
Abstract
The aim of this study is to compare the efficacy of different exercise interventions for adult flexible flatfoot. Nine databases (PubMed, EMBASE, Web of Science, the Cochrane Central Register of Controlled Trials (CENTRAL), SCOPUS, PRDro, Google Scholar, China National Knowledge Infrastructure(CNKI) and Wanfang data) were systematically searched from their inception until February 2024. The search resulted in 2112 records, with 11 studies included. All networks revealed low heterogeneity and non-significant inconsistency (I2 ≤ 25.0%). Three network plots were formed for navicular drop. Firstly, compared with the control group, strengthening the posterior tibial muscle + stretching the iliopsoas muscle + TCE (MD: 3.32, 95% CI: 1.78, 4.89), PNF (MD: 1.81, 95%CI: -0.05, 3.70), SFE (MD: 1.23, 95%CI: 1.02, 1.44) all showed better effects. And strengthening the posterior tibial muscle + stretching the iliopsoas muscle + TCE exercise is considered to be the most effective intervention, with SUCRA of 0.97. Secondly, compared with the control group, hip-focused neuromuscular exercise (MD: 6.22, 95% CI: -1.69, 14.12), SFE with EMG biofeedback (MD: -0.81, 95%CI: -1.59, 3.21) all showed better effects. And hip-focused neuromuscular exercise is considered to be the most effective intervention, with SUCRA of 0.92. Thirdly, the internal foot muscle training combined with gluteus muscle strengthening is significantly better than the other two groups, with SUCRA of 0.99. For the foot posture index, comprehensive reinforcement (MD: 1.95, 95% CI − 0.19, 4.03) showed better effects compared with the control group. In the probability ranking table, comprehensive reinforcement is significantly better than the other two groups, with SUCRA of 0.98. For the foot function index, orthoses wear + stretching + eccentric progressive resistive exercise of tibialis posterior is significantly better than the other two groups, with SUCRA of 0.92. In conclusion, various exercise therapies improve the arch shape and function of patients with flexible flatfoot, particularly hip muscle and lower limb overall muscle training.
Similar content being viewed by others

Introduction
Flexible flatfoot is characterized by a flattening of the medial longitudinal arch (MLA) of the foot in a weight-bearing position1. It is present in 13.6–26.6% of the adult population2,3. Flatfoot affects 25–49% of teenagers and 11.7–39.5% of athletes in China, with its true incidence rate significantly surpassing the statistics reported in the relevant literature4. The condition can occur unilaterally or bilaterally5 and may be symptomatic or asymptomatic6. Individuals with flatfoot have been shown to have lower balance scores during quiet standing7 and compared to those with a normal MLA, individuals with a flattened MLA have a higher incidence of lower extremity discomfort and injuries8,9.
In the treatment of flat foot, clinical practice often relies on foot orthoses10, kinesio tape11 or non-steroidal anti-inflammatory drugs12. And surgical correction was recommended in presence of grade 3 and 4 symptomatic flexible flatfoot, defined by clinical and radio graphic evaluation13. For flexible flatfoot, research suggests that targeted scientific exercise interventions can effectively improve their medial arch height and lower limb function14,15.
Different types of exercise, including short foot exercise (SFE)16, towel curling exercise (TCE)17, tibialis posterior strengthening exercise18, gluteus training14 and proprioceptive training19 are used in clinical practice. However, there is currently no evidence to indicate which exercise therapy is more effective for treating flexible flatfoot. Together with the patient, clinicians are therefore required to choose the type of exercise they prefer or expect to most effectively improve clinical outcomes.
As different types of exercise were often incorporated in different study interventions, it becomes difficult to draw conclusions regarding the efficacy of different types of exercise. Investigating the efficacy of these exercise interventions in separate pairwise meta-analyses is not possible, as insufficient data are available to address each type of exercise. In order to investigate the relative efficacy of different exercise interventions, network meta-analysis (NMA)20,21 enables the interpretation of an entire body of evidence, even though some interventions may not have been directly compared with others22,23. By generating a hierarchy of interventions, these NMAs are able to provide valuable information for clinical decision-making. Existing meta-analyses have provided evidence for exercise therapy versus ‘no treatment’24 and exercise therapy versus ‘foot orthoses’10, whereas NMA can add valuable information by combining evidence from both direct and indirect comparisons.
The primary research question was: What is the efficacy of different exercise interventions on arch shape of foot and the function of foot? Therefore, this work aimed to provide a systematic review and network meta-analysis (NMA) of randomised controlled trials (RCTs) on the efficacy of different types of exercise interventions in adults with flexible flatfoot.
