3) the long-term application of exogenous HSA may make the body develop a certain degree of dependence, negative feedback inhibits the liver to carry out endogenous albumin synthesis, which makes the self-regulation function decline and the recovery time become longer, thus prolonging the hospitalization time. In addition, the American Clinical Guidelines for the Application of Albumin point out that HSA is only used for critically ill patients with extremely low serum albumin levels (< 20 g/L). China's blood supply has always been in a "tight" status, so HSA is in short supply to varying degrees throughout the country, with a high price, and from an economic perspective, it is not recommended for routine use in postoperative hypoalbuminemia patients.
The clinical misapplication of HSA, characterized by deviations from drug indications, oversight of contraindications, neglect of appropriate compounding procedures, and other irrational practices, warrants considerable attention. International studies have highlighted that the rate of clinical inappropriateness regarding albumin administration, either in the absence of clear indications or in deviation from established guidelines, ranges from 40 to 90%28, indicating a substantial global concern. Regrettably, the situation in China mirrors this trend with a lack of optimism. Of particular concern is the prevalent irrational utilization of HSA among special patient populations, notably the elderly and critically ill individuals. Addressing this issue necessitates proactive intervention by pharmacists within medical institutions' drug management departments through the implementation of rigorous doctor's order audits and prescription reviews. Furthermore, this study aims to provide insights into the current practices surrounding HSA administration within our hospital, facilitating the development of a systematic approach for evaluating and analyzing its rational utilization across hospital settings.
Our study also has the following shortcomings: 1. Our research is a retrospective case–control study, bias is inevitable, and we will conduct a prospective study on top of the current foundation; 2. Factors affecting incision healing are complex, and even though our study covers most of the factors that are of interest in clinical and related research, it is unavoidable that we could not take all of them into account, and we will collect further and more comprehensive data in the following stages; 3. Although our results are in agreement with the most of the studies, the sample size of this study is small, and it is still necessary to further validate this conclusion through multicenter and large-sample surveys.
Conclusions
In conclusion, poor incision healing following TKA for osteoarthritis is not increased by postoperative hypoalbuminemia, and neither is it improved by postoperative HSA supplementation. Clinicians ought to endeavor to increase knowledge regarding postoperative hypoalbuminemia, and the routine use of HSA to rectify postoperative hypoalbuminemia following TKA is not recommended. It still needs to be investigated, though, whether varying levels of hypoalbuminemia raise the risk of inadequate incision healing and whether enteral nourishment can help with incision healing.
Data availability
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- HSA:
-
Human serum albumin
- KOA:
-
Knee osteoarthritis
- TKA:
-
Total knee arthroplasty
References
Suri, P., Morgenroth, D. C. & Hunter, D. J. Epidemiology of osteoarthritis and associated comorbidities. PM R. 4, S10-19 (2012).
Lee, R. & Kean, W. F. Obesity and knee osteoarthritis. Inflammopharmacology. 20, 53–58 (2012).
Liu, L., Tian, F., Li, G. Y., Xu, W. & Xia, R. The effects and significance of gut microbiota and its metabolites on the regulation of osteoarthritis: Close coordination of gut-bone axis. Front. Nutr. 9, 1012087 (2022).
Conner-Spady, B. L. et al. Patient expectations and satisfaction 6 and 12 months following total hip and knee replacement. Qual Life Res. 29, 705–719 (2020).
Rezapoor, M. & Parvizi, J. Prevention of periprosthetic joint infection. J. Arthroplasty. 30, 902–907 (2015).
Bohl, D. D., Shen, M. R., Kayupov, E. & Della, V. C. J. Hypoalbuminemia independently predicts surgical site infection, pneumonia, length of stay, and readmission after total joint arthroplasty. J. Arthroplasty. 31, 15–21 (2016).
Bohl, D. D. et al. Malnutrition predicts infectious and wound complications following posterior lumbar spinal fusion. Spine (Phila Pa 1976). 41, 1693–1699 (2016).
Liumbruno, G. M., Bennardello, F., Lattanzio, A., Piccoli, P. & Rossettias, G. Recommendations for the use of albumin and immunoglobulins. Blood Transfus. 7, 216–234 (2009).
Jevsevar, D. S. et al. The american academy of orthopaedic surgeons evidence-based guideline on: Treatment of osteoarthritis of the knee. J. Bone Joint Surg. Am. 95, 1885–1886 (2013).
Godoy, G. et al. Preoperative acute inflammatory markers as predictors for postoperative complications in primary total knee arthroplasty. Ochsner. J. 16, 481–485 (2016).
