
Abstract
The rapid epidemiological transition in Asian countries, resulting from the rising trend of urbanisation and lifestyle changes, is associated with an increasing risk of obesity in women of reproductive age. This is the first study to investigate the trends and population-attributable fraction (PAF) of obesity, and the interaction effects of education and wealth on obesity among reproductive-age women aged 15–49 years in ten Asian countries. This cross-sectional study examined the most recent (2000 to 2022) Demographic and Health Surveys (DHS) data from ten Central and Southeast Asian countries. Multilevel multinomial logistic regression models were used to compute odds ratios (ORs). PAFs adjusted for communality were calculated using adjusted ORs and prevalence estimates for each risk factor. This study included a weighted sample of 743,494 reproductive-age women. All the countries showed an increasing trend for obesity and a decreasing trend for underweight, except for the Maldives. The highest PAFs of obesity were associated with women who were married (PAF = 22.2%; 95% CI 22.1, 22.4), aged 35–49 years (PAF = 16.4%; 95% CI 15.5, 17.1), resided in wealthy households (PAF = 14.5%; 95% CI 14.4, 14.5), watched television regularly (PAF = 12.5%; 95% CI 12.1, 12.8), and lived in urban areas (PAF = 7.8%; 95% CI 7.7, 8.0). The combined PAF showed that these five risk factors were associated with 73.3% (95% CI 71.8, 74.9) of obesity among reproductive-age women. Interaction analysis between women’s education and household wealth revealed that having a secondary or higher level of education and residing in a wealthier household was associated with a lower risk of obesity (OR = 0.71, 95% CI 0.66, 0.76). The findings of this study suggest that, in order to address the rising rate of obesity among women in Asian countries, education and lifestyle modifications in urban areas should be a priority. Pakistan and the Maldives need to be a priority given the rapidly increasing trends in obesity and underweight subpopulations in their respective countries.
Similar content being viewed by others

Background
Globally, approximately one-third of adults are overweight or obese, while around one in ten are underweight, with rates varying substantially across regions and countries1. The World Obesity Federation (WOF) predicts that by 2030, roughly one billion people worldwide will be living with obesity, including one in five women and one in seven men2. Estimates indicate a significant increase in the proportion of overweight and obese women in most low- and middle-income countries (LMICs). This increase is attributed to ongoing demographic and societal changes, including rising rural-to-urban migration, which lead to greater exposure to sedentary lifestyles, processed foods, and reduced access to traditional diets and physical activity1,2. The rising burden of obesity in women represents an enormous challenge with respect to non-communicable diseases (NCDs), increased healthcare costs, potential detrimental impacts on maternal and child health, reduced workforce productivity, and social and psychological implications3,4.
There is a tendency for an increasing prevalence of obesity among women in low-income populations with rapidly developing economies (e.g., China5 and Thailand6), and among the wealthier segments of society in slower developing economies (e.g., Bangladesh, Tanzania)7. Most LMICs in Southeast and Central Asia are currently in the mid-stages of economic development with a large segment of the population shifting towards less nutritious but more affordable foods and sedentary lifestyles8,9. Consequently, alongside pre-existing issues of malnutrition, there is a growing prevalence of overweight and obesity in specific sub-populations of women across the region8,9,10. This trend is an enormous challenge for local economies and fragile healthcare systems9,11. On regional and national levels, the dual challenges of malnutrition and obesity have created a dilemma, forcing policymakers to decide which issue to address first given the constraints of limited resources.
The epidemiological and nutrition transition may not solely attributed to economic development, but may also involve other demographic and societal changes, including rural-to-urban migration12,13,14. Asian countries appear to be following this trend, with a projected urbanization rate of 1.3% by 203013,14. Around 40% of the urban population in Asia resides in mega cities, each with a population of over one million (e.g., Dhaka, Mumbai, Kolkata, Karachi, and Delhi). The population in Asian megacities is growing with a rate of > 2% per year, which also contributes to approximately 35% of the total population living in chronic poverty in urban slums14.
While increasing urbanization and commercialization may expose individuals and families to unhealthy diet and lifestyles, better education and higher income at the individual level should have an interrelated, counteracting effect on obesity15. Nationally representative studies, especially from middle-income Asian countries including China and Thailand, have in fact noted the protective effect of education and household income on female obesity5,6. Highly educated women and those who belonged to richer households are likely to have greater access to health information, be more health conscious, and have more choices regarding diet and exercise than lower-educated women from poorer households16. The existing evidence on trends in obesity and the relationship between education, household income and obesity among reproductive-age women in Central and Southeast Asia are limited and not well understood.