Methods
Protocol and registration
This network meta-analysis was reported according to Preferred Reporting Items for Systematic Reviews and Meta- Analyses (PRISMA) statement and PRISMA extension for NMA (PRISMA-NMA)25,26. This study was prospectively registered on PROSPERO (CRD42024429607).
Information sources
Nine databases (PubMed, EMBASE, Web of Science, the Cochrane Central Register of Controlled Trials (CENTRAL), SCOPUS, PRDro, Google Scholar, China National Knowledge Infrastructure(CNKI) and Wanfang data) were systematically searched from their inception until February 2024.
Search strategy
A comprehensive electronic database search strategy was constructed to identify RCTs reporting the effects of an exercise intervention for adult flexible flatfoot using a combination of relevant medical subject heading (MeSH) terms and text words. It includes terms for (1) exercise, (2) flexible flatfoot and (3) RCTs. Initially the search strategy was developed for the Pubmed database, subsequently we adjusted this strategy for other databases. Separately, the reference lists of previous systematic reviews and meta-analyses were hand searched for additional studies not identified in the initial search.
Eligibility criteria
We included RCTs describing the effects of any exercise intervention in adults (age ≥ 18 years) with flexible flatfoot. Subjects were adults diagnosed with flexible flatfoot, adult acquired flatfoot deformity stage I-II or posterior tibial tendon dysfunction stage I-II with clear clinical signs. For comparator, we included any exercise intervention, or a control group, sham group, placebo group or no-treatment group. We excluded studies if they included participants younger than 18 years, participants with a history of lower limb trauma or participants with specific pathology (eg, cancer). Full-text papers published in the English language were included, and articles published from 1990 to February 2024 were encompassed. The detailed search strategy is provided in the Appendix.
Study selection
Following the systematic search, two reviewers (YJ and XS) independently screened all papers for eligibility. Studies were initially screened by title and abstract, and subsequently by full text if they met the predetermined inclusion criteria. In either stage, a third reviewer (EZ) resolved any disagreements on study inclusion as necessary. Where studies were reported in multiple papers, only the paper reporting the most complete analysis of efficacy was included (ie, reports of subgroups or secondary analyses were discarded).
Data extraction
Two reviewers extracted and recorded data from the included studies using a standardised extraction table agreed on by all authors. Extracted data comprised: study characteristics (author and year), participant characteristics (sample size, age and sex), type of exercise intervention, duration, frequency and intensity, outcome measures and timing of follow-up assessment. Means and SDs for primary outcome measures at baseline, postintervention and change data of them were extracted. As required for NMAs, we acquired mean change scores from the baseline and postintervention values. Following the recommendations from the Cochrane Handbook for Systematic Reviews of Interventions (Chapter 6)27, we aimed to calculate the change data. When studies did not report any change data, mean and SD of change were calculated using a correlation coefficient (\({\text{Corr}}_{{\text{E}}}\)) as previously tested and validated in a similar dataset36. \({\text{Corr}}_{{\text{E}}}\)=0.55 (ND)\(,{\text{ Corr}}_{{\text{E}}}\)=0.85 (FPI), \({\text{Corr}}_{{\text{E}}} = 0.45{}{\text{FFI}}{}\).Where studies reported more than two physical exercise interventions which could be independently included in this NMA, data from all study arms were extracted.
Primary outcomes
The primary outcome measures were navicular drop (ND), foot posture index (FPI), and foot function index (FFI).
Risk of bias assessment
Methodological quality of the included RCTs was assessed independently by two reviewers (YJ and XS) using the Cochrane risk of bias tool 228 in the following domains: (1) random sequence generation, (2) allocation concealment, (3) blinding of participants and personnel, (4) blinding of outcome assessors, (5) incomplete outcome data, (6) selective reporting, and (7) other biases. Each domain was evaluated as having a high risk of bias, an uncertain risk of bias, or a low risk of bias. Disagreements were resolved through discussion between the two reviewers, and if no consensus was reached, a third reviewer was consulted for final decision-making.
Methods of analysis
The characteristics of the included trials (details of the exercise intervention, outcomes) were summarised and tabulated.
NMA was used to compare the effectiveness of interventions that had and had not been evaluated directly against each other29,30. A frequentist approach to the NMA was used31. Network geometry was illustrated using network maps with the size of the nodes being proportional to the number of studies evaluating each class of intervention32. For each outcome, MDs and 95% confidence intervals were calculated, with P < 0.05 indicating statistical significance. Heterogeneity was assessed using I2, where I2 < 50% indicated low heterogeneity and a common-effect model was used; while I2 > 50% indicated high heterogeneity and a random-effects model was used33. Additionally, by examining the area under the cumulative probability curve, we can rank the interventions, with a higher surface under the cumulative ranking curve (SUCRA) value indicating a more effective intervention34. RStudio 1.4.1106 was used for all statistical analyses. The ‘gemtc’ R-package was used to conduct the NMA.
