
Abstract
To compare the economic burden of disease and quality of life in patients with premature ejaculation (PE) and erectile dysfunction (ED). A convenience sampling method was used, and self-designed general information questionnaire, disease economic burden questionnaire, and SF-12 quality of life questionnaire were used to investigate 494 patients with ED and 285 patients with PE who attended a tertiary hospital in Taiyuan City from October 2021 to May 2023, and the relevant data were analysed using SPSS26.0 statistical software. The direct, indirect, intangible, and total economic burdens of the two groups were compared, and the differences were statistically significant (P < 0.05), and the direct, indirect, intangible, and total economic burdens of ED patients were higher than those of PE patients; the scores of the two groups in the dimensions of PF (physical function), RP (role physical), RE (role emotion), and MH (mental health) as well as in the MCS (mental component score), and overall quality of life scores, the differences were statistically significant (P < 0.05), with ED patients having lower quality of life scores than PE patients. Compared with PE patients, ED patients have a heavier economic burden of disease and lower quality of life, suggesting that the government and relevant departments of society should pay attention to the economic burden of disease and quality of life of ED patients and take appropriate measures to improve them.
Similar content being viewed by others
Premature ejaculation (PE) and erectile dysfunction (ED) are the most common sexual dysfunctions in men. PE is mainly defined as ejaculation that often or always occurs before or within approximately 1 min after vaginal penetration (primary premature ejaculation) or a significantly shorter intravaginal ejaculatory latency of less than 3 min (secondary premature ejaculation) from the time of first sexual intercourse, and is always or almost impossible to control and delay ejaculation, and is accompanied by negative physical and psychological effects, such as distress, anxiety, frustration, and low self-esteem1. ED is defined as the inability of the penis to achieve or maintain a sufficient erection for satisfactory sexual intercourse with onset greater than three months, and can be categorised mainly as organic, psychological and mixed ED2. The prevalence of PE and ED has been increasing in recent years, and studies have shown that the global prevalence of PE in men is as high as 20–30%3, and the prevalence of ED is as high as 10–48%4,5. In addition, PE and ED are often combined6. Several evidence and meta-analysis studies showed that the comorbidity of ED and PE could be up to 50%7. However, PE and ED have never been considered as a unified clinical disorder before. Colonnello, E. et al.8 proposed and defined a new classification of clinical disorders of subclinical PE (SPE) and loss of control of erection and ejaculation (LCEE) as a way to improve the clinical management of PE and comorbidities in men. The economic burden of disease refers to the sum of economic losses and consumed resources brought by disease, disability (incapacity) to the society, family, and patients9, including direct, indirect, and intangible economic burdens. The etiology of PE and ED is complex, the treatment cycle is long, and it has a chronic lifelong characteristic. Moreover, their treatment modalities are complex, causing a serious disease burden for patients; Meanwhile, the majority of men take sexual ability, sexual function as a manifestation of their masculinity, and once suffering from PE or ED, they may suffer from physical, psychological, partner, social, and economic blows10,11, which seriously threaten their physical and mental health and quality of life. Milenkovic U et al.12 have shown that the treatment of ED is extremely complex. And because the rising cost of healthcare due to ED poses a serious threat to the viability of the healthcare system, healthcare payers will resort to excluding certain treatments from insurance coverage to cope with the rising costs. This will undoubtedly significantly increase the burden of disease for people with ED. In addition, a global burden of disease study showed that in the United States, overall work productivity impairment was approximately 2.11 times greater for men with ED than for men without ED; men with ED had higher rates of absenteeism and work productivity loss compared to men without ED13,14. Besides, men with PE and ED have reduced quality of life15,16. Balon, R17. showed that men with PE had better overall health than men with ED, and the numbers of burdened individuals would be higher in the lower age cohort of patients with PE compared to the same age cohort of men with ED.
Currently, most studies on PE and ED focus on disease diagnosis and treatment, emotional and psychological aspects, and there are fewer comparative studies on the economic burden of disease and quality of life of patients with PE and ED. Therefore, the purpose of this study is to conduct a comparative analysis of the current situation of the economic burden of disease and quality of life of patients with PE and ED in order to understand the current situation of the economic burden of disease and quality of life of patients with PE and ED, and to provide a reference basis for the decision-making departments of medical and health care to improve the relevant social security system.