Cross, M. et al. The global burden of hip and knee osteoarthritis: Estimates from the global burden of disease 2010 study. Ann. Rheum. Dis. 73, 1323–1330 (2014).
Nelson, A. E. Osteoarthritis year in review 2017: Clinical. Osteoarthritis Cartilage. 26, 319–325 (2018).
Price, A. J. et al. Knee replacement. Lancet. 392, 1672–1682 (2018).
Lee, S. W., Kumar, G. K. & Kim, T. K. Unplanned readmissions after primary total knee arthroplasty in korean patients: Rate, causes, and risk factors. Knee. 24, 670–674 (2017).
Harato, K., Tanikawa, H., Morishige, Y., Kaneda, K. & Niki, Y. What are the important surgical factors affecting the wound healing after primary total knee arthroplasty?. J. Orthop. Surg. Res. 11, 7 (2016).
Carroll, K., Dowsey, M., Choong, P. & Peel, T. Risk factors for superficial wound complications in hip and knee arthroplasty. Clin. Microbiol. Infect. 20, 130–135 (2014).
Zmistowski, B. et al. Patients with uncontrolled components of metabolic syndrome have increased risk of complications following total joint arthroplasty. J. Arthroplasty. 28, 904–907 (2013).
Studley, H. O. Percentage of weight loss: A basic indicator of surgical risk in patients with chronic peptic ulcer. Nutr. Hosp. 16, 141–143 (2001).
Nelson, C. L., Elkassabany, N. M., Kamath, A. F. & Liu, J. Low albumin levels, more than morbid obesity, are associated with complications after tka. Clin. Orthop. Relat. Res. 473, 3163–3172 (2015).
Hill, G. L., Douglas, R. G. & Schroeder, D. Metabolic basis for the management of patients undergoing major surgery. World J. Surg. 17, 146–153 (1993).
Testini, M., Margari, A., Amoruso, M., Lissidini, G. & Bonomo, G. M. The dehiscence of colorectal anastomoses: The risk factors. Ann. Ital Chir. 71, 433–440 (2000).
Runyon, B. A. Low-protein-concentration ascitic fluid is predisposed to spontaneous bacterial peritonitis. Gastroenterology. 91, 1343–1346 (1986).
Böhm, M. et al. Association of cardiovascular risk factors with microalbuminuria in hypertensive individuals: The i-search global study. J. Hypertens. 25, 2317–2324 (2007).
Mahkovic-Hergouth, K. & Kompan, L. Is replacement of albumin in major abdominal surgery useful?. J. Clin. Anesthesia. 23, 42–46 (2011).
Berg, S., Golster, M. & Lisander, B. Albumin extravasation and tissue washout of hyaluronan after plasma volume expansion with crystalloid or hypooncotic colloid solutions. Acta Anaesthesiol. Scand. 46, 166–172 (2002).
Matos, G. C., Rozenfeld, S. & Martins, M. Human albumin use at hospitals in the metropolitan region of Rio de Janeiro, Brazil. Cad Saude Publica. 26, 981–990 (2010).
Boldt, J. Use of albumin: An update. Br. J. Anaesth. 104, 276–284 (2010).
Caraceni, P. et al. Clinical indications for the albumin use: Still a controversial issue. Eur. J. Intern. Med. 24, 721–728 (2013).
Funding
The work was supported by grants from Shanghai Public Health Clinical Center Institutional Level Funding Projects; Project number: KY-GW-2024-04 and KY-GW-2020-23).
Author information
Authors and Affiliations
Contributions
J.S.: Provided research ideas, data collection, analysis, literature research, and manuscript writing. G.L.Y.: Data collection, statistical analysis, some involved in manuscript writing. C.L.Y.: Data collection, research method guidance,research object screening, research guidance, manuscript revision and final approval. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Sun, J., Yang, G. & Yang, C. Influence of postoperative hypoalbuminemia and human serum albumin supplementation on incision healing following total knee arthroplasty for knee osteoarthritis: a retrospective study. Sci Rep 14, 17354 (2024). https://doi.org/10.1038/s41598-024-68482-9
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-024-68482-9
Keywords
This article is cited by
-
Effect of electroacupuncture stimulation combined with the enhanced recovery after surgery regimen on motor function recovery following total knee arthroplasty
Journal of NeuroEngineering and Rehabilitation (2025)
-
Relationship between high-sensitivity C-reactive protein to lymphocyte ratio (hs-CLR) and incision complications following medial opening-wedge high tibial osteotomy for knee osteoarthritis
BMC Surgery (2025)
-
Postoperative serum albumin drop predicts complications in primary total knee arthroplasty: a retrospective cohort study using XGBoost algorithm
BMC Musculoskeletal Disorders (2025)