Results
Study selection
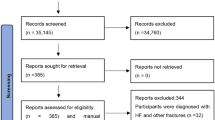
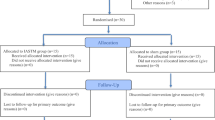
Figure 1 shows the PRISMA systematic review flow chart. A total of 2112 trials were identified in the initial systematic search. Records were excluded based on the included participants (not adult flexible flatfoot), the intervention or comparator (not a physical exercise intervention) or the study design (not an RCT). After exclusions, eleven RCTs were ultimately included in this network meta-analysis.

Flow of studies through the review. RCT, randomised controlled trial.
Risk of bias assessment
The quality assessment of the selected studies was conducted using the Cochrane risk of bias tool 2, and the assessment results are shown in Fig. 2. Ten studies were two-arm studies, with one being a three-arm study, all involving descriptions of randomization. Among them, nine studies described in detail the methods of generating random sequences. Due to the nature of exercise interventions, blinding was not implemented in most experiments, with only a few experiments using a single-blinding design. The majority of experiments reported in detail the data missing during the experimental process, with 1 studies not specifying the specific reasons for participant loss during the experiment, thus being judged as some concerns risk of bias.

Quality assessment of included studies.
Study characteristics
This study covers 11 studies, including a total of 335 participants. All participants were randomly assigned to the experimental group and control group. The experimental group included twelve different exercise therapies (short foot exercise (SFE), towel curling exercise (TCE), posterior tibial training + TCE, non-biomechanical function (NBF) exercise, proprioceptive neuromuscular facilitation (PNF), SFE with EMG biofeedback, hip-focused neuromuscular exercise, TCE + SFE, gluteus muscle strengthening, internal foot muscle training combined with posterior tibial muscle strengthening, comprehensive reinforcement, orthoses wear + stretching + concentric progressive resistive exercise of tibialis posterior, orthoses wear + stretching + and eccentric progressive resistive exercise of tibialis posterior). The duration of each intervention ranged from 10 to 40 min, the frequency ranged from once a week to seven times a week, and the duration of each study ranged from 3 days to 12 weeks. The control group received interventions such as routine daily activities, non-biomechanical function exercise, and routine care.
Study characteristics for all 11 included studies are presented in Table 1. Navicular drop (ND) was reported in 8 studies. Foot posture index (FPI) was reported in 2 studies. Foot function index (FFI) was reported in 2 studies.
Three networks of pairwise comparisons were constructed, one for navicular drop (ND) (8 RCTs, n = 297 participants/410 samples), and one for foot posture index (FPI) (2 RCTs, n = 56 participants) and one for foot function index (FFI) (2 RCTs, n = 75 participants), and direct and indirect evidence was obtained.
The following sections (ie, presentation of network structure, summary of network geometry, synthesis of results) are reported separately for each of the three networks (ie, navicular drop, foot posture index and foot function index).
Navicular drop
Eight studies were included in the NMA for navicular drop (Fig. 3), including a total of 297 participants with flexible flatfoot. Three network plots were formed, so the final results were reported according to each of them.

Network constructed for navicular drop. A, control group; B, short foot exercise(SFE); C, towel curling exercise (TCE); D, posterior tibial training + TCE; E, non-biomechanical function exercise; F, PNF; G, SFE with EMG biofeedback; H, hip-focused neuromuscular exercise; I, TCE + SFE; J, gluteus muscle strengthening; K, internal foot muscle training combined with posterior tibial muscle strengthening.
NMA1: We used the consistency model to compare different interventions with the I2 = 10%. The specific results are shown in Table 2. Compared with the control group, Strengthening the posterior tibial muscle + stretching the iliopsoas muscle + TCE (MD: 3.32, 95% CI 1.78, 4.89), PNF (MD: 1.81, 95%CI − 0.05, 3.70), SFE (MD: 1.23, 95%CI 1.02, 1.44) all showed better effects. In the probability ranking table in Fig. 4, Strengthening the posterior tibial muscle + stretching the iliopsoas muscle + TCE exercise is considered to be the most effective intervention, with SUCRA of 0.97, followed by PNF (0.70). Therefore, according to this ranking, the intervention effects of the four exercises are as follows: Strengthening the posterior tibial muscle + stretching the iliopsoas muscle + TCE > PNF > SFE > TCE > control group (NBF).