Materials and methods
General information
A questionnaire survey of ED patients and PE patients attending a tertiary hospital in Taiyuan City, Shanxi Province, China, from October 2021 to May 2023 was conducted using convenience sampling. Inclusion criteria: (1) Meet the clinical diagnostic criteria of PE or ED18,19; The cases involved in this article were diagnosed as PE or ED by a male physician through history questioning, physical examination, laboratory tests, and special investigations. Laboratory tests included serological tests and sex hormone tests, etc. Special tests include erectile nerve examination, nocturnal penile distension test (NPTR) or audio-visual stimulation penile stiffness test (AVSS), and ultrasound. (2) Age ≥ 18 years old; (3) Voluntary cooperation with the survey, cognitive and behavioral ability is intact. Exclusion criteria: (1) those who did not cooperate during the survey and had a low response rate; (2) those who had a combination of PE and ED diseases; (3) those who had cognitive dysfunction.
This is a cross-sectional survey study and the sample size formula used is as follows:\(\:\text{N}=\frac{{{{\upmu\:}}^{2}}_{{\upalpha\:}/2}{\uppi\:}(1-{\uppi\:})}{{{\updelta\:}}^{2}}\). In the formula, N is the sample content. π is the estimate of the overall rate. δ is the permitted error, which is the difference between the sample rate and the overall rate. Referring to the relevant studies of Chinese scholars, in which the survey results showed that the prevalence of ED in Chinese men was 43.4%, and the prevalence of PE was 9.5%20,21. The test level α = 0.05, µ0.05/2 = 1.96, and the permitted error δ = 0.05. Sample is needed to take into account the possibility of incomplete data, low response rate, and unqualified information in the survey process, and increase the sample size by 20 per cent. After calculation, the sample size of PE and ED can be obtained as 158 and 452 cases respectively. A total of 285 PE patients and 494 ED patients were effectively investigated in this study respectively, indicating an adequate sample size.
The study was approved by the Ethics Committee of Shanxi University of Traditional Chinese Medicine (2022LL095), and the subjects volunteered to participate in the study and signed an informed consent form. This study was conducted based on the Declaration of Helsinki.
Methods and scales
Methods of investigation
After obtaining informed consent from the patients, a self-designed general information questionnaire, a questionnaire on the economic burden of disease, and the SF-12 Quality of Life Questionnaire were used to survey the patients.
Survey questionnaire
General information questionnaire: specifics include age, domicile, marriage status, education status, occupation, combined disease (combined disease mainly refer to the presence or absence of hypertension, diabetes mellitus, dyslipidaemia, prostatitis, prostatic hyperplasia, and other sexual dysfunction disorders in addition to PE and ED), personal monthly income, and receiving treatment time (receiving treatment time is mainly the time the patient has spent treating the disease or controlling its progression through medication, surgery, psychological and physical therapy from the first visit for the disease to the present).
Disease economic burden questionnaire: the specific content includes relevant outpatient costs, travel costs, food and accommodation costs, nutritional costs, and the number of days missed by the patient and accompanying staff. Among them, the direct economic burden in this study consisted of direct medical costs (consultation and treatment costs, laboratory and examination costs, and drug costs) and direct non-medical costs (travel, accommodation, food and nutritional costs), which were calculated using the distribution modeling method22; the indirect economic burden consisted of lost wages for patients and their companions, which were calculated using the human capital method23; The intangible economic burden refers to the pain, sorrow and inconvenience suffered by patients and their family members as a result of the disease and the resulting reduction in the quality of life or other costs incurred as a result of related illnesses caused by the disease24; in this study, intangible economic burden was assessed using the willingness-to-pay method and the competitive bidding method25.
SF-12 Quality of Life Survey Scale26: the scale consists of two parts, Physical Component Score (PCS) and Mental Component Score (MCS), including 12 entries and eight dimensions, which are General Health (GH), Physical Function (PF), Role Physical (RP), Bodily Pain (BP), Mental Health (MH), Vitality (VT), Social Function (SF), and Role Emotion (RE). The PCS total score was calculated from four entries, GH, PF, RP, and BP, and the MCS total score was calculated from four entries, SF, RE, MH, and VT. Scale scores were calculated according to a uniform standard, and the range of scores for each latitude was 0-100, with higher scores indicating higher quality of life.