Policymakers in public health across Asia should examine the population-attributable fraction (PAF) of key risk factors of obesity among reproductive-age women17. This evidence is crucial for developing policy to curb intergenerational transmission of obesity18. Moreover, investigating the interaction between the socio-economic determinants of health and women’s nutritional status is further pertinent for the development of tailored prevention strategies. This will ultimately contribute to achieving the United Nations’ Sustainable Development Goal (SDG) target 3.4, which aims to reduce premature mortality from NCDs by one third through prevention and early intervention by 2030. Therefore, this study investigated the trends and PAF of obesity, and the interaction effects of education and wealth on obesity among reproductive-age women in ten Asian countries.
Methods
Study design and data sources
This cross-sectional study analysed the most recent (2012–2022) population-based data sets from the Demographic and Health Surveys (DHS) conducted in eight Southeast Asian countries and two Central Asian countries (Table 1). These countries encompassed Bangladesh, Cambodia, India, Kyrgyzstan, Maldives, Myanmar, Nepal, Pakistan, Tajikistan, and Timor-Leste. The exclusion of other countries in the region is due to surveys being restricted, unavailable, or lacking information on women’s body mass index (BMI). For each country, we retrieved data from available DHS conducted between 2000 and 2022 to analyse the trends of obesity, overweight, and underweight over the 22-year period.
The DHS program is funded by the United States Agency for International Development (USAID) and is implemented by Inner City Fund (ICF) International19. The Monitoring and Evaluation to Assess and Use Results (MEASURE) from the DHS studies were carried out by the respective Ministries of Health or governmental agencies, with support from ICF International, at regular intervals. The survey design and data are consistent, as they are based on standardized data collection methods and survey tools. The DHS gathers data on the demographics and health of individuals, encompassing topics such as maternal and child health, mortality, nutrition, and the social determinants of health19.
Ethics
Ethical clearance was obtained for all DHS from the respective countries, whereas for this study, the requirement for informed consent was waived as publicly available data were used. This study followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guideline for cross-sectional studies.
Sampling procedures and sample size
The DHS uses a two-stage stratified cluster sampling technique to select the study participants. In the first stage, the first administrative units (e.g., States and Regions) were stratified into urban or rural strata, followed by the selection of Enumeration Areas (EAs) in proportion to the population size of each cluster. In each selected EA, a complete census of households was conducted. In stage two, a fixed number of households were selected using the list of households as a sampling frame. Further details about the sampling design and questionnaire can be found in the country-specific MEASURE DHS reports.
For this study, the DHS survey data from the selected countries were pooled. The data were collected from eligible women, which included all females between the ages of 15 and 49 years who either lived in the households permanently or were present on the night before the survey. Women who were pregnant, or who had given birth in the two months preceding the survey were excluded to minimize measurement bias due to initial weight gain from pregnancy and childbirth.
Outcome variables
We used the World Health Organization (WHO) BMI cut-offs of < 18.5, 25–29.9 and ≥ 30 kg/m2 to categorize underweight, overweight and obesity, respectively20. DHS used the SECA-874 digital scale to measure weight and the SECA-213 stadiometer to measure height. Trained survey staff obtained the measurements for a single time. BMI was rounded to the nearest hundredth decimal place.
Explanatory variables
We considered several demographic and socio-economic variables including household wealth index, marital status, educational level, women’s age, number of children, current contraceptive use, place of residence, reading magazines, and watching television. The selection of the variables was informed by previous studies and the availability of relevant data. 8–10 Smoking, alcohol consumption, and women’s employment status were excluded from the analysis, either because they were not measured for each country or because they had a higher number of missing values. Table 2 provides the definitions for these explanatory variables.
The household wealth index represents a combined measurement of a household’s overall living standards. It is a composite measure of relative economic status estimated using household-level information on asset ownership and access to services from individual questionnaires21. In DHS, the household wealth index was computed using principal component analysis (PCA), considering various aspects like the possession of household amenities such as toilets, electricity, television, radio, fridge, and bicycle, as well as the availability of a source of drinking water and the type of flooring material used in the main house22. Each asset’s importance is calculated using factor scores which are standardized to have a mean of zero and a standard deviation of one. Based on whether a household owns a particular asset, standardized scores are assigned and summed up. Individuals are then ranked according to their household’s total score.