Rank of interventions for navicular drop network1. B, SFE; C, TCE; D, posterior tibial training + TCE; E, non-biomechanical function exercise; F: PNF.
NMA2: We used the consistency model to compare different interventions with the I2 = 25%. The specific results are shown in Table 3. Compared with the control group, hip-focused neuromuscular exercise (MD: 6.22, 95% CI − 1.69, 14.12), SFE with EMG biofeedback (MD: − 0.81, 95%CI − 1.59, 3.21) all showed better effects. In the probability ranking table in Fig. 5, hip-focused neuromuscular exercise is considered to be the most effective intervention, with SUCRA of 0.92, followed by SFE with EMG biofeedback (0.42). Therefore, according to this ranking, the intervention effects of the two exercises are as follows: hip-focused neuromuscular exercise > SFE with EMG biofeedback > control group.

Rank of interventions for navicular drop network2. A, control group; G, SFE with EMG biofeedback; H, hip-focused neuromuscular exercise.
NMA3: We used the consistency model to compare different interventions with the I2 = 26%. The specific results are shown in Table 4. In the probability ranking table in Fig. 6, internal foot muscle training combined with gluteus muscle strengthening is significantly better than the other two groups, with SUCRA of 0.99. Therefore, according to this ranking, the intervention effects of the three exercises are as follows: internal foot muscle training combined with gluteus muscle strengthening > internal foot muscle training combined with posterior tibial muscle strengthening > TCE + SFE.

Rank of interventions for navicular drop network3. I, TCE + SFE; J, gluteus muscle strengthening; K: internal foot muscle training combined with posterior tibial muscle strengthening.
Foot posture index
Two studies were included in the NMA for foot posture index (Fig. 7), including a total of 56 participants with flexible flatfoot.

Network constructed for foot posture index. A, control group; G, SFE with EMG biofeedback; O, comprehensive reinforcement.
We used the consistency model to compare different interventions with the I2 = 25%. The specific results are shown in Table 5. Compared with the control group, comprehensive reinforcement (MD: 1.95, 95% CI − 0.19, 4.03) showed better effects. In the probability ranking table in Fig. 8, comprehensive reinforcement is significantly better than the other two groups, with SUCRA of 0.98.

Rank of interventions for foot posture index. A, control group; G, SFE with EMG biofeedback; O, comprehensive reinforcement.
Foot function index
Two studies were included in the NMA for foot function index (Fig. 9), including a total of 75 participants with flexible flatfoot.

Network constructed for foot function index. L, orthoses wear and stretching; M, orthoses wear + stretching + concentric progressive resistive exercise of tibialis posterior; N, orthoses wear + stretching + and eccentric progressive resistive exercise of tibialis posterior.
We used the consistency model to compare different interventions with the I2 = 0.2%. The specific results are shown in Table 6. In the probability ranking table in Fig. 10, orthoses wear + stretching + eccentric progressive resistive exercise of tibialis posterior is significantly better than the other two groups, with SUCRA of 0.92.

Rank of interventions for foot function index. L, orthoses wear and stretching; M, orthoses wear + stretching + concentric progressive resistive exercise of tibialis posterior; N, orthoses wear + stretching + and eccentric progressive resistive exercise of tibialis posterior.
Discussion
This is the first study using NMA to investigate the comparative effectiveness of different exercise interventions for adults with flexible flatfoot. This study aimed to objectively evaluate the efficacy of exercise interventions on the arch shape of foot and the function of foot of the adults with flexible flatfoot, using network meta-analysis and probability ranking of the 11 clinical studies included.
The arch shape of foot
The study results indicated that hip muscle strengthening training was the most effective intervention for the navicular drop, followed by PNF technique and foot intrinsic muscle training. Both hip muscle strengthening training and PNF involved improving the stability of the lumbo-pelvic-hip complex, which may be related to the presence of lower limb movement pattern abnormalities in flatfoot patients.