Statistical analysis
SPSS26.0 statistical software was used to perform relevant descriptive analysis, t-test, and χ2 test on the data, and P < 0.05 indicated that the difference was statistically significant.
Results
Comparison of general data of patients with PE and ED
A total of 285 PE patients with a mean age of (33.90 ± 8.37) years and 494 ED patients with a mean age of (33.11 ± 8.19) years were collected in this study; as shown in Table 1, the differences between the two groups were statistically significant in terms of education status, personal monthly income, knowledge of sexual and reproductive health, friends, family support, occupational/partner relationship stress, and receiving treatment time (P < 0.05); the differences were not statistically significant in terms of age, domicile, marriage status, occupation, and combined disease (P > 0.05).
Comparison of the economic burden of disease in patients with PE and ED
As shown in Table 2, the direct economic burden for PE patients was 1901.41 (1309.88, 3973.88) yuan, the indirect economic burden was 1058.20 (793.65, 1587.30) yuan, the intangible economic burden was 2000.00 (800.00, 4500.00) yuan, and the total economic burden was 6719.40 (4154.64, 10241.22) yuan. As shown in Table 3, the direct economic burden for ED patients was 3583.31 (1740.39, 11235.72) yuan, the indirect economic burden was 1587.30 (793.65, 3174.60) yuan, the intangible economic burden was 4500.00 (2000.00, 8500.00) yuan, and the total economic burden was12717.68 (6512.97, 22493.61) yuan. As shown in Table 4, the direct, indirect, intangible, and total economic burdens of the two groups were all statistically significant when compared (P < 0.05), and the direct, indirect, intangible, and total economic burdens of ED patients were higher than those of PE patients.
Comparison of quality of life between PE and ED patients
As shown in Table 5, PE patients had the highest scores on the PF dimension (86.05 ± 21.92) and the lowest scores on the GH dimension (42.02 ± 14.38), and ED patients had the highest scores on the PF dimension (93.22 ± 15.75) and the lowest scores on the RE dimension (31.38 ± 28.08). The scores of PF, RP, RE, and MH dimensions, as well as MCS and overall quality of life scores, were statistically significant in both groups (P < 0.05); and the scores of PF dimensions in PE patients were lower than those in ED patients, and the scores of RP, RE, and MH dimensions, as well as MCS and overall quality of life scores in PE patients were higher than those in ED patients; and the quality of life scores in PE patients were higher compared with those in ED patients were higher. There was no statistically significant difference in the scores of GH, BP, VT, SF dimensions and PCS scores between the two groups of patients (P > 0.05).
Discussion
General condition of patients with PE and ED
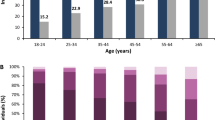
The results of this study showed that most of the patients in both groups were located in the age range of 18–39 years old, and most of them were young patients, accounting for about 80% of the patients. And most of the patients in the two groups are married. It shows that with the accelerated pace of modern life, the pressure on men from work, family and society gradually increases, which makes male sexual dysfunction diseases gradually show a younger trend, and more and more young men suffer from sexual dysfunction diseases27,28. In addition, this study showed that the educational level of PE patients was equally distributed among junior high school and below (21.4%), high school or junior college (22.1%), college (28.1%), and bachelor’s degree and above (28.4%), whereas the educational level of ED patients was mainly concentrated in bachelor’s degree and above (36.6%). Studies have shown that a lack of sexual and reproductive health knowledge can cause men to deny their sexuality, repress erectile reflexes and sexual urges, and thus cause ED29. The percentage of ED patients with bachelor’s degree and above in this study was higher than that of PE patients though. However, the percentage of PE patients with better sexual and reproductive health knowledge status was 16.5%, which was significantly higher than that of ED patients (13.4%). In addition, another study of sexual and reproductive health literacy among 1946 college students found that male college students generally had lower levels of sexual and reproductive health knowledge than women30. It shows that many men are not too concerned about sexual health in their daily life. Their sexual and reproductive health knowledge education is insufficiently acquired. And they have less knowledge and understanding of sexual and reproductive health knowledge and sexual dysfunction diseases.