Since the relative importance of different assets varies across countries, PCA is a data-driven approach that allows the wealth index to be tailored to each country’s specific socioeconomic context. However, DHS uses wealth quintiles rather than the raw PCA scores, which allow for a comparative analysis of how wealth is distributed, how it correlates with health or education outcomes, and how inequality varies across countries21.
Statistical analysis
The initial analyses involved calculating frequencies and percentages to provide an overview of the study population from the pooled data. To analyse the trends of obesity, overweight, and underweight, we calculated the prevalence, along with the corresponding 95% confidence intervals (CI), for each country from 2000 to 2022.
Multilevel multinomial logistic regression models were used in the pooled data to compute odds ratios (ORs) with 95% confidence intervals (CIs) for the risk factors for obesity, overweight and underweight (Model 1). Healthy weight groups were indicated as a reference category. The multi-level analysis was selected to account for the hierarchical structure of the data, where reproductive-age women [level I] were nested within clusters [level II]), consistent with previously published studies23,24. This approach enables accurate calculation of standard errors for regression coefficients and addresses the dependence of observations within the same clusters (i.e., women in the same cluster are likely to have more similar nutritional statuses than those in different clusters)25.
Upon identifying the key risk factors associated with obesity, overweight, and underweight, our analysis involved the computation of PAFs using Miettinen’s formula. The choice of Miettinen’s formula was based on its ability to produce reliable estimates, particularly in the presence of confounding, when adjusted ORs are used26. The PAF serves as a metric indicating the proportion of obesity among reproductive age women in Asian countries that could potentially be mitigated by addressing the identified potentially modifiable risk factors within the population27. PAF was calculated using the following formula:
where Pc is the prevalence of the modifiable risk factor among cases, and OR is the adjusted ORs of obesity, overweight, and underweight associated with the potentially modifiable risk factors26,27. Given the modifiable risk factors occur simultaneously within individuals, aggregating the PAF for each specific risk factor may lead to an overestimation of their combined effects28,29. Based on previously published studies, we employed communality weights to correct for the overlap of risk factors among participants30.
To calculate communalities, we initially computed the pairwise tetrachoric correlation among all potentially modifiable risk factors. Pairwise tetrachoric correlation is specifically designed for assessing the relationships between pairs of dichotomous variables (i.e., binary variables with two possible outcomes: ‘0/1’ or ‘yes/no’). In datasets with multiple binary variables, tetrachoric correlation is applied to each pair of variables separately. This pairwise approach is used to isolate the direct relationship between two variables without the influence of others31. Subsequently, a principal components analysis was conducted on the tetrachoric correlation matrix to extract a set of common factors that explain the relationships. The communality for each risk factor was determined by the sum of squares of the loadings in all principal components with an eigenvector greater than 1. The weighting of each risk factor was then carried out using the formula: We = 1 − communality. Following this, a combined PAF across the potentially modifiable risk factors was calculated using the specified formula:
Where ‘e’ represents each modifiable risk factor, and ‘We’ represents the communality weight of each risk factor. Finally, we estimated the adjusted PAF for each risk factor using the formula:
.
To test the interaction effect of women’s education and household wealth index on obesity, an interaction term of women’s education and household wealth index was included in the model, with education as a categorical variable (Supplementary Table 1). Multicollinearity was checked using ‘vif’ command and no significant results were evident. All statistical analyses were conducted using Stata version 18.0 (StataCorp, College Station, TX, USA) with ’svy’ command to adjust for effect of sampling and stratification, and the ’gsem’ function was used for multilevel multinomial models to account the effect of two stage sampling design in DHS survey data.
Results
Study participants
This study involved 743,494 reproductive-age women aged 15–49 years, with a mean age of 30.7 (± 9.9) years. Of the total women, 40.8% (303,280) resided in wealthy households, and 64.6% (480,588) attained secondary or higher level of education. A total of 71.2% (528,949) women were married, and 38.3% (284,493) were in the age group 35–49 years. A total of 63.4% (471,039) women had 1–4 children, and 51.1% (379,516) were using contraception methods. A total of 67.6% (502,311) women were from rural areas. About 33.5% (248,832) of women read magazines, while 73.5% (546,263) watched television (Table 3).