The impact of collapsed arches could trigger a chain reaction of issues along the kinetic chain, including heel eversion, tibial internal rotation, knee valgus, femoral internal rotation, hip joint internal rotation and adduction, leading to pelvic anterior tilt, lumbo-pelvic-hip complex instability, muscle imbalances, joint dysfunction, and high injury risk. Kulig et al.’s research43 highlighted lower plantar flexor strength, bilateral hip extension, and hip abduction endurance deficits in females with posterior tibial tendon dysfunction compared to age-matched controls. Alahmri et al.44 reported that males with flexible flatfoot may experience hip abductor muscle fatigue, indicating compromised hip muscle function alongside foot and ankle issues. Meanwhile, Turgut et al.39 indicated that flatfoot in healthy individuals were due to weakness in the gluteal muscles (gluteus maximus, medius, and minimus), which leaded to hip internal rotation causing forefoot pronation. This may have explained why gluteal muscle training could have improved symptoms of flexible flatfoot. The kinetic chain theory underscored the interconnectedness of the body, where the function of one joint or muscle could impact adjacent structures45. Therefore, reactivating the gluteal muscles, knee flexors, and knee extensors could have established proper muscle recruitment patterns and strengthened the lower limb kinetic chain, potentially benefiting individuals with flexible flatfoot.
What we can confirm is that there is a certain correlation between the hip muscle state and the arch collapse in patients with flexible flatfoot. However, due to limited research evidence, we are unable to determine the underlying relationship between these two factors. Hence, it should be noted that the the original studies did not pay much attention to this point, which may lead to limitations in the applicability of the results. There still need more sample size to support this viewpoint in the future.
In terms of the foot posture index, our NMA suggested that comprehensive foot strengthening training was more effective than using electrical stimulation to strengthen the intrinsic foot muscles, which differed from our previous understanding. This implied that training the ankle joint function and overall foot muscle strength may have been more advantageous for supporting and stabilizing the normal foot structure than solely focusing on the intrinsic foot muscles and their proprioception. Sustaining a normal arch necessitated the involvement of both intrinsic and extrinsic foot muscles46. The posterior tibial muscle acted as the primary dynamic stabilizing structure, followed by the flexor digitorum longus, flexor hallucis longus, fibularis longus, and the triceps surae. Additionally, the abductor hallucis, flexor digitorum brevis, and plantar muscles, along with other intrinsic foot muscles, contributed to rapidly restoring local stability through proprioceptors in the foot sole47. During standing and walking, these muscles collectively maintained the arch shape, cooperated, and actively engaged in regulating energy absorption and release in the foot during the walking process48. Hence, emphasizing comprehensive foot functional training could offer a novel approach to enhancing the foot posture of adults with flexible flatfoot. Nonetheless, further high-quality randomized controlled trials and clinical practice are required to delve deeper into and refine the optimal approach for comprehensive foot strengthening training.
The function of foot
The priority was given to eccentric progressive resistive exercise of tibialis posterior. This preference could have been attributed to the significant influence eccentric training has on reshaping degenerated tendons. Presently, eccentric training was extensively researched in managing achilles tendonitis and patellar tendonitis, given the specific pathological alterations in the posterior tibial muscle tendon of individuals with flexible flatfoot. Similar to the treatment of achilles and patellar tendons, eccentric contraction therapy offered two credible explanations for chronic tendon pathologies49,50. The first theory was the normalization theory of tendon structure, suggesting that eccentric contractions can enhance collagen type I, thereby enhancing the muscle tissue structure51. The second compelling theory was the force fluctuation theory, which proposed that the force fluctuations resulting from eccentric contractions stimulate muscle remodeling, effectively addressing tendon pathologies52. Nevertheless, several fundamental aspects concerning the optimal approach to eccentric contraction therapy remained unresolved, including contraction angle, movement speed, repetition count, treatment duration, and more53. These aspects necessitate further comprehensive exploration and resolution in future research. In conclusion, limited studies have detailed the specific conditions and manifestations of the “weak link” in the lower limbs of individuals with flexible flatfoot, and the effects of eccentric training of the posterior tibial muscle on such conditions. The lack of guiding evidence for clinical application underscores the necessity for additional foundational theoretical research and clinical practice reports to expound further on its scientific validity, effectiveness, and practicality.
The duration and frequency of exercise protocols
The duration and frequency of exercise protocols varies depending on different studies. A small portion of the studies chose 4–6 weeks, while the majority chose 8–12 weeks. And most of them choose to exercise 3 days or more a week. For exercise therapy, the duration of exercise intervention is crucial because the effects of exercise require a certain amount of time to accumulate and exert. Although there is currently no research comparing exercise duration, for this article, we believe that exercise therapy for patients with flexible flatfoot also follows this principle. Therefore, we recommend using an exercise regimen of at least 6 weeks, 3 times a week or more, because most exercise therapies can be completed at home after learning the correct skills.