Economic Burden of Disease in patients with PE and ED
The prevalence of male sexual dysfunction has been on a gradual rise in recent years, and more and more men are facing the threat of PE or ED. PE, ED belongs to the chronic male diseases, the course of the disease is long, easy to recur, in the short term can not be cured, the need for long-term adherence to medication. In addition PE, ED may also have an impact on men’s work productivity, attendance and activity impairment13,14,31, causing serious disease burden and existential stress to patients and their families. The results of this study showed that the mean total economic burden of PE patients was 8717.95 yuan, which accounted for 8.5% and 21.5% of the per capita gross domestic product (102,922) and per capita disposable income (40,597) of Taiyuan City, Shanxi Province, China, in 2022, respectively. The mean total economic burden of ED patients was 16,840.04 yuan, which accounted for 16.4% and 41.5% of the gross domestic product per capita (102,922) and disposable income per capita (40,597)32 in Taiyuan, Shanxi Province, China, in 2022, respectively; And when comparing the total direct, indirect, intangible, and economic burdens of the two groups, PE patients were lower than ED patients, indicating that ED patients faced a more severe economic burden of disease than PE patients. This study showed that the population of ED patients with incomes of 5001 yuan to 10,000 yuan and 10,000 yuan or more accounted for 35.6% and 4.9% of the population, respectively, which were less than that of PE patients (41.1% and 8.4%). This suggests that the population of ED patients in this study had lower income than PE patients; In addition, the percentage of ED patients in this study who received a treatment cycle of less than six months was 65%, which was more than that of PE patients (29.5%), and the percentage of patients who received a treatment cycle of more than two years was 10.1%, which was lower than that of PE patients (22.5%). However, the financial burden of disease for ED patients is still higher than that for PE patients, probably because ED involves higher costs of examination, medication, and treatment than PE, which leads to a heavier financial burden of disease for ED patients.
Quality of life of PE and ED patients
Several global studies have shown that sex is an important part of a man’s life33. Once a man suffers from sexual dysfunction, the quality of his sexual life, sexual health and sexual harmony between partners are seriously undermined, and the relationship between husband and wife and family stability are seriously threatened. At the same time, under the influence of traditional culture and gender roles, men’s self-esteem is undermined and they are prone to negative psychology, such as feelings of shame, inferiority, anxiety and depression. These create a huge burden of thought and mental stress on men, thus causing serious damage to men’s psychosocial and emotional health and quality of life34,35. The results of this study showed that both groups of patients had the highest scores on the SF-12 scale in the PF dimension, probably because most of the patients in both groups were young patients with their own physiological functioning. In addition, the SF-12 scale scores in the RP, RE, and MH dimensions as well as the MCS and overall quality of life scores were higher in PE patients than in ED patients, suggesting that the quality of life of ED patients was lower than of PE patients. This study showed that the percentage of ED patients with high occupational/partner relationship stress was 54.3%, which was significantly higher than that of PE patients (37.2%). This may be due to the fact that ED is defined as the inability of the penis to become sufficiently erect to effectively enter the vagina to accomplish a satisfying sexual encounter. While PE means that the patient can have an erection and can enter the vagina smoothly, although the time is shorter, the man can help the woman to reach orgasm by doing good foreplay such as kissing and stroking, so that both parties can obtain sexual satisfaction36. As a result, ED patients face greater partner relationship stress compared to PE patients. This is because they are afraid that their poor state of sexual functioning will not be sufficient to complete their sexual life, which will trigger their partner’s contempt, ridicule, dissatisfaction and even leaving10; it also shows that although the percentage of good and full support from friends and family is higher in ED patients (42.9% and 51.2%) than in PE patients (21.4% and 20%), however, their stigma, psychological stress, and burden of self-feeling are heavier, so their quality of life is lower.
In addition, this study has certain limitations. For example, the sample size of PE and ED patients obtained from this study was relatively small; the sample sampling range was limited; and there were varying degrees of recall bias among the patients regarding the treatment process and the specific costs associated with the disease over a one-year period.Therefore, the sample size will be further expanded in the future and a more in-depth study will be conducted through a large-scale social face questionnaire to better serve the clinic.