Trends in obesity
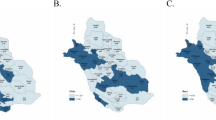
All ten South and Southeast Asian countries showed an upward trend in the obesity prevalence over the past two decades (Fig. 1). For example, in Pakistan, obesity increased from 17.3% in 2012 (95% CI: 15.2, 19.6) to 21.8% (95% CI: 19.6, 24.2) in 2018. A similar trend was observed in Maldives with obesity increasing from 13.9% (95% CI: 12.5, 15.4) in 2009 to 19.3% (95% CI: 18.1, 20.7) in 2016. All countries had a gradual increase in overweight and a gradual decrease in underweight prevalence, except for the Maldives. In Maldives, between 2009 and 2016, the prevalence of overweight decreased from 33.9% (95% CI: 32.1, 35.8) to 29.9% (95% CI: 28.4, 31.6), while the prevalence of underweight increased from 6.9% (95% CI: 5.9, 7.9) to 10.7% (95% CI: 9.7, 11.8).

Trends (2000–2022) in obesity, overweight and underweight status among reproductive-age women aged 15–49 years of age from ten countries in Asia.
Population attributable fractions for obesity
The highest PAFs of obesity were associated with married women (PAF = 22.2%; 95% CI: 22.1, 22.4), those aged 35–49 years (PAF = 16.4%; 95% CI: 15.5, 17.1), individuals who resided in rich households (PAF = 14.5%; 95% CI: 14.4, 14.5), women who watched television on a regular basis (PAF = 12.5%; 95% CI: 12.1, 12.8), and for those who were from urban areas (PAF = 7.8%; 95% CI: 7.7, 8.0) (Table 4). The combined PAF showed that these five risk factors were associated with 73.3% (95% CI: 71.8, 74.9) of obesity among reproductive-age women. Additionally, these same five risk factors were associated with 58.5% (95% CI: 58.1, 60.5) of them being overweight (Supplementary Table 2).
Interaction effect of women’s education and wealth on obesity
The interaction analysis between women’s education and household wealth index revealed that, in rich households, women who completed secondary or higher level of education had a lower risk of obesity (OR = 0.71, 95% CI: 0.66, 0.76) compared to those with no formal education (Supplementary Table 2, Model 2). In wealthy households, women who completed secondary or higher level of education exhibited a higher risk of underweight (OR = 1.52, 95% CI: 1.44, 1.61) compared to those with no formal education.
Discussion
This is the first study to investigate the trends and PAF of obesity, as well as the effects of education-wealth interaction on obesity among reproductive-age women in ten Asian countries. The findings from our study identified a rising trend in obesity. All the countries showed an increasing trend for overweight, and a decreasing trend for underweight, except for the Maldives. A total of 73.3% of obesity among reproductive age women was associated with five risk factors: being married, age ≥ 35 years, residing in wealthy households, regular television watching and living in urban areas.
The computation of PAFs for obesity provides an opportunity to guide resource distribution, particularly in countries, such as Pakistan and the Maldives, that are dealing with a substantial burden of obesity. The use of nationally representative DHS datasets further strengthens the applicability of our findings to the broader regional context. The risk factors investigated in this study hold broader implications for preventing obesity in women and improving women’s health and wellbeing. Programs promoting nutritional education and healthier lifestyles, prioritizing women in urban areas, particularly those residing in affluent households who engage in unhealthy eating habits and physical inactivity, are cost effective investments for Central and Southeast Asian countries32,33. It is estimated that for each 1 USD invested in preventing obesity, up to 5.6 USD will be returned in economic benefits33.
Obesity remains a significant challenge among wealthier segments of society, particularly within urban populations in Central and Southeast Asian countries7. The risk also tends to increase among women who are married, older, or frequently engage with media such as magazines or television. Addressing the obesity epidemic among Asian women of childbearing age requires a multifaceted approach. Interventions such as promoting healthier diets and reducing sedentary behaviours through public health campaigns, increasing access to affordable nutritious foods, and policies that regulate food advertising and promote physical activity in urban areas may help combat the growing obesity epidemic34. In some Asian cultures, women are often expected to prioritize caregiving and household responsibilities, which can limit their ability to access and engage in physical activity. Familial and peer support strategies are needed to help women overcome traditional gender roles and create an enabling environment that sustains their health-behaviour changes35.
The effect of interaction between education and household wealth on women’s obesity risk merits closer attention, as this has not been extensively discussed previously36,37. The education-obesity relationship is not uniform in all Asian societies due to the varying degree of progress in educational development, economic development, and globalization between the countries38,39. In addition to experiencing rapid economic growth, middle- to high-income Asian countries have introduced policies and initiatives aimed at improving women’s access to higher education, positioning education as a modifiable factor for obesity prevention within the broader socio-economic landscape40. However, policies and interventions for obesity prevention across LMICs in Asia have not prioritised long term measures, such as promoting women to complete secondary education41.