Therefore, this NMA suggested that the improvement of arch shape and foot function in patients with flexible flatfoot could be not only limited to the exercise of the intrinsic muscles of the foot and the muscles around the ankle, but also more focused on the overall and comprehensive adjustment of the lower limb motion chain. The training should be extended to the muscles around the hip and knee, with the focus on correcting the lower limb force line, thereby alleviating muscle bone pain caused by arch collapse.
Limitations
Due to the limited clinical research in this field, the network formed by this NMA remained relatively scattered, resulting in imprecise research findings. And the quality of evidence seemed to be mainly constrained by small sample sizes and limited studies for certain comparisons. However, this was an unavoidable consequence, and we have included all eligible RCTs to obtain the most reliable conclusions possible at this stage.
An inherent limitation of NMA was deriving indirect evidence from a limited number of direct pairwise comparisons. In the current study, this was apparent from the plots for NMAs, demonstrating uncertainty in the point measure as well as large CIs for many of the exercise interventions.
We could not provide guidance on the dose–response relationship between exercise therapy and treatment effectiveness because insufficient data were available within separate nodes to allow for an investigation of the differential effects of different exercise durations, intensities, and frequencies. Therefore, it appeared to be more beneficial to have conducted well-designed, large trials investigating the comparative effectiveness of different types of physical exercise for people with flexible flatfoot.
Conclusion
Various exercise therapy could improve the arch shape and function of flexible flatfoot patients, particularly hip muscle and lower limb overall muscle training. Current evidence suggested that strengthening the posterior tibial and plantar muscles combined with gluteus muscle strengthening, neuromuscular movements centered around the buttocks, and lower limb proprioceptive neuromuscular facilitation (PNF) techniques were effective in improving the arch shape of flexible flatfoot patients, while posterior tibial muscle centrifugal training was effective in improving foot function. These novel findings may assist clinicians to choose an appropriate exercise intervention for individuals with flexible flatfoot.
Data availability
The authors confirm that the data supporting the findings of this study are available within the article.
References
Desmyttere, G., Hajizadeh, M., Bleau, J. & Begon, M. Effect of foot orthosis design on lower limb joint kinematics and kinetics during walking in flexible pes planovalgus: A systematic review and meta-analysis. Clin. Biomech. 59, 117–129 (2018).
Aenumulapalli, A., Kulkarni, M. M. & Gandotra, A. R. Prevalence of flexible flat foot in adults: A cross-sectional study. J. Clin. Diagn. Res. 11(6), 17 (2017).
Pita-Fernandez, S. et al. Flat foot in a random population and its impact on quality of life and functionality. J. Clin. Diagn. Res. 11(4), LC22 (2017).
Li, H., Zhang, H., Zhang, H., Gai, D. & Qi, W. Study on detection methods and progress of flatfoot. CHSM. 9(09), 34–37 (2018).
Arachchige, S. N. K., Chander, H. & Knight, A. Flatfeet: Biomechanical implications, assessment and management. The Foot. 38, 81–85 (2019).
Tareco, J. M., Miller, N. H., MacWilliams, B. A. & Michelson, J. D. Defining flatfoot. Foot Ankle Int. 20(7), 456–460 (1999).
Tahmasebi, R., Karimi, M. T., Satvati, B. & Fatoye, F. Evaluation of standing stability in individuals with flatfeet. Foot Ankle Spec. 8(3), 168–174 (2015).
Açak, M. The effects of individually designed insoles on pes planus treatment. Sci. Rep.-Uk 10(1), 19715 (2020).
Riskowski, J. L. et al. Associations of foot posture and function to lower extremity pain: Results from a population-based foot study. Arthrit. Care Res. 65(11), 1804–1812 (2013).
Oerlemans, L. N. T. et al. Foot orthoses for flexible flatfeet in children and adults: A systematic review and meta-analysis of patient-reported outcomes. Bmc Musculoskel. Dis. 24(1), 16 (2023).
Siu, W. S., Shih, Y. F. & Lin, H. C. Effects of Kinesio tape on supporting medial foot arch in runners with functional flatfoot: A preliminary study. Res. Sports Med. 28(2), 168–180 (2020).
Dibello, D., Dallan, G., Di Carlo, V. & Pederiva, F. Quality of life in flexible painful flatfoot treated by anterograde calcaneo-stop procedure: The patient’s and family’s perspective. Plos one. 18(2), e0263763 (2023).
Biz, C. et al. Flatfoot over the centuries: The background of current conservative and operative treatments. Int. Orthop. 47(9), 2357–2368 (2023).
Engkananuwat, P. & Kanlayanaphotporn, R. Gluteus medius muscle strengthening exercise effects on medial longitudinal arch height in individuals with flexible flatfoot: A randomized controlled trial. J. Exerc. Rehabil. 19(1), 57 (2023).