Conclusion
In summary, patients with ED have a greater economic burden of disease and lower quality of life than patients with PE. This prompts the government and society to optimize the relevant support and protection system, and to consider including male sexual dysfunction diseases in the coverage of outpatient-related medical insurance, so as to alleviate patients’ financial burden of disease; at the same time, colleges and universities have increased the number of courses on sexual and reproductive health, and society has strengthened publicity and education to optimize the environment; in addition, clinical medical personnel should also be timely to patients and their partners on sexual dysfunction disease, sexual health-related knowledge information for popularization of science and education. Help patients to establish a good sexual cognition, to face “sex” with a positive and healthy attitude, seek medical help in time, eliminate negative emotions. This will enhance self-efficacy and psychological adjustment ability, and improve patients’ quality of life.
Data availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
References
Serefoglu, E. C. et al. An evidence-based unified definition of lifelong and acquired premature ejaculation: report of the second international society for sexual medicine ad hoc committee for the definition of premature ejaculation. J. Sex. Med. 2, 41–59 (2024).
Anna, K., Sam, S., Ben, C. & Karen, B. Mieke, V. The global prevalence of erectile dysfunction: a review. BJU Int. 124, 587–599 (2019).
Stanley, E. A. et al. An update of the International Society of Sexual Medicine’s guidelines for the diagnosis and treatment of premature ejaculation. J. Sex. Med. 2, 60–90 (2014).
Ferrini, M., Gonzalez-Cadavid, N. & Rajfer, J. Aging related erectile dysfunction-potential mechanism to halt or delay its onset. Transl Androl. Urol. 6, 20–27 (2017).
Mulhall, J., King, R., Glina, S. & Hvidsten, K. Importance of and satisfaction with sex among men and women worldwide: results of the global better sex survey. J. Sex. Med. 5, 788–795 (2008).
Cilio, S. et al. Premature ejaculation among men with erectile dysfunction—findings from a real-life cross-sectional study. Int. J. Impot. Res. 35, 558–563 (2023).
Fugl-Meyer, K. & Fugl-Meyer, A. R. Sexual disabilities are not singularities. Int. J. Impot. Res. 14, 487–493 (2002).
Colonnello, E., Ciocca, G., Limoncin, E., Sansone, A. & Jannini, E. Redefining a sexual medicine paradigm: subclinical premature ejaculation as a new taxonomic entity. Nat. Rev. Urol. 18, 115–127 (2021).
Musgrove, P. Investing in health: the 1993 world development report of the world bank. Bull. Pan Am. Health Organ. 27, 284–286 (1993).
Hartmann, U., Schedlowski, M. & Kruger, T. H. Cognitive and partner-related factors in rapid ejaculation: differences between dysfunctional and functional men. World J. Urol. 23, 93–101 (2005).
Cilio, S. et al. Unrecognised orgasmic phase disorders in men presenting with new-onset erectile dysfunction-findings from a real-life, cross-sectional study. Andrology 12, 606–612 (2024).
Milenkovic, U., Campbell, J., Roussel, E. & Albersen, M. An update on emerging drugs for the treatment of erectile dysfunction. Expert Opin. Emerg. Drugs 23, 319–330 (2018).
Jannini, E. A. et al. Health-related characteristics and unmet needs of men with erectile dysfunction: a survey in five European countries. J. Sex. Med. 11, 40–50 (2014).
Plumb, J. M. & Guest, J. F. Annual cost of erectile dysfunction to UK society. Pharmacoeconomics 16, 699–709 (1999).
Elterman, D. et al. The Quality of Life and Economic Burden of Erectile Dysfunction. Res. Rep. Urol. 13, 79–86 (2021).
Przydacz, M., Chlosta, M., Rajwa, P. & Chlosta, P. Population-level prevalence, effect on quality of life, and treatment behavior for erectile dysfunction and premature ejaculation in Poland. Sci. Rep. 13, 13168 (2023).
Balon, R. Burden of sexual dysfunction. J. Sex. Marital Ther. 43, 49–55 (2017).
Sharlip, I. Diagnosis and treatment of premature ejaculation—the physician’s perspective. J. Sex. Med. 2, 103–109 (2005).
McMahon, C. G. Current diagnosis and management of erectile dysfunction. Med. J. Aust. 210, 469–476 (2019).