The positive associations between living in urban areas, household wealth, sedentary behaviours and obesity can still be counteracted with encouraging women to complete secondary level or higher education, as shown by the experience of middle to high income Asian countries5,6,39,42,43. Women with higher education have the ability to challenge pre-existing gender norms, and make informed health and behavioural choices with respect to nutritional choices and lifestyle changes44. The importance of women completing a higher education should be acknowledged not only for preventing obesity among women and improving gender equality and the health of the entire family but also for the future economic development of an entire nation.
Asian megacities, comprising 35% of the population living in slums, demand enhanced public services such as access to healthier foods and clean water, yet improvements in these crucial areas have unfortunately not kept pace with the rapid urbanization14. Consequently, a considerable segment of general women’s population as well as women from urban areas, for instance in Timor-Leste, India, Pakistan, and the Maldives, is malnourished and faces an increased risk of infectious diseases due to poorer water, hygiene, and sanitation conditions. To tackle the double burden of nutritional problems in women, especially in impoverished areas, poverty reduction measures (e.g., employment training and micro-financing), as well as encouragement of local food production and consumption can be instrumental (Supplementary Table 3)45.
Veblen’s 1899 hypothesis46 associating female desire for thinness with higher social classes seems to be not influenced by wealth alone but rather due to the interaction between higher education and household wealth in Asian countries. It is true that the beauty industry and social media, to which affluent and educated women have greater access, have perpetuated a social preference for thinness over plumpness as a feminine ideal. However, it is important to recognize that while addressing malnutrition in women on a broader scale, body image concerns and eating disorders are typically more prevalent in rich women is a false stereotype and that nutritional disorders can be present across a wide range of socioeconomic backgrounds47.
Strengths and limitations of the study
This study has strengths. The large sample of 743,494 reproductive-age (15–49 years) women from ten Asian countries allowed us to examine PAFs for key risk factors and analyse interaction between education and wealth on obesity.
This study also had limitations. First, the use of cross-sectional data presents difficulties in establishing a temporal relationship between covariates and the outcome variable. Second, BMI as a measure of obesity does not reflect the location or amount of body fat of women. However, studies suggest that BMI is correlated to more direct measures of body fat, such as underwater weighing and dual-energy x-ray absorptiometry48. Third, we used WHO BMI cut-offs (< 18.5, 25–29.9 and ≥ 30 kg/m2) to categorize underweight, overweight and obesity. However, this cut-off may not be equally applicable across different populations due to differences in body composition and stature49. Forth, we merged widowed or divorced women as formerly married and did not test their independent association with obesity as there might be strong socio-cultural implications of these factors for women in traditional societies50.
Fifth, the study was limited by a lack of data on key behavioural factors, including dietary habit and physical activity, as the DHS did not collect information on these variables. Sixth, most of the explanatory variables were measured based on self-reported questionnaires and which could be a source of recall bias. Last, PAF estimates rely on particular assumptions, involving causality, the independence of modifiable risk factors, and consistent associations over time51. However, these assumptions might prove unrealistic due to the intricate interplay of socio-economic, cultural, healthcare, and behavioural factors associated with women’s nutritional status. Despite this complexity, PAFs offer a straightforward and intuitive metric that can supplement other methodologies in pinpointing modifiable risk factors suitable for policy intervention.
Conclusion
Central and Southeast Asian countries are experiencing a rising trend in female obesity, accompanied by a gradual reduction in underweight. A total of 73.3% of obesity among reproductive age women was associated with being married, age ≥ 35 years, residing in rich households, regular television watching and living in urban areas. Completing secondary or higher level of education exhibits a lower risk of obesity, particularly in wealthy households. Considering the increasing rate of urbanization in Asia, future interventions to prevent obesity should prioritize women in urban areas, particularly those residing in affluent households, with lower educational attainment, and engaging in unhealthy eating habits and physical inactivity. Preventing obesity should be a regional priority if SDG target 3.4 is to be achieved by 2030. Pakistan and the Maldives need to be a priority given the rapidly increasing trends in obesity and underweight subpopulations in their respective countries.
Data availability
The datasets supporting the conclusions of this article are available in the DHS repository, [https://dhsprogram.com/data/available-datasets.cfm]. The DHS provides open access to survey data files for legitimate academic research purposes. To initiate the download process, registration is mandatory. Researchers are required to provide their contact information, research title, and a brief description of the proposed analysis. Approval for dataset access is typically confirmed via email. It is important to note that these datasets are third-party resources and not under the ownership or collection of the authors, who possess no special access privileges.