Brijwasi, T. & Borkar, P. A comprehensive exercise program improves foot alignment in people with flexible flat foot: A randomised trial. J. Physiother. 69(1), 42–46 (2023).
Utsahachant, N., Sakulsriprasert, P., Sinsurin, K., Jensen, M. P. & Sungkue, S. Effects of short foot exercise combined with lower extremity training on dynamic foot function in individuals with flexible flatfoot: A randomized controlled trial. Gait Posture. 104, 109–115 (2023).
Chung, K. A., Lee, E. & Lee, S. The effect of intrinsic foot muscle training on medial longitudinal arch and ankle stability in patients with chronic ankle sprain accompanied by foot pronation. Phys. Ther. Rehabil. Sci. 5(2), 78–83 (2016).
Lee, D. & Choi, J. The effects of foot intrinsic muscle and tibialis posterior strengthening exercise on plantar pressure and dynamic balance in adults flexible pes planus. Phys. Ther. Korea. 23(4), 27–37 (2016).
Park, D. J., Lee, K. S. & Park, S. Y. Effects of two foot-ankle interventions on foot structure, function, and balance ability in obese people with pes planus. Healthcare Basel. 9(6), 667 (2021).
Cipriani, A., Higgins, J. P., Geddes, J. R. & Salanti, G. Conceptual and technical challenges in network meta-analysis. Ann. Intern. Med. 159(2), 130–137 (2013).
Li, T. et al. Network meta-analysis-highly attractive but more methodological research is needed. BMC Med. 2011, 9 (2011).
Mavridis, D., Giannatsi, M., Cipriani, A. & Salanti, G. A primer on network meta-analysis with emphasis on mental health. Evid. Based Ment Health. 18, 40–46 (2015).
Rouse, B., Chaimani, A. & Li, T. Network meta-analysis: An introduction for clinicians. Intern. Emerg. Med. 12(1), 103–111 (2017).
Feng, L., Gong, S. & Huo, H. Effect of short-foot training on foot and ankle function in patients with flat feet: Meta-analysis and systematic review. Chin. J. Tissue Eng. Res. 27(5), 799 (2023).
Hutton, B. et al. The PRISMA extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: checklist and explanations. Ann. Intern. Med. 162, 777–784 (2015).
Moher, D., Liberati, A., Tetzlaff, J., Altman, D. G., PRISMA Group*, T. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 6, e1000097–e1000106 (2009).
Higgins, J. P. T., Li, T. & Deeks, J. J. Choosing effect measures and computing estimates of effect. Cochrane Handb. Syst. Rev. Intervent. 2019, 143–176 (2019).
Sterne, J. A. C. et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 366, l4898 (2019).
Mills, E. J., Thorlund, K. & Ioannidis, J. P. A. Demystifying trial networks and network meta-analysis. BMJ 346, f2914 (2013).
De Zoete, R. M., Armfield, N. R., McAuley, J. H., Chen, K. & Sterling, M. Comparative effectiveness of physical exercise interventions for chronic non-specific neck pain: A systematic review with network meta-analysis of 40 randomised controlled trials. Br. J. Sports Med. 55(13), 730–742 (2021).
Edwards, J. J. et al. Exercise training and resting blood pressure: a large-scale pairwise and network meta-analysis of randomised controlled trials. Br. J. Sports Med. 57(20), 1317–1326 (2023).
White, I. R. Network meta-analysis. Stata J. 15, 951–985 (2015).
Tanriver-Ayder, E., Faes, C., Van De Casteele, T., McCann, S. K. & Macleod, M. R. Comparison of commonly used methods in random effects meta-analysis: Application to preclinical data in drug discovery research. BMJ Open Sci. 5, 1 (2021).
Nevill, C. R., Cooper, N. J. & Sutton, A. J. A multifaceted graphical display, including treatment ranking, was developed to aid interpretation of network meta-analysis. J. Clin. Epidemiol. 157, 83–91 (2023).
Okamura, K. et al. Effects of plantar intrinsic foot muscle strengthening exercise on static and dynamic foot kinematics: A pilot randomized controlled single-blind trial in individuals with pes planus. Gait Posture. 75, 40–45 (2020).
Pabón-Carrasco, M. et al. Randomized clinical trial: The effect of exercise of the intrinsic muscle on foot pronation. Int. J. Env. Res. Pub. He. 17(13), 4882 (2020).