Chen, W. et al. Meta-analysis of the prevalence of erectile dysfunction in Chinese men. Chin. Sex. Sci. 33, 12–18 (2024).
Du, H. et al. Analysis of factors affecting the sense of shame in patients with premature ejaculation and construction of a column-line diagram prediction model. Chin. J. Male Sci. 37, 69–74 (2023).
Robinson, L., Sarkies, M., Brown, T. & O’Brien, L. Direct, indirect and intangible costs of acute hand and wrist injuries: a systematic review. Injury 47, 2614–2626 (2016).
Burton, W. N., Conti, D. J., Chen, C. Y., Schultz, A. B. & Edington, D. W. The economic burden of lost productivity due to migraine headache: a specific worksite analysis. J. Occup. Environ. Med. 44, 523–529 (2002).
Dagenais, S., Caro, J. & Haldeman, S. A systematic review of low back pain cost of illness studies in the United States and internationally. Spine J. 8, 8–20 (2008).
Stavem, K. Association of willingness to pay with severity of chronic obstructive puhnonary disease, health status and other preference measures. Int. J. Tuberc. Lung Dis. 6, 542–549 (2002).
Jakobsson, U., Westergren, A., Lindskov, S. & Hagell, P. Construct validity of the SF-12 in three different samples. J. Eval. Clin. Pract. 18, 560–566 (2012).
Goldstein, I., Goren, A., Li, V., Tang, W. & Hassan, T. Epidemiology update of Erectile Dysfunction in eight countries with high burden. Sex. Med. Rev. 8, 48–58 (2020).
Nguyen, H., Gabrielson, A. & Hellstrom, W. Erectile Dysfunction in Young Men-A Review of the prevalence and risk factors. Sex. Med. Rev. 5, 508–520 (2017).
Wang, L. & Du, Y. Overview of erectile dysfunction in men. Chin. J. Soc. Med. 22, 162–165 (2005).
Santos, M. J., Ferreira, E. & Ferreira, M. Sexual and Reproductive Health Literacy in College Students. Eur. J. Public. Health. 29, 3–4 (2019).
Rasmussen, S., Balasubramaniam, K., Jarbol, D., Sondergaard, J. & Haastrup, P. Socioeconomic status and barriers for contacting the general practitioner when bothered by erectile dysfunction: a population-based cross-sectional study. BMC Fam. Pract. 21, 166 (2020).
Taiyuan Bureau of Statistics. Economic Performance of Taiyuan City in 2022.[ED/OL]. https://stats.taiyuan.gov.cn/sjjd/20230131/30018174.html
Lu, Y. et al. The decline in sexual function, psychological disorders (anxiety and depression) and life satisfaction in older men: a cross-sectional study in a hospital-based population. Andrologia 52, e13559 (2020).
Althof, S. E. Quality of life and erectile dysfunction. Urology 59, 803–810 (2022).
Hwang, I., Yang, D. O. & Park, K. Self-reported prevalence of and attitudes toward premature ejaculation in a community-based study of married couples. World J. Mens Health 31, 70–75 (2013).
Rowland, D. et al. Self- reported premature ejaculation and aspects of sexual functioning and satisfaction. J. Sex. Med. 1, 225–232 (2004).
Funding
This study was supported by 2023 Shanxi Provincial Colleges and Universities General Teaching Reform Innovation Project (No.J20230460).
Author information
Authors and Affiliations
Contributions
Y.F. and W.Z. wrote the main manuscript text. H.D. and J.Z. prepared figures and tables. Y.F. and W.Z. designed the study. J.Z. and H.D. collected and analysed the data. Y.F. wrote the manuscript. W.Z.critically revised the manuscript. Written informed consent was obtained from the patient for publication of thisstudy.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
This study was approved by the Ethics Committee of Shanxi University of Traditional Chinese Medicine. Written informed consent was obtained from each participant. This study was performed in accordance with the Declaration of Helsinki.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Fu, Y., Zhao, J., Zhang, W. et al. Comparison of economic burden of disease and quality of life in patients with premature ejaculation and erectile dysfunction. Sci Rep 14, 27374 (2024). https://doi.org/10.1038/s41598-024-78607-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-024-78607-9