Abbreviations
- BMI:
-
Body Mass Index
- CI:
-
Confidence interval
- DHS:
-
Demographic health survey
- ICF:
-
Inner city fund
- LMICs:
-
Low- and middle-income countries
- MEASURE:
-
Monitoring and evaluation to assess and use results
- NCDs:
-
Non-communicable diseases
- OR:
-
Odds ratio
- PAF:
-
Population attributable fraction
- SDG:
-
Sustainable development goals
- USAID:
-
United States Agency for International Development
- WOF:
-
World obesity federation
References
Abarca-Gómez, L. et al. Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to 2016: A pooled analysis of 2416 population-based measurement studies in 128· 9 million children, adolescents, and adults. Lancet. 390, 2627–2642 (2017).
Lobstein, T., Brinsden, H. & Neveux, M. World obesity atlas 2022. (2022).
Nugent, R., Levin, C., Hale, J. & Hutchinson, B. Economic effects of the double burden of malnutrition. Lancet. 395, 156–164. https://doi.org/10.1016/S0140-6736(19)32473-0 (2020).
Wells, J. C. et al. The double burden of malnutrition: Aetiological pathways and consequences for health. Lancet. 395, 75–88. https://doi.org/10.1016/S0140-6736(19)32472-9 (2020).
Mu, L. et al. Obesity prevalence and risks among Chinese adults: Findings from the China PEACE million persons Project, 2014–2018. Circ. Cardiovasc. Qual. Outcomes. 14, e007292. https://doi.org/10.1161/CIRCOUTCOMES.120.007292 (2021).
Aekplakorn, W. et al. Trends in obesity and associations with education and urban or rural residence in Thailand. Obesity. 15, 3113–3121. https://doi.org/10.1038/oby.2007.371 (2007).
Seferidi, P., Hone, T., Duran, A. C., Bernabe-Ortiz, A. & Millett, C. Global inequalities in the double burden of malnutrition and associations with globalisation: A multilevel analysis of Demographic and Health Surveys from 55 low-income and middle-income countries, 1992–2013;2018. Lancet Glob. Health10, e482-e490, doi:10.1016/S2214-109X(21)00594-5 (2022).
Biswas, T., Magalhaes, R. J. S., Townsend, N., Das, S. K. & Mamun, A. Double burden of underweight and overweight among women in South and Southeast Asia: A systematic review and meta-analysis. Adv. Nutr.11, 128–143. https://doi.org/10.1093/advances/nmz078 (2020).
Biswas, T. et al. Current progress and future directions in the double burden of malnutrition among women in South and Southeast Asian countries. Curr. Developments Nutr.3, nzz026 (2019).
Biswas, T., Townsend, N., Magalhaes, R., Hasan, M. M. & Mamun, A. A. Geographical and socioeconomic inequalities in the double burden of malnutrition among women in Southeast Asia: A population-based study. Lancet Reg. Health Southeast. Asia. 1, 100007. https://doi.org/10.1016/j.lansea.2022.04.003 (2022).
WHO (Geneva Switzerland) (2016).
Neuman, M., Kawachi, I., Gortmaker, S. & Subramanian, S. V. Urban-rural differences in BMI in low- and middle-income countries: The role of socioeconomic status. Am. J. Clin. Nutr.97, 428–436. https://doi.org/10.3945/ajcn.112.045997 (2013).
Kundu, D. & Pandey, A. K. In: Developing National Urban Policies (eds Debolina Kundu, Remy Sietchiping, & Michael Kinyanjui) Ch. Chapter 2, 13–49Springer Nature Singapore, (2020).
Rob, U. & Talukder, M. N. Urbanization prospects in Asia: A six-country comparison. Int. Q. Community. Health Educ.33, 23–37 (2013).
Collaboration, N. C. D. R. F. Rising rural body-mass index is the main driver of the global obesity epidemic in adults. Nature. 569, 260–264. https://doi.org/10.1038/s41586-019-1171-x (2019).
Aekplakorn, W. et al. Trends in obesity and associations with education and urban or rural residence in Thailand. Obes. (Silver Spring). 15, 3113–3121. https://doi.org/10.1038/oby.2007.371 (2007).
Poole, C. A history of the population attributable fraction and related measures. Ann. Epidemiol.25, 147–154. https://doi.org/10.1016/j.annepidem.2014.11.015 (2015).
Haire-Joshu, D. & Tabak, R. Preventing obesity across generations: Evidence for early life intervention. Annu. Rev. Public. Health. 37, 253–271. https://doi.org/10.1146/annurev-publhealth-032315-021859 (2016).