Houck, J., Neville, C., Tome, J. & Flemister, A. Randomized controlled trial comparing orthosis augmented by either stretching or stretching and strengthening for stage II tibialis posterior tendon dysfunction. Foot Ankle Int. 36(9), 1006–1016 (2015).
Kulig, K. et al. Nonsurgical management of posterior tibial tendon dysfunction with orthoses and resistive exercise: A randomized controlled trial. Phys. Ther. 89(1), 26–37 (2009).
Turgut, E., Yagci, G. & Tunay, V. B. Hip-focused neuromuscular exercise provides immediate benefits in foot pronation and dynamic balance: A sham-controlled cross-over study. J. Sport Rehabil. 30(7), 1088–1093 (2021).
Alam, F. et al. Effects of selective strengthening of tibialis posterior and stretching of iliopsoas on navicular drop, dynamic balance, and lower limb muscle activity in pronated feet: A randomized clinical trial. Phys. Sportsmed. 47(3), 301–311 (2019).
Mulchandani, P., Warude, T. & Pawar, A. Effectiveness of gluteal muscle strengthening on flat foot. Asian J. Pharm. Clin. Res. 10(6), 219–221 (2017).
Sánchez-Rodríguez, R. et al. Modification of pronated foot posture after a program of therapeutic exercises. Int. J. Env. Res. Pub. He. 17(22), 8406 (2020).
Kulig, K., Popovich, J. M. Jr., Noceti-Dewit, L. M., Reischl, S. F. & Kim, D. Women with posterior tibial tendon dysfunction have diminished ankle and hip muscle performance. J. Orthop. Sports Phys. Ther. 41(9), 687–694 (2011).
Alahmri, F., Alsaadi, S., Ahsan, M. & Almousa, S. The effect of isokinetic hip muscle strength on normal medial longitudinal arch feet and pes planus. J. Med. Life. 15, 9 (2022).
Izraelski, J. Assessment and treatment of muscle imbalance: The Janda approach. J. Can. Chiropr. Assoc. 56(2), 158 (2012).
Flores, D. V., Mejía-Gómez, C., Fernández-Hernando, M., Davis, M. A. & Pathria, M. N. Adult acquired flatfoot deformity: Anatomy, biomechanics, staging, and imaging findings. Radiographics 39(5), 1437–1460 (2019).
McKeon, P. O., Hertel, J., Bramble, D. & Davis, I. The foot core system: A new paradigm for understanding intrinsic foot muscle function. Br. J. Sports Med. 49(5), 290–290 (2015).
Giza, E., Cush, G. & Schon, L. C. The flexible flatfoot in the adult. Foot Ankle Clin. 12(2), 251–271 (2007).
Öhberg, L., Lorentzon, R. & Alfredson, H. Eccentric training in patients with chronic Achilles tendinosis: normalised tendon structure and decreased thickness at follow up. Br. J. Sport Med. 38(1), 8–11 (2004).
Challoumas, D. et al. Management of patellar tendinopathy: A systematic review and network meta-analysis of randomised studies. BMJ Open Sport Exerc. Med. 7, e001110 (2021).
Langberg, H. et al. Eccentric rehabilitation exercise increases peritendinous type I collagen synthesis in humans with Achilles tendinosis. Scand. J. Med. Sci. Sport. 17(1), 61–66 (2007).
Rees, J. D., Wolman, R. L. & Wilson, A. Eccentric exercises; why do they work, what are the problems and how can we improve them?. Br. J. Sport Med. 43(4), 242–246 (2009).
Alfredson, H., Pietilä, T., Jonsson, P. & Lorentzon, R. Heavy-load eccentric calf muscle training for the treatment of chronic Achilles tendinosis. Am. J. Sports Med. 26(3), 360–366 (1998).
Acknowledgements
We thank all the reviewers and for their assistance and support.
Funding
No sources of funding were used to assist in the preparation of this article.
Author information
Authors and Affiliations
Contributions
Study concept and design: Y.J., and X.S.; Search of databases and screening of articles: Y.J., and X.S; Data extraction and quality assessment of articles: Y.J., and X.S, and E.Z.; Data synthesis and analysis: Y.J., and X.S.; Initial drafting of the manuscript: Y.J.; Revision of the drafted manuscript and supervision:E.Z.; Final review of the manuscript: Y.J, X.S, and E.Z. All authors have read and agreed to the published version of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Jia, Y., Sai, X. & Zhang, E. Comparing the efficacy of exercise therapy on adult flexible flatfoot individuals through a network meta-analysis of randomized controlled trials. Sci Rep 14, 21186 (2024). https://doi.org/10.1038/s41598-024-72149-w
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-024-72149-w