Corsi, D. J., Neuman, M., Finlay, J. E. & Subramanian, S. V. Demographic and health surveys: A profile. Int. J. Epidemiol.41, 1602–1613. https://doi.org/10.1093/ije/dys184 (2012).
WHO. Overweight and obesity, (2018). https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight
Program, T. D. Wealth Index Construction (2016). https://www.dhsprogram.com/topics/wealth-index/Wealth-Index-Construction.cfm
Vyas, S. & Kumaranayake, L. Constructing socio-economic status indices: How to use principal components analysis. Health Policy Plan.21, 459–468. https://doi.org/10.1093/heapol/czl029 (2006).
Ahmed, K. Y. et al. Factors associated with underweight, overweight, and obesity in reproductive age Tanzanian women. PLoS One. 15, e0237720. https://doi.org/10.1371/journal.pone.0237720 (2020).
Tareke, A. A. & Abate, M. G. Nutritional paradox in Ethiopian women: Multilevel multinomial analysis. Clin. Nutr. ESPEN. 36, 60–68. https://doi.org/10.1016/j.clnesp.2020.02.005 (2020).
Peugh, J. L. A practical guide to multilevel modeling. J. Sch. Psychol.48, 85–112. https://doi.org/10.1016/j.jsp.2009.09.002 (2010).
Ahmad, K., Rasmus Oestergaard, N. & Mohammad Ali, M. Methods matter: Population attributable fraction (PAF) in sport and exercise medicine. Br. J. Sports Med.54, 1049. https://doi.org/10.1136/bjsports-2020-101977 (2020).
Miettinen, O. S. Proportion of disease caused or prevented by a given exposure, trait or intervention. Am. J. Epidemiol.99, 325–332. https://doi.org/10.1093/oxfordjournals.aje.a121617 (1974).
Ogbo, F. A., Page, A., Idoko, J. & Agho, K. E. Population attributable risk of key modifiable risk factors associated with non-exclusive breastfeeding in Nigeria. BMC Public. Health. 18, 247. https://doi.org/10.1186/s12889-018-5145-y (2018).
Wilson, L. F. et al. Population attributable risk of modifiable risk factors associated with invasive breast cancer in women aged 45–69 years in Queensland, Australia. Maturitas. 76, 370–376. https://doi.org/10.1016/j.maturitas.2013.09.002 (2013).
Sue See, R. et al. Potentially modifiable dementia risk factors in all australians and within population groups: An analysis using cross-sectional survey data. Lancet Public. Health. 8, e717–e725. https://doi.org/10.1016/S2468-2667(23)00146-9 (2023).
Bonett, D. G. & Price, R. M. Inferential methods for the Tetrachoric correlation coefficient. J. Educational Behav. Stat.30, 213–225. https://doi.org/10.3102/10769986030002213 (2016).
Okunogbe, A., Nugent, R., Spencer, G., Ralston, J. & Wilding, J. Economic impacts of overweight and obesity: Current and future estimates for eight countries. BMJ Glob Health. 6, e006351. https://doi.org/10.1136/bmjgh-2021-006351 (2021).
Vuik, S., Lerouge, A., Guillemette, Y., Feigl, A. & Aldea, A. The economic burden of obesity. (2019).
Sturmberg, J. P. In: Health System Redesign Ch. Chapter 11, 213–232 (Springer International Publishing), (2018).
Joranli, K. T., Vefring, L. T., Dalen, M., Garnweidner-Holme, L. & Molin, M. Experiences of social support by participants with morbid obesity who participate in a rehabilitation program for health-behavior change: A qualitative study. BMC Nutr.9, 149. https://doi.org/10.1186/s40795-023-00810-0 (2023).
Aitsi-Selmi, A. et al. Interaction between education and household wealth on the risk of obesity in women in Egypt. PLoS One. 7, e39507. https://doi.org/10.1371/journal.pone.0039507 (2012).
Leroy, J. L., Habicht, J. P., Gonzalez de Cossio, T. & Ruel, M. T. Maternal education mitigates the negative effects of higher income on the double burden of child stunting and maternal overweight in rural Mexico. J. Nutr.144, 765–770. https://doi.org/10.3945/jn.113.188474 (2014).
Zhou, M. The shifting income-obesity relationship: Conditioning effects from economic development and globalization. SSM Popul. Health. 15, 100849. https://doi.org/10.1016/j.ssmph.2021.100849 (2021).
Aitsi-Selmi, A., Bell, R., Shipley, M. J. & Marmot, M. G. Education modifies the association of wealth with obesity in women in middle-income but not low-income countries: An interaction study using seven national datasets, 2005–2010. PLoS One. 9, e90403. https://doi.org/10.1371/journal.pone.0090403 (2014).
Si, W. Higher education expansion and gender norms: Evidence from China. J. Popul. Econ.35, 1821–1858. https://doi.org/10.1007/s00148-022-00888-z (2022).
Ford, N. D., Patel, S. A. & Narayan, K. M. Obesity in low- and Middle-Income countries: Burden, drivers, and emerging challenges. Annu. Rev. Public. Health. 38, 145–164. https://doi.org/10.1146/annurev-publhealth-031816-044604 (2017).
Nakamura, T. et al. Relationship between socioeconomic status and the prevalence of underweight, overweight or obesity in a General Japanese Population: NIPPON DATA2010. J. Epidemiol.28 (Suppl 3), S10–S16. https://doi.org/10.2188/jea.JE20170249 (2018).
Sabanayagam, C., Shankar, A., Saw, S. M., Tai, E. S. & Wong, T. Y. The association between socioeconomic status and overweight/obesity in a malay population in Singapore. Asia Pac. J. Public. Health. 21, 487–496. https://doi.org/10.1177/1010539509343957 (2009).
Raghupathi, V. & Raghupathi, W. The influence of education on health: An empirical assessment of OECD countries for the period 1995–2015. Arch. Public. Health. 78, 20. https://doi.org/10.1186/s13690-020-00402-5 (2020).
Menon, S. & Penalvo, J. L. Actions targeting the double burden of malnutrition: A scoping review. Nutrients 12, doi: (2019). https://doi.org/10.3390/nu12010081
McLaren, L. & Kuh, D. Women’s body dissatisfaction, social class, and social mobility. Soc. Sci. Med.58, 1575–1584. https://doi.org/10.1016/S0277-9536(03)00209-0 (2004).
Huryk, K. M., Drury, C. R. & Loeb, K. L. Diseases of affluence? A systematic review of the literature on socioeconomic diversity in eating disorders. Eat. Behav.43, 101548. https://doi.org/10.1016/j.eatbeh.2021.101548 (2021).
Romero-Corral, A. et al. Accuracy of body mass index in diagnosing obesity in the adult general population. Int. J. Obes. (Lond). 32, 959–966. https://doi.org/10.1038/ijo.2008.11 (2008).
Pray, R. & Riskin, S. The history and faults of the body Mass Index and where to look next: A literature review. Cureus. 15, e48230. https://doi.org/10.7759/cureus.48230 (2023).
Teachman, J. B. & Weight Marital status, and changes in Marital Status. J. Fam Issues. 37, 74–96. https://doi.org/10.1177/0192513X13508404 (2016).
Eide, G. E. Attributable fractions for partitioning risk and evaluating disease prevention: A practical guide. Clin. Respir J.2 (Suppl 1), 92–103. https://doi.org/10.1111/j.1752-699X.2008.00091.x (2008).
Acknowledgements
The authors are grateful to Measure DHS, ICF International, Rockville, MD, USA, for providing the data for analysis.
Funding
This study received no grant from any funding agency in public, commercial or not for profit sectors.
Author information
Authors and Affiliations
Contributions
ST conceptualized the study, obtained the data, had full access to the dataset, and takes responsibility for the integrity and accuracy of the data analysis. Concept and design: ST, KYA, AGR; Acquisition, analysis, or interpretation of data: ST, KYA, HMB, BC, MMH, AGR; Drafting of the manuscript: ST, KYA, AGR; Critical review of the manuscript for important intellectual content: All authors; Statistical analysis: ST, KYA, HMB, BC, MMH; Administrative, technical, or material support: ST, AGR; Supervision: AGR. All authors have read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Thapa, S., Ahmed, K.Y., Bizuayehu, H.M. et al. Trends and social determinants of the obesity epidemic among reproductive-age women in ten Asian countries. Sci Rep 14, 22545 (2024). https://doi.org/10.1038/s41598-024-73522-5
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-024-73522-5
Keywords
This article is cited by
-
Worldwide burden and cross-regional health inequalities of high BMI-attributable colorectal cancer by gender from 1990 to 2021, with predictions through 2041
BMC Gastroenterology (2025)
-
Global burden and trend of rheumatic heart disease among women of childbearing age, 1990–2021, with projection to 2040
BMC Cardiovascular Disorders (2025)
